










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.12 no.4 Ribeirão Preto dez. 2016
http://dx.doi.org/10.11606/issn.1806-6976.v12i4p240-248
DOI: 10.11606/issn.1806-6976.v12i4p240-248
REVIEW ARTICLE
Integrative review of literature on the construction of Therapeutic Projects Singles in the mental health field1
Revisión integradora de la literatura en la construcción de proyectos terapéuticos singulares en el campo de la salud mental
Ana Laura Pires RodovalhoII; Renata Fabiana PegoraroIII
IIPsychology undergraduate course, Universidade Federal de Uberlândia, Uberlândia, MG, Brazil
IIIPhD, Adjunct Professor, Universidade Federal de Uberlândia, Uberlândia, MG, Brazil
ABSTRACT
We conducted an integrative review of literature on the construction and monitoring of Therapeutic Projects Singles by teams of mental health services. The survey was conducted in electronic databases Scielo, Redalyc and Pepsic between 2004 and 2014. We found 419 publications and 13 selected from the keywords: individual therapeutic projects, therapeutic projects singles, mental health, psychosocial care, reference technical center of psychosocial care, mental health services. The analysis of articles singles out four blocks of meaning: Who designs the project; Problems in the development; Relevance of the project; and their absence. The study points to difficulties in the inclusion of family members and users in the construction of therapeutic projects by the teams.
Descriptors: Mental Health; Mental Health Services; Patient Care Team.
RESUMEN
Hemos llevado a cabo una revisión integradora de la literatura sobre la construcción y el seguimiento de proyectos terapéuticos individuales por equipos de los servicios de salud mental. La encuesta se realizó en bases de datos electrónicas Scielo, Redalyc y Pepsic entre 2004 y 2014. Se ha encontrado 419 publicaciones y 13 seleccionados de las palabras clave: proyectos individuales singulares, salud mental, atención psicosocial, la referencia centro técnico de la atención psicosocial, servicios de salud mental. El análisis de los artículos destaca a cuatro bloques de significado: ¿Quién diseña el proyecto; Los problemas en el desarrollo; Relevancia del proyecto; y su ausencia. El estudio apunta a las dificultades en la inclusión de miembros de la familia y de los usuarios en la construcción de proyectos terapéuticos por los equipos.
Descriptores: Salud Mental; Servicios de Salud Mental; Grupo de Atención al Paciente.
Introduction
The "Singular Therapeutic Projects" (STP) are instruments developed by health teams to guide the comprehensive care to users. In the field of mental health, the STP is prepared by the teams for attention of users with severe and persistent mental illness and/or substance use, who carry out treatment in Psychosocial Care Centers in Brazil. Thus, it is an instrument aligned with current public policies of mental health in the country, which constitute an attempt to reverse the psychiatric ward and segregationist model that marked the psychiatric care in Brazil for a long time(1-2).
CAPS (Psychosocial Care Centers, in Portuguese) function in the "open door" model, that is, they were created to welcome and help all individuals with severe mental disorders who seek them, through a treatment by multidisciplinary team, so that such persons can be more autonomous and reinserted in their social and cultural environment. These institutions are placed in strategic areas, in several municipalities, so that the users are treated where they live(1).
CAPS offer daily service aiming actions to help each user according to their needs and respect their desire to learn and may involve education, work, sports, among others; predominantly with group workshops and activities. Each user receives multidisciplinary attention inside the CAPS. The teams are different in each of the CAPS modalities. In CAPS I, placed in municipalities of smaller population size, operate at least 1 psychiatric doctor or trained in mental health, 1 nurse, 3 top-level professionals (including psychologist) and 4 mid-level professionals; in CAPS II, there are 1 psychiatrist, 1 nurse with mental health training, 4 top-level professionals and 6 mid-level professionals; and for users of the CAPS III, which operates 24 hours/day, the minimum team is expected to be 2 psychiatrists, 1 nurse with mental health training, 5 top-level professionals and 8 mid-level professionals(1).
Professionals can be organized in reference teams, formed by several professionals from different fields who assist and monitor the user who goes to CAPS. Some CAPS have a single person, the Therapist of Reference or Reference Technician to closely monitor users, prepare and monitor their therapeutic projects(3-4).
The STP must respect the particularities of individuals by customizing "the service of every person in the unit and beyond," proposing activities such as workshops at times when the individual uses the service, respecting his/her wishes and needs(1).
In the STP, activities should be defined in the intensive, semi-intensive or non-intensive care modalities. Intensive Care is daily for those suffering from severe psychological distress, for those who are in crisis and/or for those that need ongoing attention due to intense difficulties. In the Semi-Intensive Care the subject is assisted in up to 12 days a month, and is usually for those in which suffering is decreasing, which enables better social relationship, but the person needs CAPS to develop greater autonomy. In Non-Intensive Care, the individual no longer needs the assistance of the teams as in the other cases, and can be assisted at most up to 3 days per month(1).
The STP preparation should occur from the relations between the user and the reference technician and reference team, always emphasizing the individuals, their family and their social context. Therefore, the STP should not be developed solely by the team. It is imperative that the team talks to the user and family members so that the STP is a targeted tool, open to change, but with defined objectives and evaluation of results(4-5). Thus, the subjects are seen beyond their disease, so that their participation in social media and their autonomy increase. It is therefore a unique strategy developed by the team to the user’s care.
The formation of the STP to CAPS users has as main purpose to avoid hospital admissions and promote the social reintegration of the subject. Its preparation begins with the welcome strategy, as in the process of listening to the user, the professional can identify aspects of the disease and the social context of the individual. From there, the team takes into account not only the difficulties of the individuals, to help him/her to overcome them, but also their abilities, desires and needs that can be worked in CAPS in order to create greater bond between team and user and show them the responsibility they have on their treatment and their choices(3).
From the recognition of the importance of developing STP for users of mental health services, the objective of this study was established in carry out an integrative literature review on the construction and monitoring of Singular Therapeutic Projects by teams of Psychosocial Care Centers.
Method
Integrative literature review was adopted to this study(6). From the guiding question "How are the Singular Therapeutic Projects constructed and monitored by teams of Psychosocial Care Centers in Brazil?", literature search was performed by the following criteria: (a) Inclusion criteria: theoretical articles (bibliographic research and essays), research reports and experience reports, publications of the last ten years (2004-2014) in Portuguese, in electronic databases Scielo, Redalyc and Pepsic, using keywords (alone and combined with AND): singular therapeutic projects, individual therapeutic projects, mental health, psychosocial care, reference technician, Psychosocial Care Center, mental health services; (B) Exclusion criteria: articles not written in Portuguese, editorials, reviews, news or letters from scientific journals, theses, monographs, dissertations, book chapters and books.
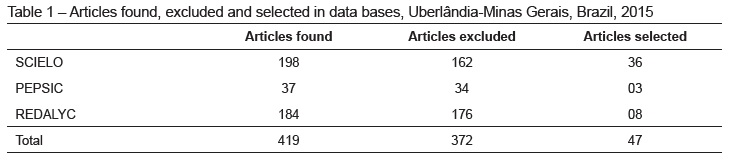
Searching electronic databases 419 articles were found, published between 2006 and 2014, in full text. From reading the titles and abstracts, articles published in other languages were eliminated (F=21), and articles that did not address the treated subject (F=346), and articles repeated in databases (F=5). A total of 372 articles were excluded and 47 were selected (Table 1).
From that number, the articles were completely read (F=47) to determine if they answered the guiding question of the study; those that answered the question constituted the corpus of analysis of this research: 13 articles, which were read in full and then extracted the following information, as directed by Broome(7): (a) year of publication; (b) source of publication; (c) type of study; (d) sample; (E) objectives and (f) the main results of each article. For increased reliability of the results, each researcher has prepared a spreadsheet and then the information was discussed and solidified in a single instrument. Furthermore, the level of evidence of each study was assigned(8). In the level of evidence some initial information are considered to present to the reader conditions to verify if the procedures are appropriate, in addition to demonstrate possible methodological flaws of the review.
Results
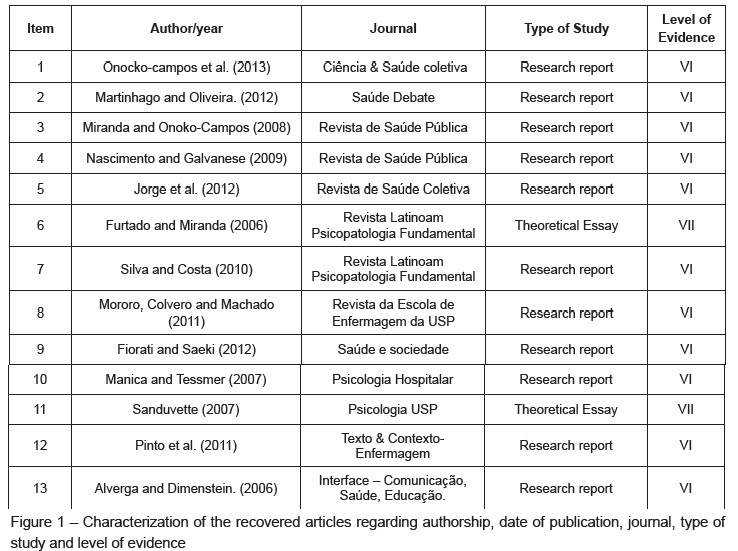
We covered 13 publications(9-21) from 2006 to 2013, most of which (F=7) from health care journals(9-13,17,21), and others(14-16,18-20) from psychology journals(18-19), psychopathology(14-15) and nursing(16,20).
We found 11 field research reports and two theoretical essays(14,19). The analysis of field research reports indicated that there was a predominance of research developed through group techniques (focus group, reflection, intervention and narrative) and individual interviews with CAPS III and CAPSi professionals, users, family members, service coordinators, Support Center for Family Health teams and outpatient care teams. Level of evidence VI was given to 11 articles reporting research for representing evidence from a single qualitative or descriptive study (Figure 1).
As for objectives, five articles had objectives directly related to the construction of the STP(16-17,20-21); the joint construction of the STP for services such as Support Center for Family Health, CAPS (Psychosocial Care Centers), outpatient care and primary care(17) and construction of STP solely by the CAPS team(16,20-21). The other articles analyzed the experiences of users linked to autonomous groups of medication(9,13), the perceptions of users, family members and professionals on teamwork(10-11), describe the physical structure and human resources of a CAPS(12) and work processes in a CAPS for children(18). One of the articles(19) had no objectives.
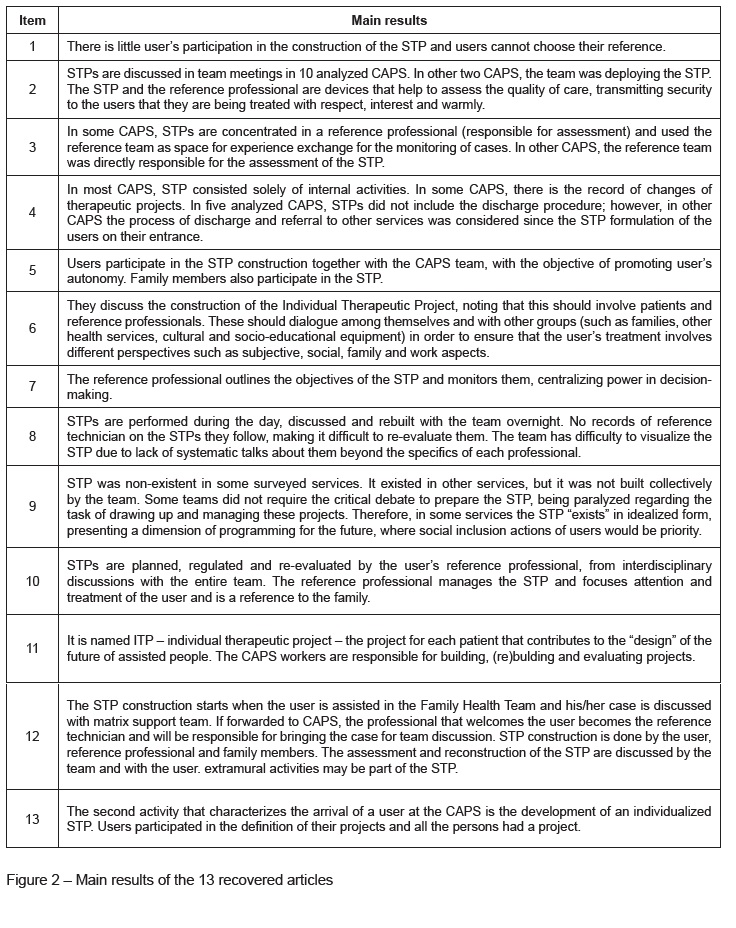
Figure 2 shows the main results of each recovered article. The analysis of articles identified four blocks of meaning, which are described below.
The first block of meaning refers to the producer of the STP. In the analyzed articles three possibilities were found: the development only by the reference technician(11,15), the joint development involving the user, family members, reference technician and the team(10,13-14,18,20-21), and initiate preparation, considering the user service in the Family Health Strategy (FHS), highlighting the need for user attention in the service network(20).
The second block of meaning refers to problems in the development of the STP selected in the articles. The first problem is the centralizing role of the Reference Technician (RT) which prepares and monitors the project without dialoguing with the other components of the service(9,11,15). This centralizing role is uncooperative to construct integral care, which is only possible through the exchange of knowledge made by different professionals in dialogue. It is noteworthy that, according to the articles when there is dialogue it is not always critical. The existence of a critical debate in teams is a practice considered as essential. The super-specialization of professionals who perform activities necessary to the service but without considering the STP as a whole has not yet been identified as a problem in the construction of STP(16-17). Team practice still stands as an issue the STP record, whether to update the project or to point out the possibility of user discharge(12).
The third block of meaning deals with the STP relevance. The first relevant point highlights the network role(14,20). Participation of different services for STP discussion, found in the articles, can be considered as an indication that Psychosocial Care Network has been working. In addition, the STP is understood as a project for the user’s future(17,19) and as an expression of Expanded Clinic.
Finally, the last block of meaning refers to the absence of STP in some CAPS investigated in one of the selected articles(17), showing a mismatch between psychosocial care, based on the expanded clinic, in the production of autonomy of subjects and construction of a comprehensive care.
Discussion
In this review, some publications addressed that the reference technician (RT) is the only person responsible for preparing the STP(11,15). On the one hand, it points to the RT importance; on the other hand, it shows little or no team participation in the development. The RT is considered a device(22) of bond promotion with the user, in which a specific professional of the team is chosen to assist a number of users, being responsible for monitoring and reassessing the project of each one of them.
However, this is not the only existing model. Some services adopt the arrangement of small team reference(23), that is, a part of the team becomes responsible for the production and monitoring of the STP, involving a larger number of professionals with the users’ project.
Developing the STP, starting from the dialogue between the RT and the team, as well as user and family members(10,13-14,18,20-21) points to the interdisciplinary importance of understanding the user’s needs and opportunity to create bonds, allowing that the care of the person in psychological distress is not done only from the perspective of the professional, but involving what is important from the perspective of the person himself/herself and the family(22).
It is necessary that the reference professional encourages active users’ participation in building their own STP, as this development enables the users to be agents to identify their difficulties and desires, developing more autonomy over their own trajectory(24).
The user’s path in the Center(20) must also be considered in the STP construction. First, by the integral Unified Health System concept(25) that defines a person as an indivisible whole and part of their community, which implies the recognition that the care points existing in the health system must be articulated to the promotion, protection and health recovery. Second, the existence of Psychosocial Care Network (RAPS, in Portuguese)(26) established by the Order MS/3088 of 2011, formed by services articulated to each other and belonging to different levels of primary, secondary and tertiary care. With the institutionalization of the Psychosocial Care Network, it is evident the need for dialogue between the health facilities towards the user care that is not associated with a single service. It is also worth highlighting as a problem in the construction of the STP the lack of the user’s participation, contrary to recommended by the Ministry of Health(24).
On the other hand, the notion of projectuality(27) was highlighted in the recovered literature(17,19). This concept highlights the importance of understanding the STP as a project for the user’s future. In this sense, the project is intended to create a space for reflection on new possibilities of existence and life(27) and not just to be seen as a grid or schedule of activities exposed to the user, indicating the days and weeks in which he should go to CAPS to do activities(22,27). When the STP is compared to a list of activities to be done by the user at CAPS it does not work as an instrument that can help the user to think about other possibilities of existence beyond the disease and diagnosis; in order to build a STP based in projectuality it is necessary to respect the steps for the construction of this instrument, namely: the diagnosis, setting objectives, the division of responsibilities in relation to tasks and the re-evaluation of the project(24,27). In the diagnosis the user should be considered as a complex being that has several dimensions (organic, psychological, social, and cultural) and uniqueness through this whole context. The definition of targets includes proposals agreed between the users and their professional of greater bond/RT. The responsibilities for task division imply that the entire team that takes care of the user must be included in the actions proposed in the project. Finally, a STP must include the revaluation, so that necessary modifications are made according to the individual’s evolution(24,27).
As can be seen, the STP is an instrument that allows the team to meet the interests of each user, allowing them to provide a more effective treatment in each case and activities that meet the users’ care needs, therefore, it is a tool to generate greater link between CAPS and user. However, the reality is that the user often fits what the service offers. Most health services organizations do not seek to form other groups or workshops for those who do not fit in any of the offered activities, either because the activities are not interested or do not contemplate the needs of customers(28). Therefore, one of the main objectives that support the logic of mental health services, that is, creating bonds between the user and CAPS, is difficult to be done.
The STP also appears as a possibility to perform Expanded Clinic(12), which is characterized by the management of professionals in an interdisciplinary way on the user’s care by promoting his/her understanding as a complex and autonomous being(22,24). By adopting the STP, the team takes responsibility for the meticulous care to every user as to his/her need and/or desire by seeking to develop bonds and joint actions towards life production. The resources to be adopted for a care in the expanded clinic perspective are multiple and must be chosen from the vulnerability of the case, its complexity and uniqueness, in view of the search for autonomy(22).
In addition, the expanded clinic implies the need for professional expertise and training detached from the biomedical model and drug interventions as center of attention to the user. Therefore, the practice should not fight the disease to find a cure but develop new possibilities of existence to the person in psychological distress(24). This perspective should involve therefore the users themselves and their family members in the project construction.
On that basis, it was found in the analyzed articles the prevalence of a traditional clinical structure, such as: no participation of the users in building their STP, the absence of discharge planning in the STP, the lack of external activities at CAPS, the super-specialization of care, the centralization of the project by the RT, and the lack of construction of the STP together with the team. These clinic characteristics in the more traditional sense point to a view of not comprehensive human beings more aligned to the biomedical health care model that emphasizes healing practices and does not understand the teamwork as essential. In psychosocial care services the biomedical model should not be a guiding of the team’s behavior(29-30).
In this regard, we stress that it is essential an ongoing assessment process of the functioning of CAPS and its alignment with health public policies and mental health(31), capable of leveraging changes not only in the form of care, but also to question the actions in the mental health field, allowing greater alignment to the psychosocial care field.
Final remarks
Considering that the objective of this study was to perform an integrative literature review on the construction and monitoring of Singular Therapeutic Projects by the teams of Psychosocial Care Centers, it has been reached. Thirteen publications have been identified from pre-defined selection and exclusion criteria, which pointed out that even with the STP services, this is not built from the identification of the user’s needs, setting of objectives, definition of professionals responsible for the actions and timing for project reassessment.
A limitation of this study is the small number of selected works, indicating that there is only one difficulty in building the STP, but also the need to expand the scientific debate on this issue, crucial to the functioning of psychosocial care services.
References
1. Ministério da Saúde (BR). Saúde mental no SUS: os centros de atenção psicossocial [Internet]. Brasília-DF; 2004 [Acesso 22 jul 2015]. Disponível em:: http://www.ccs.saude.gov.br/saude_mental/pdf/sm_sus.pdf. [ Links ]
2. Ministério da Saúde (BR). Reforma psiquiátrica e política de saúde mental no Brasil [Internet]. Brasília-DF; 2005 [cited 2014 abr 10]. Disponível em:: http://bvsms.saude.gov.br/bvs/publicacoes/Relatorio15_anos_Caracas.pdf. [ Links ]
3. Boccardo ACS, Zane FC, Rodrigues S, Mangia E. O projeto terapêutico singular como estratégia de organização do cuidado nos serviços de saúde mental. Rev Terapia Ocup Univ São Paulo. 2011;22(1):85-92. [ Links ]
4. Silva EA, Costa II. O profissional de referência em saúde mental: das responsabilizações ao sofrimento psíquico. Rev Latino-Am Psicopatol Fundamental. 2010;13(4):635-47. [ Links ]
5. Miranda FAC, Coelho EBS, More CLOO. Projeto terapêutico singular [Internet]. Florianópolis: Universidade Federal de Santa Catarina; 2012 [Acesso 03 jan 2016]. Disponível em: https://ares.unasus.gov.br/acervo/handle/ARES/1089 [ Links ]
6. Souza MT, Silva MD, Carvalho R. Integrative review: what is it? How to do it?. Einstein. 2010;8(1):102-6. [ Links ]
7. Broome ME. Integrative literature reviews in the development of concepts. In: Rodgers BL, Knafl KA, editores. Concept development in nursing: Foundations, techniques and applications. Philadelphia: Saunder; 2000. p. 231-50. [ Links ]
8. Pompeo DA, Rossi LA, Galvão CM. Integrative literature review: the initial step in the validation process of nursing diagnoses. Acta Paul Enferm. 2009;22(4):434-8. [ Links ]
9. Onocko-Campos RT, Passos E, Palombini AL, Santos SVD, Stefanello S, Gonçalves LLM et al. A Gestão Autônoma da Medicação: uma intervenção analisadora de serviços em saúde mental. Ciênc Saúde Coletiva. 2013;18(10):2889-98. [ Links ]
10. Martinhago F, Oliveira WFA. A prática profissional nos Centros de Atenção Psicossocial II (CAPS II), na perspectiva dos profissionais de saúde mental de Santa Catarina. Saúde Debate. 2012;36(95):583-94. [ Links ]
11. Miranda L, Onoko-Campos RT. Analysis of reference work in Psychosocial Care Centers. Rev Saúde Pública. 2008;42(5):907-13. [ Links ]
12. Nascimento AF, Galvanese ATC. Evaluation of psychosocial healthcare services in the city of São Paulo, Southeastern Brazil. Rev Saúde Pública. 2009;43(supl.1):8-15. [ Links ]
13. Jorge MSB, Campos RO, Pinto AGA, Vanconcelos MGF. Experiências com a gestão autônoma da medicação: narrativa de usuários de saúde mental no encontro dos grupos focais em centros de atenção psicossocial. Physis. 2012;22(4):1543-61. [ Links ]
14. Furtado JP, Miranda L. O dispositivo "técnicos de referência" nos equipamentos substitutivos em saúde mental e o uso da psicanálise winnicottiana. Rev Latino-Am Psicopatol Fundamental. 2006;9(3):508-24. [ Links ]
15. Silva EA, Costa II. O profissional de referência em Saúde Mental: das responsabilizações ao sofrimento psíquico. Rev Latino-Am Psicopatol Fundamental. 2010;13 (4):635-47. [ Links ]
16. Mororo MEML, Colvero LA, Machado AL. The challenges of comprehensive care in a Psychosocial Care Center and the development of therapeutic projects. Rev Esc Enferm USP. 2011;45(5):1171-6. [ Links ]
17. Fiorati RC, Saeki T. Projeto terapêutico nos serviços extra-hospitalares de saúde mental: uma reflexão crítica sobre a forma de elaboração e gestão dos projetos terapêuticos nos serviços. Saude Soc. 2012;21(3):587-98. [ Links ]
18. Manica G, Tessmer L. Terapeuta de referência: uma visão referenciada por profissionais da Saúde Mental. Psicol Hosp. 2007;5(2):1-23. [ Links ]
19. Sanduvette V. Sobre como e por que construir, (re)construir e avaliar projetos terapêuticos nos centros de atenção psicossocial (CAPS). Psicol USP. 2007;18(1):83-100. [ Links ]
20. Pinto DM, Jorge MSB, Pinto AGA, Vasconcelos MGF, Cavalcante CM, Flores AZT et al. Projeto terapêutico singular na produção do cuidado integral: uma construção coletiva. Texto Contexto-Enferm. 2011;20(3):493-502. [ Links ]
21. Alverga ER, Dimenstein M. A reforma psiquiátrica e os desafios na desinstitucionalização da loucura. Interface. (Botucatu). 2006;10(20):299-316. [ Links ]
22. Griogolo TM, Pappiani C. Clínica ampliada: recursos terapêuticos dos centros de atenção psicossocial de um município do norte de santa catarina. Cad Bras Saúde Mental. 2014;6(14):1-26. [ Links ]
23. Chaves BL, Pegoraro RF. Contribuições do arranjo "Equipe de Referência" a um Centro de Atenção Psicossocial. Estud Pesqui Psicol. 2013;13(3):939-56. [ Links ]
24. Ministério da Saúde (BR). Cartilha da PNH: Clínica ampliada, equipes de referência e projeto terapêutico singular [Internet]. Brasilia; 2008 [Acesso 20 mar 2015]. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/clinica_ampliada_equipe_projeto_2ed.pdf. [ Links ]
25. Ministério da Saúde (BR). ABC do SUS: Doutrinas e princípios [Internet]. Brasilia; 1990 [Acesso 22 jul 2015]. Disponível em: http://www.pbh.gov.br/smsa/bibliografia/abc_do_sus_doutrinas_e_principios.pdf. [ Links ]
26. Ministério da Saúde (BR). Portaria n. 3.088 de 23 de dezembro de 2011 (BR). Institui a Rede de Atenção Psicossocial para pessoas com sofrimento ou transtorno mental e com necessidades decorrentes do uso de crack, álcool e outras drogas, no âmbito do Sistema Único de Saúde [Internet]. Diário Oficial da União; 2011 [Acesso 15 fev 2015]. Disponível em: http://www.saude.mg.gov.br/images/documentos/Portaria%20do%20Ministerio%20da%20Saude%20GM%20N%203088%202011%202702.pdf
27. Oliveira GN. O projeto terapêutico singular. In: Campos GWS, Guerrero AVP organizadores. Manual de práticas na atenção básica: saúde ampliada e compartilhada. São Paulo (SP): Aderaldo & Rothschild; 2008. p. 283-97. [ Links ]
28. Dell´Acqua G, Mezzina R. Resposta à crise: estratégia e intencionalidade da intervenção no serviço psiquiátrico territorial. In: Amarante P, coordenador. Archivos de Saúde Mental e Atenção Psicossocial. Rio de Janeiro: Nau; 2005. p. 161-94. [ Links ]
29. Mangia E, Castilho JPLV, Duarte VRE. A construção de projetos terapêuticos: visão de profissionais em dois centros de atenção psicossocial. Rev Terapia Ocup Univ São Paulo. 2006;17(2):87-98. [ Links ]
30. Marco MA. Do modelo biomédico ao modelo biopsicossocial: um projeto de educação permanente. Rev Bras Educ Med. 2006;30(1):60-72. [ Links ]
31. Nascimento GCM, Scorsolini-Comin F, Peres RS. Mental Health in the Unified Health System: Mapping the Contributions from the Psychosocial Care Centers. SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) [Internet]. 2013 [Acesso 15 jan 2016];9(2):95-102. Disponível em: http://pepsic.bvsalud.org/scielo.php?script=sci_abstract&pid=S1806-69762013000200008&lng=pt&nrm=iso&tlng=en [ Links ]
Received: February 5th 2016
Accepted: April 20th 2016
Corresponding Author:
Renata Fabiana Pegoraro
Universidade Federal de Uberlândia
Av. Pará, 1720 - Bloco 2C, Sala 47, Campus Umuarama - Bairro Umuarama
CEP 38405-320. Uberlândia, MG, Brasil
E-mail: rfpegoraro@yahoo.com.br, renata.pegoraro@ufu.br
1 This research was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). Process #CNPQ2014-HUM048 and by Pró-Reitoria de Pesquisa e Pós-Graduação da Universidade Federal de Uberlândia, Uberlândia, MG, Brazil.


{kind=link}
{kind=link}
{kind=link}