










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
On-line version ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.13 no.3 Ribeirão Preto July/Sep. 2017
http://dx.doi.org/10.11606/issn.1806-6976.v13i3p156-166
REVIEW ARTICLE
DOI: 10.11606/issn.1806-6976.v13i3p156-166
Resilience in children and adolescents victims of early life stress and maltreatment in childhood
La resiliencia en niños y adolescentes víctimas de estrés temprano y maltrato en la infancia
Isabela Masucci de Lima CamargoI; Maria Neyrian de Fátima FernandesII; Marina Sayuri YakuwaIII; Ana Maria Pimenta CarvalhoIV; Patricia Leila dos SantosV; Edilaine Cristina Silva Gherardi-DonatoIV; Débora Falleiros de MelloIV
IMaster’s student, Escola de Enfermagem de
Ribeirão Preto, Universidade de São Paulo, PAHO/WHO Collaborating Centre for
Nursing Research Development, Ribeirão Preto, SP, Brazil
IIDoctoral student, Escola de Enfermagem de
Ribeirão Preto, Universidade de São Paulo, PAHO/WHO Collaborating Centre for
Nursing Research Development, Ribeirão Preto, SP, Brazil. Assistant Professor,
Universidade Federal do Maranhão, Imperatriz, MA, Brazil
IIIDoctoral student, Escola de Enfermagem de
Ribeirão Preto, Universidade de São Paulo, PAHO/WHO Collaborating Centre for
Nursing Research Development, Ribeirão Preto, SP, Brazil
IVPhD, Associate Professor, Escola de Enfermagem de
Ribeirão Preto, Universidade de São Paulo, PAHO/WHO Collaborating Centre for
Nursing Research Development, Ribeirão Preto, SP, Brazil
VPhD, Professor, Faculdade de Medicina de Ribeirão
Preto, Universidade de São Paulo, Ribeirão Preto, SP, Brazil
ABSTRACT
This study aimed to characterize resilience in children and adolescents who were abused in childhood. 17 articles were found, between 2011 and 2015. According to the analyzed scientific literature, it found that childhood abuse have negative relationship with the development of resilience and positive with the emergence of depressive and anxiety symptoms, as well as, positive factors such as social and family support has positive relationship with resilience. It is concluded that the development of resilience in children and adolescents victims of abuse can act as a protective factor for these individuals.
Descriptors: Psychological Resilience; Psychological Stress; Child Abuse.
RESUMEN
Este estudio tuvo como objetivo caracterizar la resiliencia en niños y adolescentes abusados en la infancia. Se encontraron 17 artículos, entre 2011 y 2015. De acuerdo con la literatura científica analizada, se encontró que el abuso infantil tiene relación negativa con el desarrollo de la capacidad de recuperación y positiva con la aparición de los síntomas depresivos y de ansiedad, así como, factores positivos tales como el apoyo social y familiar tiene relación positiva con la capacidad de recuperación. Se llegó a la conclusión de que el desarrollo de la resiliencia en niños y adolescentes víctimas de abuso puede actuar como un factor de protección para estas personas.
Descriptores: Resiliencia Psicológica; Estrés Psicológico; Maltrato a Los Niños.
Introduction
From the earliest age to the end of life, the human being experiences the most varied types of stressors and must continually learn to adapt to the different realities shaped by these adversities. We can say that individuals spend their entire lives looking for mechanisms and strategies to overcome and deal with grief, change and constant attempts to turn negative experiences into something positive, whether to avoid contact with stressors or ease their reactions before them.
Thus, it is possible to affirm that life is an ongoing process of losses and gains and a kind of healing is necessary to learn how to deal with losses. This healing process can be compared to the development of resilience in individuals, since it arises from a wound open by trauma(1).
In this sense, we can define resilience as an interactive and subjective process that occurs in some individuals who have a relatively good evolution despite the experience of strong stresses or adversities. These individuals present a better response than others who undergo the same experiences, consolidating some type of development(1-2).
As adversities can be present since the conception of human beings, their impact on child development is a reason of concern, due to the consequent increased chance of triggering physical and mental difficulties throughout life. Any adverse event occurred during childhood is considered an abuse(3), and it is called early stress. Stress is a reaction of individuals to adversity that impels them to seek an adjustment or response to the conditions that aroused the anxiety or fear, aiming to stabilize internal biological processes and preserve self-esteem(4).
According to the World Health Organization (WHO), child abuse corresponds to any type of abuse and neglect that occurs in children under 18 years of age. It includes all types of physical or emotional abuse, sexual abuse, abandonment, neglect or exploitation of any nature that may result in damage, potentiate immediate or long-term harm to health, survival and development of dignity in the context of social interactions(5).
Child abuse leads to suffering of children and their relatives, generating stress that is associated with disrupted brain development. In extreme cases, it may compromise the development of the nervous and immune systems(5).
Studies(3,6-7) show that adults with a history of childhood abuse are at higher risk for development of mental disorders, including depression and anxiety. Indices of use of drugs and other substances and risk behaviors are also more prevalent in these adults.
The greater chance of compromised health in adult life is related to changes in the response to stress triggered by traumatic experiences, that is, the effect of stress as a risk factor for several pathologies can be increased in individuals with a history of childhood abuse because these individuals tend to have an increased response to stress in adult life.
In this context, it is evident that facing sorrow during childhood can indefinitely cause deep marks in individuals. Thus, adverse events, such as childhood abuse, are generators of early stress and factors capable of catalyzing and leading to the development of clinical pathologies and mental disorders in adult life.
Although the relationship between early stress and development of pathologies in the adult life of people who experienced child abuse is clear, not all individuals who have this e kind of traumatic experience develop pathologies. Among the factors underlying this relationship, the literature cites genetic, psychological and social availability.
Thus, the same stressing event occurred early in life could weaken the response to stress in adult life, favoring the development of pathologies, or could act as a catalyst for the development of a greater capacity to respond to future adversities, giving the subjects a higher level of resilience before stressful events.
In view of the exposed problem and the scientific production on the subject, the following guiding question was formulated: What are the characteristics of resilience in children and adolescents victims of childhood abuse? In this sense, the objective of the present study is to characterize resilience in children and adolescents who suffered childhood abuse, based on a review of the scientific literature.
Method
This is an Integrative Literature Review, a method that proposes to incorporate the applicability of study results, establishment of data collection criteria, and a synthesis of knowledge, allowing the inclusion of experimental and non-experimental studies(8-9).
In this study, the integrative review focused first on the identification of the theme and selection of the guiding question of the study; then, establishment of inclusion and exclusion criteria; categorization of studies; evaluation of the studies included in the integrative review; interpretation of results and synthesis of knowledge(10-11).
The topic addressed in this study was the development of resilience in children and adolescents who experience childhood abuse. The guiding question of the research was: how does the development of resilience take place in children and adolescents who have suffered childhood abuse?
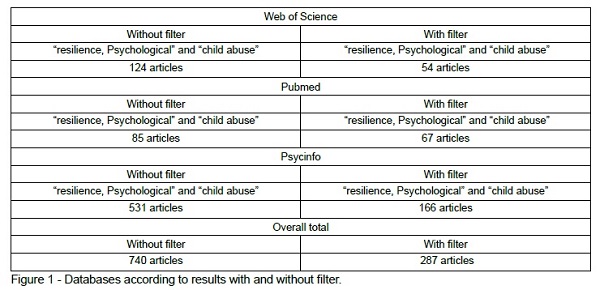
The survey of articles in the literature was carried out in the months of March to April 2016 in the following databases: Web of Science, PubMed/Medline (Medical Literature and Retrivial System on Line), PsycInfo. The DecS (Descriptors in Health Sciences) and MeSH (Medical Subject Headings) descriptors used were: resilience, psychological and child abuse.
The inclusion criteria adopted were: articles published in the period from 2011 to 2015 to include the most up-to-date evidence on the subject, original articles available in full length and published in Portuguese, English or Spanish. Articles that did not address abuse in children and adolescents (abuse suffered up to age 19), research conducted with adults, or with people over 19 years of age, and theoretical or review studies were excluded.
Figure 1 shows the results of the search for articles per database. The initial result refers to the total number of articles found according to the descriptors used, and then the inclusion criteria (filter) were applied to refine the search. Of these studies listed, 287 met the inclusion criteria. After applying the exclusion criteria and after the reading of the articles in full length, the corpus of this study was composed of 17 articles. Then, relevant data for this review were extracted and the information organized in groups.
The overall classification of articles was based on scientific evidence currently available in the literature, including levels of evidence and degrees of recommendation as a way of obtaining the best results. The level of evidence was classified according to the type of study as set by the Oxford Centre for Evidence-based Medicine(12).
At Level 1, evidence comes from randomized controlled clinical trials with narrow-confidence intervals or systematic reviews or meta-analyses of all relevant randomized controlled trials or from clinical guidelines based on systematic reviews of randomized controlled trials. At level 2, evidence comes from historical cohort studies or with segments of committed cases (at least one well-delineated, but lower quality, randomized controlled trials) and ecological studies. At level 3, evidence is obtained from well-designed clinical trials without randomization (case-control studies), systematic reviews of case-control studies. At level 4, evidence comes from case reports (cohort or lower quality case-control studies). At level 5, evidence originates from the opinion of authorities and/or expert committee reports. Studies with evidence up to level three were considered in the present study(12).
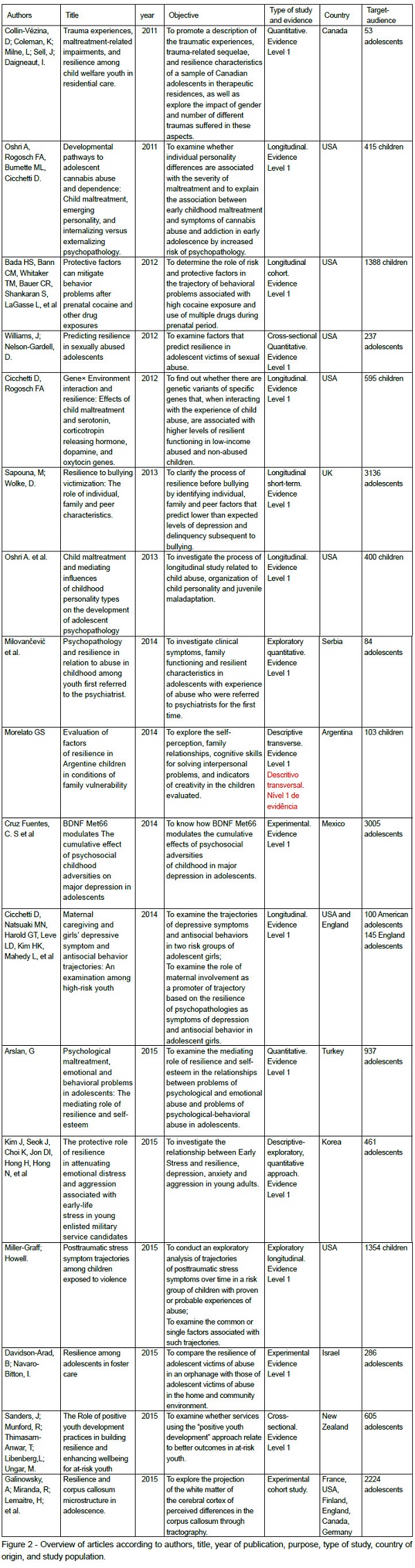
In order to analyze and interpret data, the information was organized in a previously prepared identification form(10) containing the identification of the study, year of publication, authors, type of study, place, and population studied. This information was collected for each article of the sample to catalog the data. This allowed a better visualization and comparison of the articles. Data were organized according to similarities of content that emerged in the corpus investigated and were descriptively analyzed. The articles were distributed into three categories: family and institutional abuse and resilience; sexual abuse and resilience; and resilience and factors intrinsic to the individuals.
Results
The articles that make up the corpus of this study were mostly written in the English language. Figure 2 summarizes the general data of the selected articles. The majority (88%) had a quantitative delineation. As for the place of origin, eight were researches developed in the United States but there was variability among the countries, with results from Canada, United Kingdom, Serbia, Argentina, New Zealand, Israel, Korea, among others. Regarding the level of evidence, all articles we classified as level 1.
The 16 articles were divided into three categories: family and institutional abuse and resilience (10); substance use and abuse and resilience (3); and resilience and factors intrinsic to the individuals (3).
Resilience: family and institutional abuse and early stress
The studies included in this category deal with resilience in children and adolescents victims of family and institutional abuse; ten articles were obtained for this analysis. Five studies(13-17) investigated exclusively the abuse that occurred in the family environment, and the other five(18-22) addressed institutional abuse. Among the ten studies included in this category, two(13, 22) investigated both family and institutional abuse.
It was found that the occurrence of childhood abuse is closely related to higher rates of onset of symptoms of psychiatric disorders(13-15, 19), lower rates of resilience, learning difficulties in children(15), and greater occurrence of delinquency and depressive and anxious behavior in girls who were victims of abuse when compared to girls without such a history(13).
With respect to family abuse, factors that positively influence the development of resilience by children and adolescents, such as parental acceptance and self-perception of adolescents as being resilient(16) and the intervention of secondary family member such as uncles or grandparents to avoid abuse or neglect(15) were described.
A study also found(17) that greater involvement of maternal care and its benefits leads to a decrease in depressive symptoms, but does not prevent their onset. Family factors such as exposure to violence may have a negative effect on the development of resilience(14) and children and adolescents with higher resilience indexes, when compared to those with lower indices, had a greater capacity to identify the existence of family problems(15).
With regard to abuse in institutions, studies reported that children or adolescents who had suffered abuse had experienced effects of such abuse on their development. It was also found(20) that bullying in adolescence is associated with higher levels of depressive symptoms and delinquent behavior. There was also association with lower self-esteem and greater conflict with parents. However, the majority of male adolescents presented lower indexes of these symptoms, thus showing to be more resilient. On the other hand, despite the traumatic experience, female adolescents presented higher self-esteem and a lower rate of family conflicts. The highest level of resilience was also associated with less use of alcohol and other drugs.
As for the relationship between resilience and early stress, median levels of early stress may suggest higher levels of resilience(14), as well as, exposure to violence within the family and community may be a risk factor for the development of post-traumatic stress symptomatology in children and adolescents(14).
In addition, it was identified that adolescents with two or more types of negative experiences achieved lower resilience results; those with four or five different traumatic experiences had the lowest scores when compared with those with only one type(18). The age at which the traumatic experience had been experienced also influenced the development of resilience. It was observed that older and younger adolescents reached similar levels of resilience; however, older subjects had made a better use of the services in which they were inserted(21). Other factors that influence behavioral development are personal variables such as sense of hope or expectation and intelligence, also influencing the development of resilience. Adolescents with lower levels of school engagement, social support, hope and expectation, as well as previous history of sexual abuse, had greater behavioral problems and were less likely to be resilient(22).
Drug use and abuse and resilience
This category included one article(23) that analyzed the effects of a prenatal environment exposed to drugs and its influence on the development and the resilient capacity of the child; and two articles(24-25) that related use and abuse of drugs and childhood abuse.
Abuse of psychoactive substances still during the prenatal phase leaves marks on children that can last for a lifetime. As for the role of risk and protective factors on the development of behavioral problems associated with high exposure to cocaine and use of several different drugs during pregnancy, it was found that children of mothers with high exposure to drugs were more likely to develop an aggressive and problematic behavior during life, especially in the case of boys(23). The other article included in this category showed that individuals with aggressive characteristics had a greater tendency to engage in drug abuse and chemical dependency(24).
Children of mothers who were strongly exposed to drugs had low rates of verbal IQ and attention deficit. However, research showed that children with high levels of resilience were protected against behavioral problems in childhood and adolescence(23).
There was an association between increased risk of psychopathology, individual personality differences and the severity of early childhood abuse with the symptoms of cannabis abuse and dependence in early adolescence. In this study, it was observed that children who had experienced severe levels of abuse were less predisposed to develop resilience and presented more externalizing symptoms (egocentrism and aggressiveness). Child abuse, personality disorder and internalizing or externalizing symptoms predispose to regular use of cannabis and development of cannabis dependence. There is therefore a positive relationship between exposure to trauma and substance use disorder(24).
Similar results were also found in another study(25) in which child abuse was perceived as an environmental stressor that potentiate the impairment of personality development, resulting in increased psychopathology in adolescence and a higher tendency to use cannabis.
Resilience and factors intrinsic to the individual
Four articles were included in this category, two related to the genotype/phenotype interaction, other addressing the neurological characteristics of adolescents exposed to early stress, and a last one that addressed the relationship between self-esteem and resilience.
According to the studies(26-27), there is a close relationship between genotype and stressful events experienced by children and adolescents, who are in a crucial phase of human development. For example, stressful events can cause changes in brain-derived neurotrophic factor (BDNF), a component of the family of homologous proteins known as neurotrophins that plays a central role in the development, physiology, and pathology of the nervous system, as well as in processes related to brain plasticity such as memory and learning(27).
In the research findings(27), it was found that homozygous subjects for BDNF were statistically associated with the resilient phenotype. Moreover, there was evidence that the BDNF genotype associated with the number of adversities experienced in childhood, such as abuses, neglect and family dysfunction, poor family adjustment, parental death and experience of serious diseases, had a protective effect against the risk of lifelong depression. However, these results were evident only in women.
Another research(26) attempted to find out whether there were specific gene variants that interacted with the experience of child abuse and were associated with higher levels of resilient functioning in low-income malnourished children; the study found low resilient functions in abused children. The study also found that individual personality traits such as resilient ego and moderate super-ego, self-esteem process, and relationship factors were differentially predictive of resilient functioning in children who had or not been abused.
The results of this research showed that some genetic variants exert an insignificant effect on the prediction of resilience in the group of abused children. On the other hand, genotype contributes to the high functioning of resilience in non-abused children when compared to abused children who have the same genotype. Abuse experiences may also influence genetic processes, including epigenetic processes and the degree to which genes are expressed(26). That is, childhood abuse can cancel out the effects of a genotype favorable to the development of resilience.
Another path taken to understand the development of resilience is the neurobiological one. The projection of the white matter of the cerebral cortex of perceived differences in the corpus callosum was investigated to evaluate the relationship between negative events of life and fractional anisotropy (FA) values in a sample of adolescents. The results showed that FA is increased after exposure to stressful events and that high levels of FA are associated with high resilience capacity(28).
The results showed an increase in FA in certain segments of the corpus callosum in the resilient group (adolescents with low risk of mental disorder, despite exposure to stressful events). In this way, a solid corpus callosum should protect against mental disorders by increasing resilience. It is, thus, possible to state that the nature of the response of the corpus callosum to early stress can play an important role in the determination of psychiatric resilience(28).
Another factor analyzed was the mediating role of self-esteem and resilience in psychological and emotional abuse, indicating that these are negatively correlated with resilience and self-esteem, and positively correlated with behavioral and emotional problems in adolescents(29). Thus, high levels of resilience and self-esteem protect adolescents from behavioral problems, even when they are experiencing psychological abuse, thus playing an important role in protecting the well-being of adolescents facing adversity(29).
Discussion
Research on the development of resilience among individuals who are victims of child abuse is complex and requires a multidisciplinary approach. Such study runs through the fundamental vision of neurobiology and the psychological paths of development to promote mechanisms of change and points of reflection for intervention in the human life cycle(30). Therefore, promoting resilience is a critical factor for children experiencing early abuse and neglect.
The results of this review are consistent with another study(31) that considers the variations in resilience to be associated with various influences such as the age at which the stressful situation is experienced, temper and personality of the child, availability of social capital in the home and in the community, and family poverty.
Moreover, the development of resilience has been also seen in children and adolescents who use drugs. The study showed that frequent use of drugs is detrimental, especially in dysfunctional families. Furthermore, drug abuse can generate other forms of harm such as sexually transmitted diseases and cardiorespiratory problems and injuries resulting from violence(32).
Studies(31, 33) of human development show the influence of the quality of parenting on individuals. Effective parenting has been associated with positive outcomes in children exposed to a range of adverse conditions, such as poverty, divorce, and parental death. Thus, parenting can be considered an important resource for promoting resilience.
The presence of depression in the caregiver is also an important factor in child development. Depressive symptoms were associated with children who were unlikely to develop competence criteria in the social, behavioral and resilient domains(30). Besides the quality of parenting, having healthy parents is also another important factor that promotes resilience in young children.
The study of resilience must constantly consider how impressive is the complexity in which the body and the brain interact through different environments(26). Currently, the field of genetics is rapidly turning attention towards studies on global genomic expression profile in large populations to examine the complex genetic contributions to resilience. Additional genetic polymorphisms, and gene-gene and gene-environment interactions have currently been identified. As the genetic basis of resilience becomes more evident, it is expected that genes and therapeutic drugs be specifically developed for low resilience genetic profiles(34).
Although social support and the influence of social relationships are essential to help children overcome difficulties experienced in early age, the evidence suggests that intrinsic characteristics and external factors do not exert an isolated but rather a joint influence to promote and help maintaining resilience(35).
Conclusion
The analyzed aspects show that children and adolescents who experience adversity can develop resilience according to several factors ranging from genetic characteristics to the quality of the relationship with social institutions. Knowing these factors makes it possible to know and understand how individuals are able to adapt to new forms, seek resources in themselves and in the environment that surround them, solve the problems that they meet in the course of their lives, through the development of resilience.
Scientific evidence from the analyzed studies made it clear that the identification of stressors in childhood and adolescence is essential for prevention and health promotion actions in order to increase the possibilities for the development of resilience in these individuals. As for the practice of health professionals, it is fundamental to include this theme in the training, in the continuing education and in the planning of health care, seeking the instrumentation of the professional action to detect and intervene in cases of children and adolescents in situation of abuse.
However, further studies are still needed to understand how to intervene so as to facilitate the promotion of resilience since childhood, through the social and family support network that children or adolescents may have, so that they may grow and develop in a healthy and safe manner, having their rights guaranteed.
It is noteworthy that although there is a large scientific production on issues related to resilience, the research of this topic specifically related to children and adolescents victims of abuse, the literature produced is still insufficient. Bearing in mind that, for the described age group, the development of resilience is a key protective factor in favor of healthy development, the need for investment in intervention studies to contribute to the construction of scientific evidence focused on the development of resilience for improvement of assistance to children and adolescents who experience situations of early stress is clear.
References
1. Coimbra RM, Morais NA. A resiliência em questão: perspectivas teóricas, pesquisa e intervenção. Porto Alegre: Artmed; 2015. 232p. [ Links ]
2. Rutter M. Annual Research Review: Resilience – clinical implications. Journal of Child Psychology and Psychiatry. 2013;54(4):474-87. doi: 10.1111/j.1469-7610.2012.02615.x. [ Links ]
3. Herrenkohl TI, Jung H, Klika JB, Mason WA, Brown EC, Leeb RT, et al. Mediating and Moderating Effects of Social Support in the Study of Child Abuse and Adult Physical and Mental Health. Am J Orthopsychiatry. 2016. [ Links ]
4. Townsend MC. Psychiatric Mental Health Nursing: concepts of care in evidence-based practice. 8th ed. Philadelphia: F. A. Davis Company; 2014. [ Links ]
5. World Health Organization (WHO). Child maltreatment. In: Organization WHO, editor. Geneva: World Health Organization; 2014. [ Links ]
6. Hebert M, Lavoie F, Blais M. Post Traumatic Stress Disorder/PTSD in adolescent victims of sexual abuse: resilience and social support as protection factors. Cien Saude Colet. 2014;19(3):685-94. [ Links ]
7. Konradt CE, Jansen K, Magalhães PVdS, Pinheiro RT, Kapczinski FP, Silva RAd, et al. Early trauma and mood disorders in youngsters. Archives of Clinical Psychiatry (São Paulo). 2013;40:93-6. [ Links ]
8. Lanzoni GMM, Meirelles BHS. Liderança do enfermeiro: uma revisão integrativa da literatura. Revista Latino-Americana de Enfermagem. 2011;19(3):651-8. [ Links ]
9. Souza MT, Silva MD, Carvalho R. Revisão integrativa: o que é e como fazer? Einstein. 2010; 8(1): 102-6. [ Links ]
10. Broome ME. Integrative literature reviews for the development of concepts. In: Rodgers BL, Knafl KA, editors. Concept development in nursing: foundations, techniques and applications. Philadelphia (USA): W.B Saunders Company; 2000. p.231-50. [ Links ]
11. Ganong LH. Integrative reviews of nursing research. Res Nurs Health. 1987 Mar; 10(1):1-12. Oxford. Oxford Centre for Evidence-based Medicine – Levels of Evidence: Oxford University; 2009 [cited 2016 15 mai]. Disponível em: http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/. [ Links ]
13. Milovancević MP, Tenjović L, Ispanović V, Mitković M, Kirćanski JR, Mincić T, et al. Psychopathology and resilience in relation to abuse in childhood among youth first referred to the psychiatrist. Vojnosanit Pregl. 2014;71(6):565-70.
14. Miller-Graff LE, Howell KH. Posttraumatic stress symptom trajectories among children exposed to violence. J Trauma Stress. 2015;28(1):17-24. [ Links ]
15. Morelato GS. Evaluación de factores de resiliencia en niños argentinos en condiciones de vulnerabilidad familiar. Universitas psychologica. 2014;13(4):1473-88. [ Links ]
16. Davidson-Arad B, Navaro-Bitton I. Resilience among adolescents in foster care. Children And Youth Services Review. 2015;59:63-70. doi: 10.1016/j.childyouth.2015.09.023. [ Links ]
17. Cicchetti D, Natsuaki MN, Harold GT, Leve LD, Kim HK, Mahedy L, et al. Maternal caregiving and girls’ depressive symptom and antisocial behavior trajectories: An examination among high- risk youth. 2014;26(4pt2):1461-75.
18. Collin-Vezina D, Coleman K, Milne L, Sell J, Daigneault I. Trauma Experiences, Maltreatment-Related Impairments, and Resilience among Child Welfare Youth in Residential Care. International Journal of Mental Health and Addiction. 2011(5):577-89. [ Links ]
19. Kim J, Seok J, Choi K, Jon DI, Hong H, Hong N, et al. The Protective Role of Resilience in Attenuating Emotional Distress and Aggression Associated with Early- life Stress in Young Enlisted Military Service Candidates. Journal Of Korean Medical Science. 2015;30(11):1667-74. [ Links ]
20. Sapouna M, Wolke D. Resilience to bullying victimization: The role of individual, family and peer characteristics. Child Abuse & Neglect. 2013;37(11):997-1006. [ Links ]
21. Sanders J, Munford R, Thimasarn-Anwar T, Liebenberg L, Ungar M. The role of positive youth development practices in building resilience and enhancing wellbeing for at- risk youth. Child Abuse & Neglect. 2015;42:40-53. [ Links ]
22. Williams J, Nelson-Gardell D. Predicting Resilience in Sexually Abused Adolescents. Child Abuse & Neglect: The International Journal. 2012;36(1):53-63. [ Links ]
23. Bada HS, Bann CM, Whitaker TM, Bauer CR, Shankaran S, LaGasse L, et al. Protective factors can mitigate behavior problems after prenatal cocaine and other drug exposures.(Report). Pediatrics. 2012;130(6):E1479. [ Links ]
24. Oshri A, Rogosch FA, Cicchetti D. Child maltreatment and mediating influences of childhood personality types on the development of adolescent psychopathology. J Clin Child Adolesc Psychol. 2013;42(3):287-301. [ Links ]
25. Oshri A, Rogosch FA, Burnette ML, Cicchetti D. Developmental Pathways to Adolescent Cannabis Abuse and Dependence: Child Maltreatment, Emerging Personality, and Internalizing Versus Externalizing Psychopathology. Psychology of Addictive Behaviors. 2011;25(4):634-44. [ Links ]
26. Cicchetti D, Rogosch FA. Gene × Environment interaction and resilience: Effects of child maltreatment and serotonin, corticotropin releasing hormone, dopamine, and oxytocin genes. Development and Psychopathology. 2012;24(2):411-27. [ Links ]
27. Cruz-fuentes CS, Benjet C, Martínez-levy GA, Pérez-molina A, Briones-velasco M, Suárez-gonzález J. BDNF Met66 modulates the cumulative effect of psychosocial childhood adversities on major depression in adolescents. Brain and Behavior. 2014;4(2):290-7. [ Links ]
28. Galinowski A, Miranda R, Lemaitre H, Paillère Martinot ML, Artiges E, Vulser H, et al. Resilience and corpus callosum microstructure in adolescence. 2015;45(11):2285-94. [ Links ]
29. Arslan G. Psychological maltreatment, emotional and behavioral problems in adolescents: The mediating role of resilience and self-esteem. Child Abuse Negl. 2015;52:200-9. [ Links ]
30. Panter-Brick C, Leckman JF. Editorial commentary: resilience in child development–interconnected pathways to wellbeing. Journal of Child Psychology and Psychiatry. 2013 Apr 1;54(4):333-6. [ Links ]
31. Dubowitz H, Thompson R, Proctor L, Metzger R, Black MM, English D, et al. Adversity, Maltreatment, and Resilience in Young Children. Academic pediatrics. 2016 Apr 30;16(3):233-9. [ Links ]
32. Claro HG, Oliveira MAF, Ribeiro APR, Fernandes CC, Cruz AS, Santos EGM. Perfil e padrão de uso de crack de crianças e adolescentes em situação de rua: uma revisão integrativa. SMAD, Ver. Eletrônica Saúde Mental Álcool Drog. 2014 Apr; 10(1): 35-41. [ Links ]
33. Sandler I, Schoenfelder E, Wolchik S, MacKinnon D. Long-term impact of prevention programs to promote effective parenting: Lasting effects but uncertain processes. Annual review of psychology. 2011;62:299. [ Links ]
34. Wu G, Feder A, Cohen H, Kim JJ, Calderon S, Charney DS, et al. Understanding resilience. Frontiers in behavioral neuroscience. 2013 Feb 15;7:10. [ Links ]
35. Herrenkohl TI, Jung H, Klika JB, Mason WA, Brown EC, Leeb RT, et al. Mediating and Moderating Effects of Social Support in the Study of Child Abuse and Adult Physical and Mental Health. Am J Orthopsychiatry. 2016. [ Links ]
Received: Oct. 12th 2016 Corresponding Author:
Accepted: Jul. 30th 2017
Maria Neyrian de Fátima Fernandes
Universidade de São Paulo. Escola de
Enfermagem de Ribeirão Preto
Av. dos Bandeirantes, 3900
Bairro: Monte Alegre
CEP: 14040-902
Ribeirão Preto, SP, Brasil
E-mail: neyrianfernandes@gmail.com

