










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.14 no.3 Ribeirão Preto jul./set. 2018
https://doi.org/10.11606/issn.1806-6976.smad.2018.000367
ARTIGO DE REVISÃO
DOI: 10.11606/issn.1806-6976.smad.2018.000367
O auto-estigma dos usuários de álcool e drogas ilícitas e os serviços de saúde: uma revisão integrativa da literatura
El auto-estigma de los usuarios de alcohol y drogas ilícitas y los servicios de salud: um repaso integrativa de la literatura
Raquel Helena Hernandez FernandesI; Carla Aparecida Arena VenturaI
IUniversidade de São Paulo, Escola de Enfermagem de Ribeirão Preto, Centro Colaborador da OPAS/OMS para o Desenvolvimento da Pesquisa em Enfermagem, Ribeirão Preto, SP, Brasil
RESUMO
OBJETIVOS: identificar, analisar e sintetizar evidências científicas sobre a relação entre o estigma existente nos serviços de saúde no que se refere aos usuários de álcool e drogas ilícitas e o auto-estigma destes usuários.
MÉTODO: revisão integrativa da literatura, através de cinco etapas distintas.
RESULTADOS: do total de artigos encontrados nas bases de dados, 07 foram selecionados e analisados, resultando nas categorias "O estigma público nos serviços de saúde" e "A relação entre o estigma nos serviços de saúde e o auto-estigma em usuários de álcool e drogas ilícitas".
CONCLUSÃO: o auto-estigma é influenciado pelo estigma público propagado, principalmente, por autoridades e por profissionais de saúde. Uma das alternativas para atenuar o cenário do auto-estigma é o apoio social.
Descritores: Usuários de Drogas; Transtornos Relacionados ao Álcool; Auto-Estigma; Estigma Internalizado; Serviços de Saúde.
RESUMEN
OBJETIVOS: identificar, analizar y sintetizar evidencias científicas sobre la relación entre el estigma existente en los servicios de salud en el que se refiere a los usuarios de alcohol y drogas ilícitas y el auto-estigma de estos usuarios.
MÉTODO: revisión integrativa de la literatura, por medio de cinco etapas distinguidas.
RESULTADOS: del total de artículos encontrados en las bases de datos, 07 fueron seleccionados y analizados, resultando en las categorias "El estigma público en los servicios de salud" y "La relación entre el estigma en los servicios de salud y el auto-estigma em usuarios de alcohol y drogas ilícitas".
CONCLUSIÓN: el auto-estigma es influenciado por el estigma público propagado, principalmente, por autoridades y por profesionales de salud. Una de las alternativas para atenuar el escenario del auto-estigma es el apoyo social.
Descriptores: Consumidores de Drogas; Trastornos Relacionados con el Alcohol; Autoestigma; Estigma Internalizado; Servicios de Salud.
Introdução
Quando o uso de álcool e drogas ilícitas passa a ser um problema para a sociedade e promove em seus usuários comportamentos socialmente inaceitáveis, com uma conotação negativa, estes são associados a uma imagem de fraqueza moral, o que pode acarretar em sua exclusão social(1), tornando-os um grupo vulnerável da população(2).
Dentre as formas de exclusão dos usuários de álcool e drogas ilícitas destaca-se o estigma, que está muito relacionado ao preconceito, à marginalização e à eugenia. O termo estigma foi criado pelos gregos para designar sinais no corpo feitos com cortes ou fogo, para denunciar que a pessoa que os tivesse era escrava, criminosa ou traidora e, também, para anunciar que essa pessoa possuía algo de mau. O estigma representa uma construção social que atua como uma marca que atribui a um indivíduo um status desvalorizado em relação ao outro(3).
O estigma dos usuários de álcool e drogas ilícitas está associado a como a sociedade encara esse problema. Logo, em uma sociedade em que o alcoolismo ou o uso de drogas ilícitas possui uma forte conotação moralizante, o estigma social se torna um grande problema para o usuário(1).
Existem duas vertentes de estudo sobre estigma relacionado ao uso de álcool e outras drogas. A primeira está ligada ao entendimento e ao estudo de como se forma o processo de estigmatizar e as estratégias de mudança de percepção dos profissionais e dos próprios usuários sobre o uso de álcool, a fim de promover uma postura resiliente na recuperação do problema. A outra linha de estudo estabelece que o reforço do estigma social é visto como benefício para o controle e recuperação do usuário de álcool e drogas ilícitas. Nessa perspectiva, existe uma punição social não formalizada que procura passar a mensagem de que determinados comportamentos não são tolerados socialmente(4).
Nesse contexto, o estigma representa importante fonte de danos, especialmente em situações de busca por emprego e moradia, o que resulta em isolamento social e, muitas vezes, em lacunas na utilização dos serviços de saúde(2).
Além disso, alguns teóricos argumentam que o uso/abuso do álcool e outras drogas ilícitas teve, e ainda tem, repercussões nos cenários da desassistência ao usuário, estigma e preconceito, formas de tratamento inadequadas, exclusão familiar, moralidade social, associação ao ócio e à criminalidade(5).
Desse modo, a atribuição moral e culpabilização do usuário de álcool e drogas ilícitas pela sociedade podem criar barreiras na qualidade do cuidado em saúde, reforçando sua exclusão e sofrimento(2) e possibilitando o surgimento de dois tipos principais de estigma que se inter-relacionam: o estigma público, que ocorre quando um grupo adquire preconceito em relação a outro grupo, e o auto-estigma, no qual membros de um grupo estigmatizado internalizam o estigma público(6). Assim, os usuários de álcool e drogas ilícitas se sentem e são estigmatizados tanto pela sociedade quanto se auto-estigmatizam, o que origina isolamento social e pode atuar como barreira para os tratamentos médicos e psicológicos(7-8), uma vez que os referidos usuários internalizam todos os preconceitos e exclusões provenientes do estigma público, sendo levados à crença que de fato são moralmente condenáveis e, por isso, não merecedores de quaisquer benefícios, restando-lhes o isolamento social.
É, portanto, fundamental compreender o fenômeno do auto-estigma por parte dos usuários de álcool e drogas ilícitas e, assim, buscar maneiras de enfrentamento, bem como de minimizar suas consequências. Este estudo apresenta como objetivos identificar, analisar e sintetizar evidências científicas sobre a relação entre o estigma existente nos serviços de saúde no que se refere aos usuários de álcool e drogas ilícitas e o auto-estigma destes indivíduos.
Método
Para alcançar o objetivo deste estudo, uma revisão integrativa da literatura foi realizada para reunir e sintetizar o conhecimento pré-existente sobre a relação entre o estigma por parte dos serviços de saúde no que diz respeito aos usuários de álcool e drogas ilícitas e o auto-estigma destes indivíduos, por meio de pesquisas múltiplas que visam embasar discussões e conclusões gerais a respeito deste tema(9).
O percurso metodológico ocorreu em cinco etapas distintas: 1) formulação do problema, 2) coleta de dados ou definições sobre a busca na literatura, 3) avaliação dos dados, 4) análise dos dados e 5) apresentação e interpretação dos resultados(10-11).
Dessa forma, a pergunta norteadora do processo revisional foi: Qual é a relação entre o estigma proveniente dos serviços de saúde no que se refere aos usuários de álcool e drogas ilícitas e o seu auto‑estigma? A pergunta foi construída por meio da estratégia PICo (P: paciente ou problema; I: intervenção; Co: contexto)(12), que consistiu em: P (usuários de álcool e drogas ilícitas), I (auto-estigma), Co (estigma proveniente dos serviços de saúde).
A seleção dos artigos ocorreu a partir das bases de dados eletrônicas, dentre elas, a CINAHL, que é uma base importante na área da Enfermagem; APA Psycnet (American Psychological Association), que é uma base reconhecida na área da Psicologia; Scopus, que é uma base de dados multidisciplinar; e Pubmed, por ser a base de maior relevância na saúde internacional.
Para a obtenção dos trabalhos relacionados à temática proposta, a qualificação do processo ocorreu pela busca de palavras-chaves, uma vez que a busca por meio de descritores resultou em muitos artigos não pertinentes ao assunto. As palavras-chave utilizadas foram "drug users", "substance use disorders", "alcohol-related disorders", "alcoholism", "self stigma", "internalized stigma", "substance-related disorders", "health services", "delivery of health care", "health care", "addiction", "alcohol drinking patterns", "drug abuse", "drug usage", "marijuana usage", "intravenous drug usage", e "substance abusers".
Os critérios de inclusão dos estudos foram: artigos publicados nos idiomas inglês, espanhol e português, estudos primários recuperados nas bases de dados no período de 1992 a 2015. Os critérios de exclusão adotados foram a impossibilidade de aquisição do artigo, os classificados como editoriais e os que não corresponderam diretamente à temática. Os artigos científicos foram submetidos a uma pré-seleção por meio de leituras do título e resumo, de forma a compor um conjunto de trabalhos associados à questão norteadora.
Resultados
Revisão Integrativa
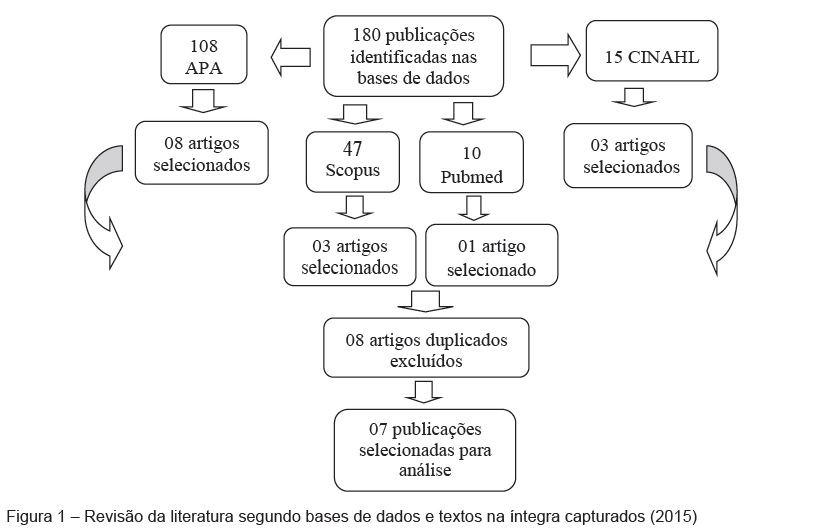
Foram encontrados, ao todo, 180 artigos. A partir da leitura de títulos e resumos, na base de dados CINAHL, dos 15 artigos encontrados, 03 foram selecionados. Na APA Psycnet, foram encontrados 108 artigos, dos quais 08 foram selecionados. Na base de dados Scopus, 47 artigos foram encontrados e 03 artigos foram selecionados. Ainda, por meio da base de dados Pubmed, 10 artigos foram encontrados, sendo 01 artigo selecionado. A partir desta pré-seleção, com a filtragem dos artigos por meio de leituras e buscas de repetição de artigos nas bases de dados, 08 artigos foram excluídos, restando 07 que foram selecionados para leitura na íntegra. A Figura 1 sintetiza as fases de busca e seleção de artigos desta revisão.
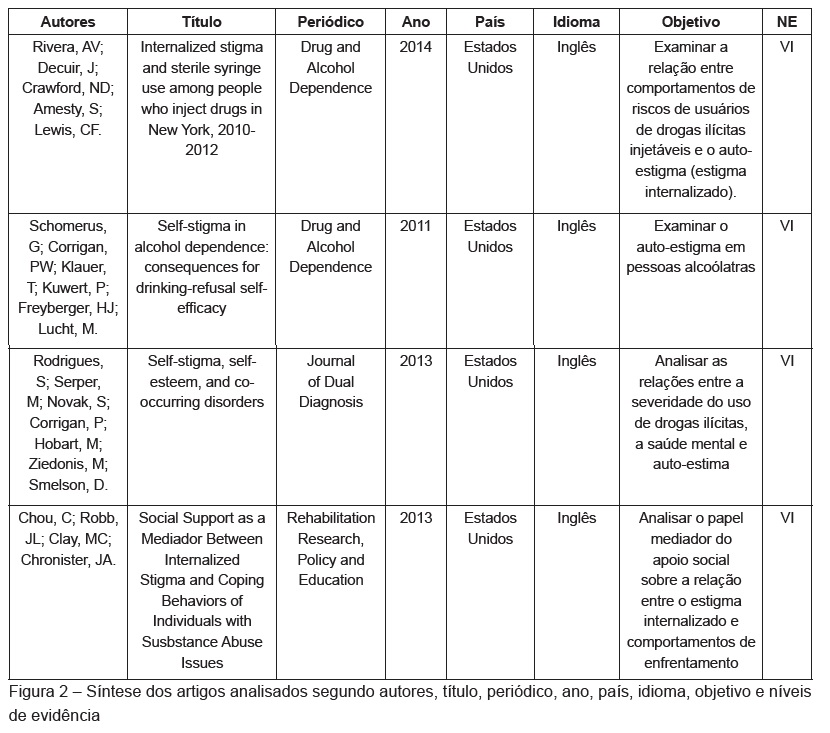
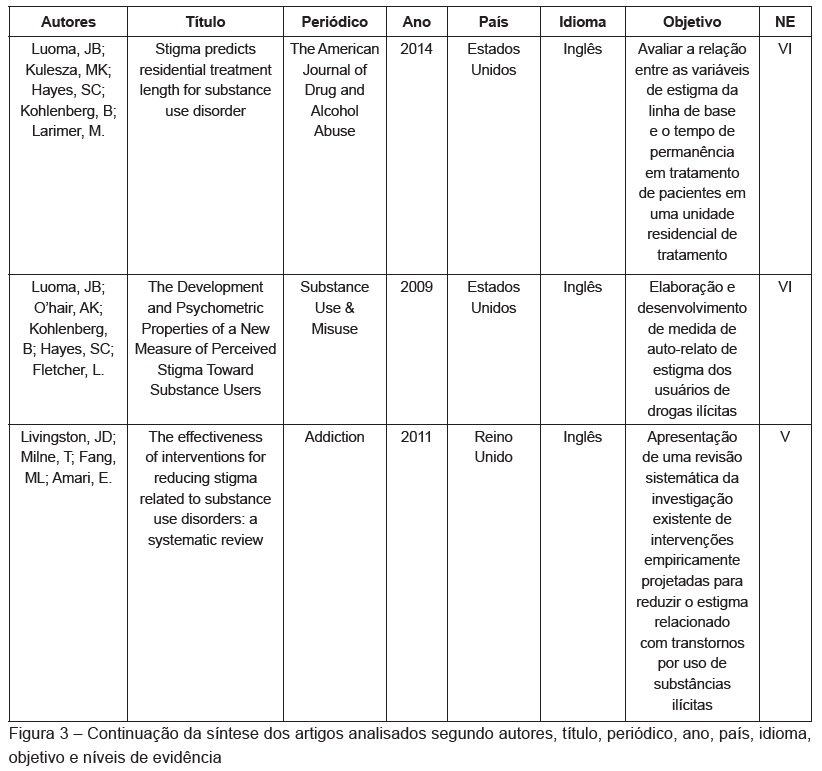
Os artigos analisados passaram por um levantamento de informações que consistiram em autores, título, periódico, ano, país, idioma, objetivo e nível de evidência (NE)(9), sintetizados nas Figuras 2 e 3.
Observa-se a prevalência de estudos descritivos (nível de evidência VI), recentemente publicados e em idioma inglês. Durante a avaliação dos estudos, alguns aspectos foram categorizados para facilitar a identificação daqueles que se repetiam.
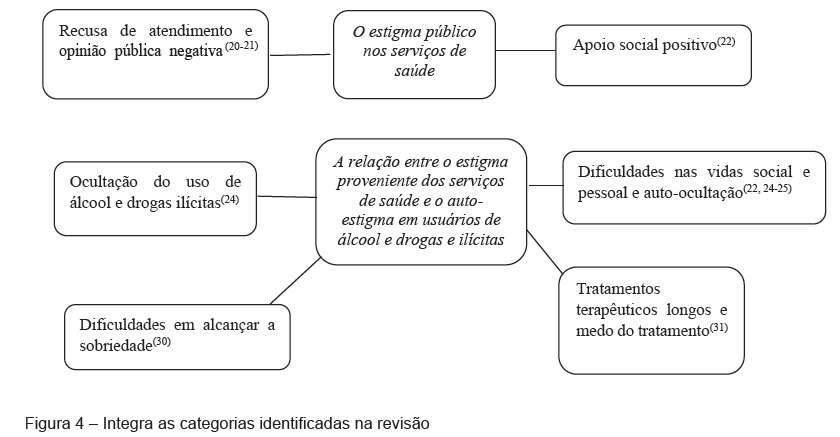
Como resultado final, a leitura dos artigos selecionados possibilitou visualizar o processo de auto-estigma em usuários de álcool e drogas ilícitas, dividido em dois aspectos: o estigma público nos serviços de saúde (profissionais de saúde) e a relação entre esse estigma e o auto-estigma em usuários de álcool e drogas ilícitas.
Discussão
O estigma público nos serviços de saúde
Os serviços de saúde são organizações integradas por profissionais de saúde, que influenciam suas ações internas e externas. Os estudos selecionados sugerem que esses profissionais podem cultivar crenças negativas sobre as pessoas usuárias de álcool e drogas ilícitas por meio de ideias de que esses usuários utilizam recursos do sistema que não pertencem especificamente ao tratamento, além de muitas vezes não aderirem ao tratamento recomendado(13-14). Tais percepções podem contribuir para a prestação desigual e pobre de cuidados para essas pessoas.
Nesse contexto, os usuários podem optar por esconder seus problemas de uso de substâncias para evitar o estigma, o que pode resultar na prestação de cuidados que não atendam às necessidades relacionadas com o uso de substâncias (por exemplo, durante a gravidez)(15). Além disso, os profissionais de saúde podem se recusar a oferecer certos serviços (por exemplo, troca de agulhas) ou não prescrever tratamentos farmacológicos eficazes para pacientes que sofrem de outras doenças (por exemplo, câncer, dor nas costas) por causa do estigma(16-17).
O sucesso no tratamento terapêutico desses pacientes é raro, uma vez que a recaída é rotineira e é muito influenciada pelo estigma proveniente dos profissionais de saúde(18). Conjugado a isso, os pacientes que retomam tratamento já iniciado sofrem mais estigma e preconceito do que aqueles que estão aderindo ao tratamento pela primeira vez(19).
Estes achados reforçam a teoria de que o estigma público estrutural é proveniente de atitudes e comportamentos negativos de representantes de instituições públicas, tais como as pessoas que trabalham nos setores da saúde e da justiça criminal, por exemplo(20). Assim, é possível concluir que a opinião pública sobre a gravidade do uso do álcool e drogas ilícitas, no sentido moralmente pejorativo, relaciona-se também ao auto-estigma, facilitando que os usuários internalizem a opinião pública negativa(21).
Diante de tal cenário, estudos apontam que o apoio social positivo consegue diminuir o impacto negativo do auto-estigma, pelo fato de que os usuários de álcool e drogas ilícitas internalizam o mínimo possível as atitudes estigmatizantes, o que os leva a promoverem comportamentos de enfrentamento e de gestão do estigma(22).
A relação entre o estigma proveniente dos serviços de saúde e o auto-estigma em usuários de álcool e drogas ilícitas
O ato de usuários de álcool e drogas esconderem o uso(18,23) é uma das consequências do auto-estigma, o que os impossibilita a procurar ajuda médica, serviços sociais e apoio social(24). Assim, essas pessoas usam a auto-ocultação como forma de enfrentamento, ou seja, preferem passar despercebidas pela sociedade(25).
Além disso, os usuários de álcool e drogas ilícitas que internalizam o estigma são depressivos(26), evitam o tratamento, sentem-se incapazes de procurar emprego e possuem pobres relações interpessoais(27). Nessa perspectiva, especificamente os usuários de drogas ilícitas possuem um grande número de parceiros sexuais e de parceiros para consumo de drogas, possivelmente por se entenderem e dividirem as experiências discriminatórias que vivenciaram e vivenciam(28-29).
Nessa mesma esfera, usuários de drogas ilícitas injetáveis que sofrem auto-estigma, sentem-se mais confortáveis adquirindo seringas em farmácias, e não em serviços públicos(24). Ademais, o estigma e o auto-estigma podem dificultar os usuários de álcool e drogas ilícitas a alcançar a sobriedade(30).
Ainda sobre o tratamento terapêutico, outro ponto significativo sobre o auto-estigma é que quanto mais elevado ele se torna e quanto maior a vergonha, mais longo é o tratamento. Isso ocorre pelo fato de que os usuários de álcool e drogas ilícitas têm medo do que será abordado durante o tratamento e de serem julgados por seus comportamentos e dependências(31).
Percebe-se uma relação muito próxima entre as categorias identificadas. Assim, com o objetivo de ilustrar a discussão e sintetizar as referidas categorias, foi elaborada a Figura 4.
Considerações finais
Esta revisão integrativa identificou poucos estudos que analisaram a relação entre o estigma por parte dos profissionais de saúde e o auto-estigma em usuários de álcool e drogas ilícitas. A literatura nesta área ainda é escassa, o que leva a crer que há a necessidade de mais pesquisas e estudos direcionados ao auto-estigma em usuários de álcool e drogas ilícitas.
Nesse sentido, as publicações existentes são significativas ao apontar que o auto-estigma é muito influenciado pelo estigma público propagado, principalmente, por entidades tidas como autoridades e por profissionais de saúde, o que engloba os serviços de saúde. Esses indivíduos e entidades são referências sociais, o que torna o estigma público ainda mais grave nesses casos.
Diante dessa opinião pública negativa, há a a crença de que as pessoas usuárias de álcool e drogas ilícitas não são dignas de assistência de saúde e, assim, surge a recusa de atendimento e tratamento teraupêutico a esses indíviduos. Mesmo quando não há recusa, o estigma público é fator tão demolidor que quando os usuários de álcool e drogas ilícitas sentem-se estigmatizados, internalizam o estigma, resultando no auto-estigma.
Uma das consequências do auto-estigma é o medo das pessoas usuárias de álcool e drogas ilícitas sobre o que será abordado durante o tratamento terapêutico, que se torna ineficaz, com alto índice de recaídas e dificultando o usuário a alcançar a sobridade. Ainda nesse cenário, o auto-estigma apresenta como consequências a ocultação do uso das substâncias, e a dificuldade de alcançarem vidas sociais e pessoais saudáveis e dignas.
Existem alternativas para a melhora do cenário do auto-estigma e uma delas é o apoio social positivo. Se o usuário de álcool e drogas ilícitas sente que tem o apoio social positivo de familiares, amigos, profissionais de saúde e autoridades, poderá sentir-se amparado, acolhido e, assim, o seu tratamento terapêutico poderá ser eficaz. Dessa forma, intervenções nos grupos acima relatados podem desmistificar a dependência do álcool e das drogas ilícitas, fazendo com que o apoio social prevaleça sobre o estigma.
Referências
1. Ronzani TM, Furtado EF. Estigma Social sobre o Uso de Álcool. J Bras Psiquiatr. 2010; 9(4):326-32. [ Links ]
2. Pickenhagen A, Sartorius N. Annotated bibliography of selected publications and other materials related to stigma and discrimination because of mental illness and intervention programmes fighting it. Geneva: World Psychiatric Association; 2002. [ Links ]
3. Goffman E. Estigma – Notas da manipulação da identidade deteriorada. 4 ª ed. Rio de Janeiro: LTC Editora; 1998.
4. Room R. Stigma, social inequality and alcohol and drug use. Drug Alcohol Rev. 2005; 24:143-55. [ Links ]
5. Azevedo DM, Miranda FAN. Práticas Profissionais e Tratamento Ofertado nos CAPSad do Município de Natal-RN: com a palavra a família. Esc Anna Nery. 2010;14 (1):56-63. [ Links ]
6. Corrigan PW. How stigma interferes with mental health care. Am Psychol. 2004; 59:614-25. [ Links ]
7. Berger M, Wagner TH, Baker LC. Internet use and stigmatized illness. Soc Sci Med. 2005;61:1821-7. [ Links ]
8. Palm J. Moral concerns – Treatment staff and user perspectives on alcohol and drug problems [master’s thesis]. Department of Criminology, University of Stockholm, Stockholm; 2006.
9. Mendes KDS, Silveira RCCP, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem.Texto Contexto Enferm. 2008; 17:758-64. [ Links ]
10. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005;52(5):546-53. [ Links ]
11. Ganong LH. Integrative reviews of nursing research. Res Nurs Health. 1987;10(1):1-11. [ Links ]
12. Santos CMC, Pimenta CAM, Nobre MR. The PICO strategy for the research question construction and evidence search. Rev. Latino-am. Enfermagem. 2007; 15:508-11. [ Links ]
13. Weiss M G, Ramakrishna J, Somma D. Health-related stigma: rethinking concepts and interventions. Psychol Health Med. 2006; 11: 277–87.
14. Henderson S, Stacey CL, Dohan D. Social stigma and the dilemmas of providing care to substance users in a safetynet emergency department. J Health Care Poor Underserved. 2008; 19:1336–49.
15. Ahern J, Stuber J, Galea S. Stigma, discrimination and the health of illicit drug users. Drug Alcohol Depend. 2007; 88:188–96.
16. Anstice S,Strike CJ, Brands B. Supervised methadone consumption: client issues and stigma. Subst Use Misuse. 2009;44:794–808.
17. Shah S, Diwan S. Methadone: does stigma play a role as a barrier to treatment of chronic pain? Pain Physician. 2010;13: 289–93.
18. Luoma JB, Twohing MP, Waltz T, Hayes SC, Roget N, Padilla M, et al. An investigation of stigma in individuals receiving treatment for substance abuse. Addict Behav. 2007;32: 1331-46. [ Links ]
19. Semple SJ, Grant I, Patterson TL. Utilization of Drug Treatment Programs by Methamphetamine Users: The Role of Social Stigma. Am J Addictions. 2005; 14:367–80.
20. Livingston JD, Milne T, Fang ML, Amari E. The effectiveness of interventions for reducing stigma related to substance use disorders:a systematic review. Addiction. 2011;107: 39-50. [ Links ]
21. Rodrigues S, Serper M, Novak S, Corrigan P, Hobart M, Ziedonis M, et al. Self-stigma, self-esteem, and co-occurring disorders. J Dual Diagn. 2013; 9(2):129-33. [ Links ]
22. Chou C, Rohb JL, Clay MC, Chronister JA. Social Support as a Mediator Between Internalized Stigma and Coping Behaviors of IndividuiJs With Substance Abuse Issues. Rehabil Res, Policy, Educ. 2013;27:104-8. [ Links ]
23. Mateu-Gelabert P, Maslow C, Flom PI, Sandoval M, Bolyard M, Friedman SR. Keeping it together: stigma, response and perception of risk in relationships between drug injectors and crack smorkers, and other community residents. AIDS Care. 2005;17:802-13. [ Links ]
24. Rivera AV, DeCuir J, Crawford ND, Amesty S, Lewis CF. Internalized stigma and sterile syringe use among people who inject drugs in New York City, 2010-2012. Drug Alcohol Dependence. 2014; 144: 259-64.
25. Luoma JB, O’Hair AK, Kohlenberg BS, Hayes SC, Fletcher L. The Development and Psychometric Properties of a New Measure of Perceived Stigma Toward Substance Users. Substance Use Misuse. 2009; 45:47–57.
26. Latkin C, Davey-Rothwell M, Yang JY, Crawford N. The relationship between drug user stigma and depression among inner-city drug users in Baltimore. MD. J Urban Heatlh. 2012; 90:147-56. [ Links ]
27. Luoma JB, Kohlenberg BS, Hayes SC, Bunting K, Rye AK. Reducing selfstigma in substance abuse through acceptance and commitment therapy: Model, manual development, and pilot outcomes. Addiction Res Theory. 2008;16(2):149-65. [ Links ]
28. Crawford ND, Ford CG, Galea S, Latka M, Vlahov D. The relationship between perceived discrimination and high-risk social ties among illicit drug users in New York City – 2006-2009. AIDS Behav. 2012; 17: 419-26.
29. Crawford ND, Borrell LN, Galea S, Ford C, Latkin C, Fuller CM. The influence of neighborhood chacacteristics on the relationship between discrimination and increased drug-using social ties among illicit durg users. J Community Health. 2013;38:328-37. [ Links ]
30. Schomerus G, Corrigan PW, Klauer T, Kuwert P, Freyberger H, Lucht M. Self-estigna in alcohol dependence: Consequences for drinking-refusal self-efficacy. Drug Alcohol Dependence. 2011;114:12-7. [ Links ]
31. Luoma JB, Kulesza M, Hayes SC, Kohlenberg B, Larimer M. Stigma predicts residential treatment length for substance use disorder. Am J Drug Alcohol Abuse. 2014; 40(3):206-12. [ Links ]
Recebido: 17.01.2017
Aceito: 31.07.2018
Autor de correspondência:
Carla Aparecida Arena Ventura
E-mail: caaventu@eerp.usp.br
https://orcid.org/0000-0003-0379-913X


{kind=link}
{kind=link}
{kind=link}
{kind=link}