










Services on Demand
article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
On-line version ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.14 no.3 Ribeirão Preto Jul./Sept. 2018
http://dx.doi.org/10.11606/issn.1806-6976.smad.2018.000407
REVIEW ARTICLE
DOI: 10.11606/issn.1806-6976.smad.2018.000407
Healthcare of women crack users during pregnancy: bibliographic review
Cuidado de mujeres usuarias de crack en la gestación: revisión bibliográfica
Mariana Cristina Lobato RibeiroI; Barbara Bartuciotti GiustiII; Suely Itsuko CiosakII; Ivanilde Marques da SilvaIII
IUniversidade Nove
de Julho, São Paulo, SP, Brazil
IIUniversidade de São Paulo, Escola de Enfermagem,
São Paulo, SP, Brazil
IIIUniversidade Adventista de São Paulo, São Paulo,
SP, Brazil
ABSTRACT
OBJECTIVE: to raise and analyze the literature
contributions related to this theme.
METHOD: an integrative review was
performed in the Lilacs and Pubmed databases, considering studies published
between 2006 and 2017, in Portuguese, English and Spanish languages, from the
intersection of the descriptors: harm reduction, Cocaine, Crack and Gestation.
CONCLUSION: the scientific literature prioritizes the epidemiological analysis
of the phenomenon and the consequences of drug use in the concept, but little
explores strategies of clinical and psychosocial care.
Descriptors: Pregnancy; Crack Cocaine; Cocaine; Harm Reduction.
RESUMEN
OBJETIVO: levantar y analizar las contribuciones de la literatura
relacionadas con la temática.
MÉTODO: se realizó una revisión integrativa, en
las bases de datos Lilacs y Pubmed, considerando estudios publicados entre 2006
y 2017, en los idiomas portugués, inglés y español, a partir del cruce de los
descriptores: reducción de daños, Cocaína, Crack y Gestación.
CONCLUSIÓN: la
literatura científica prioriza el análisis epidemiológico del fenómeno y las
consecuencias del uso de drogas en el concepto, pero poco explora las
estrategias de atención clínica y psicosocial.
Descriptores: Embarazo; Crack Cocaína; Cocaína; Reducción de Daños.
Introduction
Gestation and puerperium represent important moments in the family life cycle, producing specific changes and demands and becoming a moment that is propitious for the development of preventive and promotion actions of health in Primary Health Care (PHC)(1).
At the beginning of the 1990s, the Family Health Strategy (FHS) emerged in Brazil as a tool for reorienting the care model based on PHC. The FHS was to act in accordance with the principles of the Unified Health System - SUS(2) and based its practice on the central and derivative attributes of PHC.
Since the insertion of low-risk prenatal care as an essential attribute of the FHS, the coverage of prenatal care increased in Brazil(1), facilitating the access of pregnant women and their families to care in a timely manner (first trimester of pregnancy), as well as the coordination of the actions of puerperal care and childcare with the same family health team(3). Even in situations where pregnant women need to be followed-up in high-risk prenatal services, it is essential that they maintain the bond with their PHC team(4), ensuring that care be coordinated by a team that knows their family, community and social context.
The FHS faces challenges associated with the growing difficulties of social cohesion observed in the last decades in its assigned territories: socioeconomic inequality, internal migrations, rapid and disorderly urbanization, collapse of respect for the law and local economy based on drugs(5). These challenges are present in prenatal care and the need to provide assistance to pregnant women in situations of chemical dependence(6), particularly Crack users, is a frequent situation.
Crack is produced by "cooking" a cocaine base paste, combined with various substances; when burned, it produces a crackling noise(7). The start of the effect of this drug is rapid and fleeting(8). Two decades after the introduction of the first report of crack use in São Paulo, the formulation of the drug has changed; substances have been added in order to reduce the production cost, which makes it increasingly difficult to describe its effects(8). There are several forms of use to consume it, such as cans, bottles and pipes, and it is common to share the tools used, increasing the risk of infections, such as viral hepatitis(9).
Socio-demographic data describe crack users as predominantly young, nonwhite people, with low schooling and low socioeconomic status and lack of formal employment(9-10). Crack is a drug associated with the culture of marginalization and social exclusion(8,11). In a study conducted in the capitals of Brazil, more than half of the participants reported that the main motivation to try the drug was the desire/curiosity to feel the effects. Peer pressure was reported by 26.7% of the interviewees and 29.2% stated that one of the reasons to use the drug was family problems or affective losses(9).
Among women users of crack and similar products analyzed in the same study(9), about 10% reported being pregnant at the moment of the interview and more than half had already become pregnant at least once after starting using the drug use.
International studies point to sexual abuse in childhood and adolescence as a major predictor of patterns of abuse and dependence of different drugs in adulthood and, in national studies, 44.5% of the women crack users interviewed reported having suffered sexual violence(9). A study conducted in England with women abusers of psychoactive substances found that 66% of the interviewed women had had sex without condoms and 55% reported having been sexually coerced at some point. High rates of sexually transmitted diseases (STDs), changes in cervical cytology, unplanned pregnancies and abortions, induced and spontaneous, were observed(12).
Studies investigating the effects of crack in pregnancy have pointed to the occurrence of placental abruption, premature delivery, and cardiopulmonary risks to the pregnant women. As for the newborn, respiratory, cardiovascular and neurological complications have been described, as well as intrauterine growth restriction, acute intoxication and withdrawal syndrome. The drug passes the placental and blood-brain barrier without prior metabolization These complications are not restricted to the immediate postpartum because the drug reaches breast milk, producing cognitive deficits and causing damages to motherhood(6,13). However, studies that point out these alterations should be interpreted with caution because the abuse of crack and cocaine is usually accompanied by maternal and socioeconomic risk factors(4,14).
The approach to crack users is complex. The reduction/discontinuation of use is a decision of the drug addicted, and despite the known harm, this is not a simple decision to make(15). It is a decision influenced by several aspects such as emotional state, difficulty to adhere to outpatient treatment, environmental stimuli, narcissistic traits and denial(16). In particular, the fissure, the intense desire to obtain the drug after a period of abstinence, causes great physical and psychological discomforts and can lead users to antisocial behaviors(16). This characteristic makes strategies such as hospitalization less effective; after hospitalization many patients experience relapses(17).
Harm Reduction (HR) strategies are usually more successful because they focus on minimizing the adverse consequences of drug misuse. In this case, the strategy stems from a undeniable reality, i.e., not trying to deny it or to modify it by imposition, or by moral or ethical discourses(17). Treating chemical dependents as ordinary people opens a door for dialogue and bonding, respecting the individual and improving his quality of life(17).
Once gestation is established, the ideal would be the immediate suspension of the use of crack and other drugs, such as alcohol and tobacco(4). However, this is a complex decision, as well as is the role of the professionals who care for these women, since in the prenatal or mental health protocols of PHC there are no recommendations regarding the management of pregnant women who use crack or cocaine. Therefore, in this study, we sought to identify in the scientific literature the basis for the care of these pregnant women.
Objective
This study aimed to perform an integrative review on the use of crack and cocaine in pregnant women and the possible strategies of specific clinical and psychosocial care for this population.
Methodology
This is an exploratory research of a bibliographical character, developed from an integrative review of articles, with the following research question: What are the contributions of the scientific literature about care for pregnant women who use crack- cocaine?
An integrative review uses methodologies that provide the synthesis of existing knowledge on a given theme by means of structured techniques of analysis of scientific data platforms(18-19).
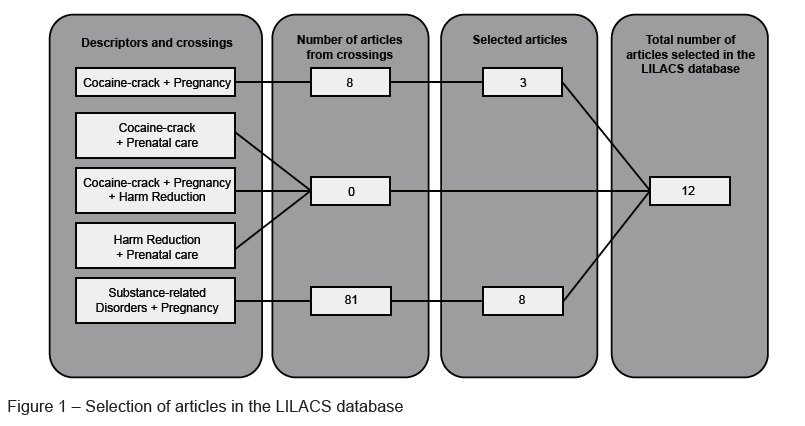
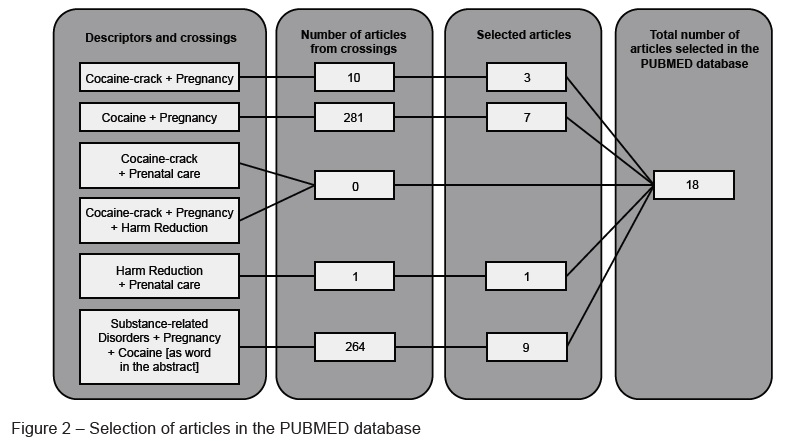
The present bibliographic search was carried out from June to July 2017 through the crossings of keywords, as descriptors and words of the abstracts: Harm Reduction; Cocaine; Crack; Pregnancy; and Substance-related Disorders in the PUBMED and LILACS databases, published in Portuguese, English and Spanish, considering publications between 2006 and 2017. The inclusion criteria were: articles addressing care for pregnant women users of cocaine and crack cocaine. The exclusion criteria were: articles not addressing this theme. A first selection of texts was made by reading the titles and the abstracts of the articles found in each search; then, the texts were later analyzed in full length. The process of selection of articles is presented in Figures 1 and 2. At the end of this process, we obtained the final sample of 30 articles:
Results
The process of selection of articles for this study evidenced that the topic of care of pregnant women who are users of crack-cocaine has been little studied. Most of the articles found did not address this theme, but the effects of maternal drug use on the fetus or make epidemiological analyses of the phenomenon. Only articles that addressed the care of these pregnant women were selected for this study.
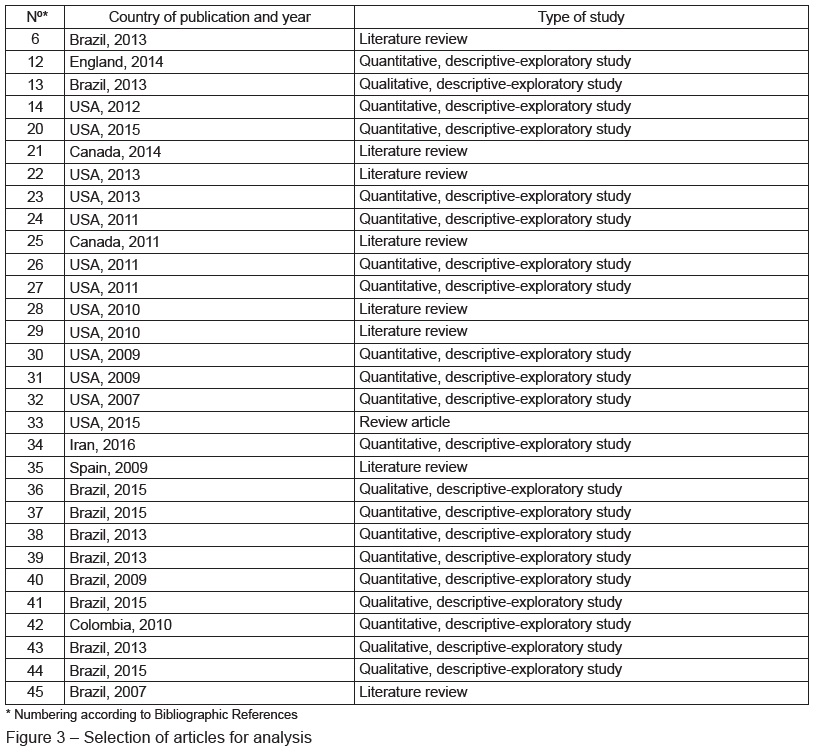
Figure 3 shows the year and country of the publication selected and the type of study.
The topics related to the care of pregnant women using crack-cocaine in the selected studies included the following aspects:
1) Consideration of high gestational risk - risk of maternal and fetal complications:
The high prevalence of the association between gestation and use of psychoactive substances, such as crack-cocaine in different parts of the world(12,15,20,23,28-29,41);
Higher overall mortality in the population of pregnant women using crack than in the population of pregnant women in general(15,35);
Obstetric and neonatal complications: preeclampsia and eclampsia, placental abruption, intrauterine growth retardation of the fetus, maternal malnutrition, prematurity, low birth weight, early neonatal jaundice, and congenital syphilis(15,20-22,28 -29.34,43);
2) Contextualization of gestational complications:
Gestational complications and sequelae in the fetus should be interpreted and associated with other maternal and socioeconomic risk factors(21 31,33-35);
Phenomena such as unemployment, poor housing, poor diet and other aspects related to social vulnerability are frequently observed in this population(36-37,39-41);
Low adherence to prenatal care among women who use crack and/or cocaine, with possible influence on the negative outcomes observed (gestational complications and sequelae in the fetus)(4,31,41,43);
Distrust of the patients toward professionals for fear of being reported to police authorities and disbelief in the results of care(31,43);
Frequent association between abusive use of psychoactive substances (including crack cocaine) with sexual risk behaviors, prostitution and physical and sexual violence (12,36,39-40);
Frequent association between crack-cocaine use, gestation and depressive symptoms, posttraumatic stress and suicidal tendency(22,24,30,38,42);
Use of alcohol and other drugs among family members; little or no family support during pregnancy(36-38,44-45);
High prevalence of postpartum relapse(20);
3) Reorganization of the practice for prenatal care in this population:
Given the frequent association of multiple substance use among crack-cocaine users, the use of a substance such as tobacco and/or alcohol is indicated serve as an alert to investigate the use of other substances, such as crack(22-23,37);
The use of flexible care systems for this population is emphasized(25);
The use of community resources for care is encouraged(25);
It is identified that the association of different strategies of clinical approach to this population, such as Cognitive-Behavioral Therapy, the 12 steps and approaches of community reinforcement have better results, with reduction of drug use and better adherence to prenatal care(27-28,32);
Discussion
Although the use of crack and cocaine during gestation is described in the literature as a growing phenomenon(6,9,13,15), few studies have advanced towards the possibilities of specific care for this population during gestation. No studies on the clinical management of pregnant women using cocaine and crack were identified. Although the HR policy guidelines are protected by the Article 196 of the Federal Constitution, as an intervention of prevention, assistance, and promotion of health and human rights(17), there are no recommendations on the operationalization of these actions aimed at pregnant women.
Likewise, there are no recommendations of the Ministry of Health (MOH) regarding the assistance to be provided to these women during pregnancy. However, some measures have been taken, such as the creation of Street Medical Offices which have as guiding principles the respect for differences, the promotion of human rights and social inclusion, fight against stigma, HR actions and intersectoriality(4). Just like in PHC, Street Medical Offices make care accessible to these women, based on the on-site care provided.
The studies analyzed point to several recurrent gestational complications among pregnant women who use crack-cocaine(15,20-22,28-29,34,43), but the text of the Technical Manual of High Risk Prenatal Care is limited to the recognition of the problem, without pointing out suggestions for the care of this population. The use of illicit drugs in pregnancy is still taboo, both in academic community and in public policy.
Due to stigmatization, it is common to see pregnant women denying the use of drugs during prenatal consultations(13,21,28). It is important that the professionals involved in the care be open to embrace and listen to these patients. This same attitude should guide the creation of therapeutic plans(46). Without building a relationship of partnership, one that values the beliefs and world views of these women, effective planning is not possible.
The studies analyzed in this review, as well as other publications(47-48), state the fundamental importance of contextualization to understand the gestational complications associated with the use of crack-cocaine. The social context of this population is often extremely vulnerable. Besides poverty, which is often reflected in poor diet and insecure housing(47-48), phenomena such as use of psychoactive substances by other family members(47-48), family breakdowns(9,48), domestic violence(12,43), sexual violence(12), use of multiple psychoactive substances(22-23,43), association with other mental health complications(22,24,30) and low prenatal adherence(31) are also frequent.
Thus, associating the complications observed in these pregnant women exclusively with the use of crack-cocaine only reproduces stigmatization, and underestimate the analysis of the phenomenon its full complexity. Likewise, clinical recommendations that are restricted to the abandonment of drug use(4) are also inefficient because they increase the possibility of the pregnant women to distrust the health care team which assists them, creating obstacles to open communication and shared planning of scientifically based actions such as harm reduction.
On the other hand, there are no studies that support the progressive reduction of drug use or its use in an alternative manner during pregnancy; there are no studies that establish safe limits for the use of these substances during pregnancy. Still, stipulating total suspension as the only alternative can create on the women an expectation of psychic suffering, anguish and possibly rupture in the therapeutic bond. In view of these aspects, HR strategies may be of fundamental importance because they recognize abstinence as important, but does not consider it the only alternative.
Among the few proposals to reorganize the care practices for these women identified in this review(46) is the focus on making more flexible agendas and the maintenance of the bond of the women with family health workers, especially in the coordination of care. The studies analyzed in this review point out that drug addiction has a strong relation with the family and social context(21,31,33-38,44-45). The role of PHC in coordinating the care of these pregnant women is crucial because the family focus and the community focus(49) are equally important to ensure that the phenomenon be known and fully addressed.
In addition, longitudinality provides an individualized therapeutic relationship. Knowing deeply not only the women but their families and community, as well as being recognized as a reference, either as a professional or as a team, for health care for this population legitimizes the role of the professionals and their health care proposals. This approach is characteristic of PHC(39). Maintaining the bond of the pregnant women users of crack-cocaine with their PHC team guarantees not only comprehensive assistance during prenatal care but also the accompaniment of the children in their neuro-psychomotor development and weight gain within their socio-cultural context( 1).
Conclusion
During this study, the great challenge inherent to the cultural, social, demographic and economic changes of the last decades is evident. However, research with pregnant women who are crack users and other drugs has prioritized the epidemiological analysis of the phenomenon and its consequences in the fetus. The care for women who use crack and other drugs during pregnancy has been poorly studied; there is therefore little evidence of research on specific recommendations for this population. Hence, the importance of specific public health policies and the creation of care strategies in different levels of health care directed at these women and their families, considering the guidelines for perinatal care in line with the care for Chemical Dependency; always considering the women as part of the Care project. In addition, it is fundamental that the academic community and health professionals consider this increasingly frequent theme in the practice of PHC and in the other loci of perinatal care.
Acknowledgements
To the community of UBS Vila Dalva, which provided us with learning and a special look for care with Chemical Dependents.
References
1. Ministério da Saúde (BR). Grupo Hospitalar Conceição. Gerência de Saúde Comunitária - Atenção à saúde da gestante em APS. Porto Alegre; 2011. [ Links ]
2. Rosa WAG, Labate RC. The Family Health Program and the construction of a new model for primary care in Brazil. Rev. Latino-Am. Enfermagem. 2005;13(6):1027-34. [ Links ]
3. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Área Técnica de Saúde da Mulher. Pré-natal e Puerpério: atenção qualificada e humanizada – manual técnico. Brasília: Ministério da Saúde; 2006.
4. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Gestação de alto risco: manual técnico. 5ed. Brasília : Editora do Ministério da Saúde; 2010. [ Links ]
5. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica: Saúde mental. Brasília: Ministério da Saúde; 2013. [ Links ]
6. Martins-Costa SH, Vettorazzi J, Cecin GKG, Maluf JMRA, Stumpf CC, Ramos JGL. Crack: a nova epidemia obstétrica. Rev HCPA. 2013;33(1):55-65. [ Links ]
7. Kessler F, Pechansky F. Uma visão psiquiátrica sobre o fenômeno do crack na atualidade. Rev Psiquiatr RS. 2008;30(2):96-8. [ Links ]
8. Oliveira LG, Nappo SA. Crack na cidade de São Paulo: acessibilidade, estratégias de mercado e formas de uso. Rev Psiq Clín. 2008;35(6):212-8. doi: 10.1590/S0101-60832008000600002 [ Links ]
9. Ministério da Saúde (BR). Ministério da Justiça. Secretaria Nacional de Políticas sobre Drogas. FIOCRUZ. Estimativa do número de usuários de crack e/ou similares nas Capitais do País: Livreto Domiciliar. Rio de Janeiro; 2013. [Acesso 22 ago 2018]. Disponível em: http://portal.mj.gov.br/services/DocumentManagement/FileDownload.EZTSvc.asp?DocumentID={9B17D77F-C442-4B2B-8705-117920F30C6F}&ServiceInstUID={74624DEB-0C14-4B3A-B8F3-CD26DEF53FC1}. [ Links ]
10. Oliveira LG, Nappo SA. Caracterização da cultura de crack na cidade de São Paulo: padrão de uso controlado. Rev Saúde Pública. 2008;42(4):664-71. doi: 10.1590/S0034-89102008005000039. [ Links ]
11. Araujo RA, Pansard M, Boeira BU, Rocha NS. As estratégias de coping para o manejo da fissura de dependentes de crack. Rev HCPA. 2010;30(1):36-42. [ Links ]
12. Edelman NL, Patel H, Glasper A, Bogen-Johnston L. Sexual health risks and health-seeking behaviours among substance-misusing women. J Adv Nurs. 2014 Dec;70(12):2861-70. doi: 10.1111/jan.12442. [ Links ]
13. Kassada DS, Marcon SS, Pagliarini MA, Rossi RM. Prevalência do uso de drogas de abuso por gestantes. Acta Paul Enferm. 2013; 26(5):467-71. doi: 10.1590/S0103-21002013000500010 [ Links ]
14. Hser YI, Kagihara J, Huang D, Evans E, Messina N. Mortality among substance-using mothers in California: a 10-year prospective study. Addiction. 2012 Jan;107(1):215-22. doi: 10.1111/j.1360-0443.2011.03613.x [ Links ]
15. Chaves TV, Sanchez ZM, Ribeiro LA, Nappo SA. Fissura por crack: comportamentos e estratégias de controle de usuários e ex-usuários. Rev Saúde Pública. 2011; 45(6):1168-75. Doi: 10.1590/S0034-89102011005000066 [ Links ]
16. Ferreira ACZ, Capistrano FC, Maftum MA, Kalinke LP, Kirchhof ALC. Caracterização de Internações de Dependentes Químicos em uma Unidade de Reabilitação. Cogitare Enferm. 2012; 17(3):444-51. doi: 10.5380/ce.v17i3.29284. [ Links ]
17. Universidade Federal de São Paulo (UNIFESP). Ministério da Saúde (BR). Programa de Orientação e Atendimento a Dependentes (PROAD). Drogas e Redução de Danos: uma cartilha para profissionais de saúde. São Paulo; 2008. [ Links ]
18. Souza MT, Silva MD, Carvalho R. Integrative review: what is it? How to do it?. Einstein. (São Paulo) [Internet]. 2010 Mar [cited 2018 Aug 10]; 8(1):102-6. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1679-45082010000100102&lng=en. http://dx.doi.org/10.1590/s1679-45082010rw1134. [ Links ]
19. Mendes KDS, Silveira RCCP, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto Contexto Enferm. 2008 Dec; 17(4): 758-64. Doi: 10.1590/S0104-07072008000400018. [ Links ]
20. Forray A, Merry B, Lin H, Ruger JP, Yonkers KA. Perinatal substance use: a prospective evaluation of abstinence and relapse. Drug Alcohol Depend. 2015 May 1;150:147-55. doi: 10.1016/j.drugalcdep.2015.02.027 [ Links ]
21. Cressman AM, Natekar A, Kim E, Koren G, Bozzo P. Cocaine abuse during pregnancy. J Obstet Gynaecol Can. 2014 Jul;36(7):628-31. [ Links ]
22. Cain MA, Bornick P, Whiteman V. The maternal, fetal, and neonatal effects of cocaine exposure in pregnancy. Clin Obstet Gynecol. 2013 Mar;56(1):124-32. doi: 10.1097/GRF.0b013e31827ae167. [ Links ]
23. Gaalema DE, Higgins ST, Pepin CS, Heil SH, Bernstein IM. Illicit drug use among pregnant women enrolled in treatment for cigarette smoking cessation. Nicotine Tob Res. 2013 May; 15(5):987–91. https://doi.org/10.1093/ntr/nts220
24. Rubin LH, Cook JA, Grey DD, Weber K, Wells C, Golub ET, et al. Perinatal depressive symptoms in HIV-infected versus HIV-uninfected women: a prospective study from preconception to postpartum. J Womens Health. (Larchmt). 2011 Sep;20(9):1287-95. doi: 10.1089/jwh.2010.2485 [ Links ]
25. Wong S, Ordean A, Kahan M. Substance use in pregnancy. J Obstet Gynaecol Can. 2011 Apr;33(4):367-84. doi: 10.1080/08897077.2011.598399
26. Jones HE, O’Grady KE, Tuten M. Reinforcement-based treatment improves the maternal treatment and neonatal outcomes of pregnant patients enrolled in comprehensive care treatment. Am J Addict. 2011 May-Jun;20(3):196-204. doi: 10.1111/j.1521-0391.2011.00119.x
27. Schottenfeld RS, Moore B, Pantalon MV. Contingency management with community reinforcement approach or twelve-step facilitation drug counseling for cocaine dependent pregnant women or women with young children. Drug Alcohol Depend. 2011 Oct 1;118(1):48-55. doi: 10.1016/j.drugalcdep.2011.02.019. [ Links ]
28. Hull L, May J, Farrell-Moore D, Svikis DS. Treatment of cocaine abuse during pregnancy: translating research to clinical practice. Curr Psychiatry Rep. 2010 Oct;12(5):454-61. doi: 10.1007/s11920-010-0138-2. [ Links ]
29. Keegan J, Parva M, Finnegan M, Gerson A, Belden M. Addiction in pregnancy. J Addict Dis. 2010 Apr;29(2):175-91. doi: 10.1080/10550881003684723. [ Links ]
30. Eggleston AM, Calhoun PS, Svikis DS, Tuten M, Chisolm MS, Jones HE. Suicidality, aggression, and other treatment considerations among pregnant, substance-dependent women with posttraumatic stress disorder. Compr Psychiatry. 2009 Sep-Oct;50(5):415-23. doi: 10.1016/j.comppsych.2008.11.004. [ Links ]
31. Schempf AH, Strobino DM. Drug use and limited prenatal care: an examination of responsible barriers. Am J Obstet Gynecol. 2009; 200(4):412.e1-10. doi: 10.1016/j.ajog.2008.10.055. [ Links ]
32. Svikis DS1, Silverman K, Haug NA, Stitzer M, Keyser-Marcus L. Behavioral strategies to improve treatment participaion and retention by pregnant drug-dependent women. Subst Use Misuse. 2007;42(10):1527-35. [ Links ]
33. McAllister D, Hart CL. Inappropriate interpretations of prenatal drug use data can be worse than the drugs themselves. Neurotoxicol Teratol. 2015;52(Pt A):57. http://dx.doi.org/10.1016/j.ntt.2015.07.002 [ Links ]
34. Aghamohammadi A, Zafari M. Crack abuse during pregnancy: maternal, fetal and neonatal complication. J Matern Fetal Neonatal Med. 2016 Mar;29(5):795-7. doi: 10.3109/14767058.2015.1018821 [ Links ]
35. Ruoti CM , Ontano M, Calabrese E , Airaldi L, Gruhn E, Galeano J, et al. Uso y abuso de drogas durante el embarazo. Mem. Inst. Investig. Cienc. Salud. 2009;7(2):32-44. [ Links ]
36. Rodrigues MP, Zerbetto SR, Ciccillini MF. Percepção da equipe de enfermagem sobre os fatores de risco para o consumo de drogas pelas gestantes. SMAD, Rev. Eletrônica Saúde Mental Álcool Drog.[Internet]. 2015 [Acesso 2 jun 2017]; 11(3):153-60. Disponível em: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1806-69762015000300006&lng=pt&nrm=iso&tlng=pt [ Links ]
37. Lima LPM, Santos AAPS, Póvoas FTX, Silva FCL. O papel do enfermeiro durante a consulta de pré-natal à gestante usuária de drogas. Rev Espaço para a Saúde. 2015; 16(3):39-46. [ Links ]
38. Viellas EFV, Gama SGN, Carvalho ML, Pinto LW. Factors associated with physical agression in pregnant women and adverse outcomes for the newborn. J Pediatr. 2013;89(1):83-90. [ Links ]
39. Faler CS, Câmara SG, Aets DRGC, Alves GG, Béria JU. Family psychosocial characteristics, tobacco, alcohol, and other drug use, and teenage pregancy. Cad Saúde Pública. 2013;29(8):1654-63. [ Links ]
40. Bassols AMS, Boni R, Pechansky F. Alcohol, drugs, and risky sexual behavior are related to HIV infection in female adolescents. Rev Bras Psiquiatria. 2010;32(4):361-8. [ Links ]
41. Nicolli T, Gehlen MH, Ilha S, Diaz CMG, Machado KFC, Nietsche EA. Teoria do autocuidado na desintoxicação química de gestantes em uso de crack: contribuições da enfermagem. Esc Anna Nery. 2015;19(3):417-23. [ Links ]
42. Vélez ML, Jansson LM. Síndrome de estrés postraumático en mujeres embarazadas abusadoras de drogas. Rev Colomb Psiquiatr. [Internet]. 2010 [Acesso 2 jun 2017]; 39(supl): 84-92. Disponível em: http://www.elsevier.es/es-revista-revista-colombiana-psiquiatria-379-avance-resumen-sindrome-estres-postraumatico-mujeres-embarazadas-S0034745014602699 [ Links ]
43. Portela GLC, Barros LM, Frota NM, Landim APP, Caetano JÁ, Farias FLRF. Perception of pregnant on consuption of illicit drugs in pregnancy. SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. 2013 [cited 2017 Jun 2]; 9(2):58-63. Available from: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1806-69762013000200002&lng=pt&nrm=iso&tlng=pt [ Links ]
44. Reis FT, Loureiro RJ. O uso de crack durante a gestação e suas repercussões biopsicossociais e espirituais. SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. 2015 [Acesso 2 jun 2017]; 11(2):105-11. Disponível em: http://pepsic.bvsalud.org/scielo.php?pid=S1806-69762015000200007&script=sci_arttext&tlng=pt [ Links ]
45. Rodrigues DT, Nakano MAS. Violência doméstica e abuso de drogas na gestação. Rev Bras Enferm, Brasília. 2007; 60(1):77-80. [ Links ]
46. Botelho AAM, Rocha RC, Melo VH. Uso e dependência de cocaína/crack na gestação, parto e puerpério. Femina. [Internet]. 2013 [Acesso 21 ago 2018];41(1). Disponível em: http://files.bvs.br/upload/S/0100-7254/2013/v41n1/a3777.pdf [ Links ]
47. Yabuuti PLK, Bernardy CCF. Perfil de gestantes usuárias de drogas atendidas em um Centro de Atenção Psicossocial. Rev Baiana Saúde Pública. [Internet]. 2014 [Acesso 2 jun 2017];38(2):344-56. Disponível em: http://inseer.ibict.br/rbsp/index.php/rbsp/article/view/53 [ Links ]
48. Marangoni SR, Oliveira MLF. Uso de crack por multípara em vulnerabilidade social: história de vida. Cienc Cuid Saúde. 2012;11(1):166-72. [ Links ]
49. Starlfield B. Atenção primária: equilíbrio entre necessidades de saúde, serviços e tecnologia. Brasília: UNESCO, Ministério da Saúde; 2002. [ Links ]
Received: Aug 4th 2017 Corresponding author:
Accepted: Aug 17th 2018
Mariana Cristina Lobato Ribeiro
E-mail: marianalobatorb@gmail.com
https://orcid.org/0000-0002-180-8276


{kind=link}
{kind=link}
{kind=link}