










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versión On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.16 no.1 Ribeirão Preto enero/mar. 2020
http://dx.doi.org/10.11606/issn.1806-6976.smad.2020.153349
ORIGINAL ARTICLE
Lipid profile and alcohol consumption: longitudinal study on adults' health (ELSA-BRASIL)*
Ludmila Macêdo NaudI,II ; Isabela Judith Martins BensenorIII; Paulo Andrade LotufoIV
; Isabela Judith Martins BensenorIII; Paulo Andrade LotufoIV
IUniversidade de São Paulo, Faculdade de Saúde Pública, Departamento de Epidemiologia, São Paulo, SP, Brazil
IIMinistério da Saúde, Comissão Nacional de Ética em Pesquisa, Brasília, DF, Brazil
IIIUniversidade de São Paulo, Faculdade de Saúde Pública, São Paulo, SP, Brazil
IVUniversidade de São Paulo, Faculdade de Medicina, São Paulo, SP, Brazil
ABSTRACT
OBJECTIVE: to investigate the effect of general alcohol consumption and of the type of alcoholic beverage consumed, in different lipid measurements.
METHOD: the effect of alcohol consumption as well as that of the type of alcoholic beverage consumed were investigated, in different lipid measurements, for the participants in the Longitudinal Study on Adults' Health for both sexes.
RESULTS: analyses were conducted on the type and amount of alcoholic beverage consumed by sex. Low-to-moderate alcohol consumption, regardless of the type of alcoholic beverage, resulted in higher levels of HDL-cholesterol, HDL2- cholesterol and HDL3-cholesterol in males and females. No participants in the study consumed low-to-moderate amounts of spirits. Triglycerides showed inverse effects for men and women according to the lipid profile. For men, spirits contributed to a better triglyceride profile while for women it was the opposite. Men who consumed spirits showed lower triglyceride levels, and women who consumed that beverage type had higher levels. Our results are in agreement with those of previous studies.
CONCLUSION: alcohol consumption resulted in different levels of serum lipid measurements in men and women. Thus, it is concluded that response to alcohol has biological differences.
Descriptors: Alcoholism; Fats; Lipoproteins, HDL; Sex Distribution.
Introduction
Some prospective studies have found that low-to-moderate constant alcohol consumption would be associated with reduced risk for coronary disease(1-4) and that such reduction would be related to the beneficial effects of alcohol on lipids, particularly on HDL-cholesterol(5-7). The protective effects of alcohol against coronary disease would be mediated by increased HDL-cholesterol(8). Although less frequently, reduced LDL-cholesterol has also been reported and, in addition to HDL-cholesterol and LDL-cholesterol, alcohol has also been shown to change triglycerides levels. On average, for each extra gram of alcohol consumed a day, triglycerides increased by 0.19mg/dL(9-10).
Most of these studies have evaluated the effects of alcohol and the onset of disease; however, the influence of different types of alcoholic beverages on plasma lipid levels has been investigated to a lesser extent and in specific populations. In general, male individuals or the effects of alcohol consumption on populations that are dependent on the substance are studied. To our knowledge, this is the only study to investigate the association between alcohol consumption and lipid measurements in such a large Brazilian sample, comparing the effects on men and women.
Experimental and cross-sectional studies have reported the beneficial effects of alcohol consumption on HDL-cholesterol regardless of the type of alcoholic beverage consumed, but in relation to alcohol consumption itself, they have suggested that non-alcoholic components, such as antioxidant polyphenols in red wine, would be responsible for the cardioprotective effect(9,11-13). The aim of this study was to investigate the effect of alcohol consumption in general, as well as that of the type of alcohol beverage consumed on different lipid measurements.
Method
ELSA-Brasil
ELSA-Brasil is a cohort with 15,105 participants aged 35 to 74 years in six Brazilian cities. The population comprises active and retired professors and employees from six Brazilian research institutions: Federal University of Rio Grande do Sul, University of São Paulo, Federal University of Minas Gerais, Oswaldo Cruz Foundation, Federal University of Bahia and Federal University of Espirito Santo(6). Briefly, out of 15,105 participants evaluated in 2008-10, 4,979 of them had their lipid profiles measured by the Vertical Auto Profile (VAP) test at the São Paulo State Collection Center(7). Individuals who had no alcohol consumption data were excluded, thus totaling the 4,976 people analyzed in this study.
Each participant responded to an interview according to a standard protocol. The interviews and tests were conducted by interviewers trained in strict quality control. ELSA-Brasil was approved by the Research Ethics Committee of the University of São Paulo Hospital (CEP-HU) under CEP-HU Registration no. 659/06 and, at the same time, under SISNEP Registration no. FR-93920. Following the creation of the Brazil Platform, ELSA-Brasil was approved by Conep with CAAE Registration no. 08109612.7.1001.0076, and all the participants involved in this study signed an Informed Consent Form.
Lipoprotein and LDL subclass measurements
Blood collection occurred after a 12-hour night fasting period. The blood samples were centrifuged at the local center and stored in tubes at -80 ºC. A complete lipoprotein profile that included plasma cholesterol, HDL-cholesterol, HDL2-cholesterol, HDL3- cholesterol, lipoprotein A, real LDL (LDL-cholesterol without IDL and lipoprotein A), IDL-cholesterol and VLDL-cholesterol for each individual was determined using the Vertical Auto Profile - VAP methodology (Atherothech®, Birmingham, Alabama, USA). VAP is a direct measurement method with no estimates involved. It is based on the combination of ultracentrifugation and a continuous flow enzymatic cholesterol analyzer that is highly sensitive and reproducible.
Subclass cholesterol profile analysis was performed using the LDL-VAP method, which is a modification of the VAP procedure designed to separate subclasses of LDL-cholesterol ranging from LDL1-cholesterol to LDL4-cholesterol.
Alcohol consumption
To evaluate the consumption of alcoholic beverages (beer, wine, spirits), the Alcohol Use Questionnaire, structured with closed questions and based on the National Center for Health Statistics questionnaire, was used. The drinking pattern and weekly frequency of alcohol consumption was determined based on this questionnaire.
To calculate the amount of ethanol in grams, the mean percentage of alcohol of the most common beverage brands in the market was used: beer: 6%, wine: 12% and distillates: 39%. Firstly, the amount reported weekly by the measurement in mL was determined and then the amount of pure alcohol intake in mL/week was calculated according to the alcohol concentration in each beverage. They were subsequently added to the amount of alcohol consumed in beverage types and then multiplied by the ethanol density (0.8) to obtain the total amount of pure ethanol in grams per week. People who consumed alcohol excessively were categorized as those who had ethanol consumption greater than or equal to 210g/week for males and greater than or equal to 140g/week for females.
Statistical analysis
All statistical analyses were performed using the SPSS software, version 17. Because of the different drinking patterns between men and women and their variations in lipid measurements, all analyses were conducted separately. Normality analysis was performed using the Kolmogorov-Smirnov test.
Alcohol consumption was taken as the categorical variable (low-to-moderate and excessive). Low-to-moderate categories were defined differently by sex according to the US Department of Agriculture Dietary Guidelines 2005, for men: low-to-moderate was less than or equal to 210g/week, and excessive was greater than 210g/week, while for women, low-to-moderate was less than or equal to 140g/week and excessive was greater than 140 grams per week.
When considering the specific type of alcoholic beverage consumed, consideration was given to individuals who were not only prone to consume just one type of beverage, but who also consumed different types of wine, beverage or spirits. For that purpose, a particular predominant type of alcoholic beverage was defined if the consumption of this specific type of beverage totaled two thirds or more of the total amount of ethanol consumed.
To compare the types of beverages consumed (abstainers, consumers of wine, beer, spirits or mixed), the One-Way ANOVA test was used. To compare low-to- moderate drinkers with excessive drinkers for each type of beverage, Student's t test was performed.
Results
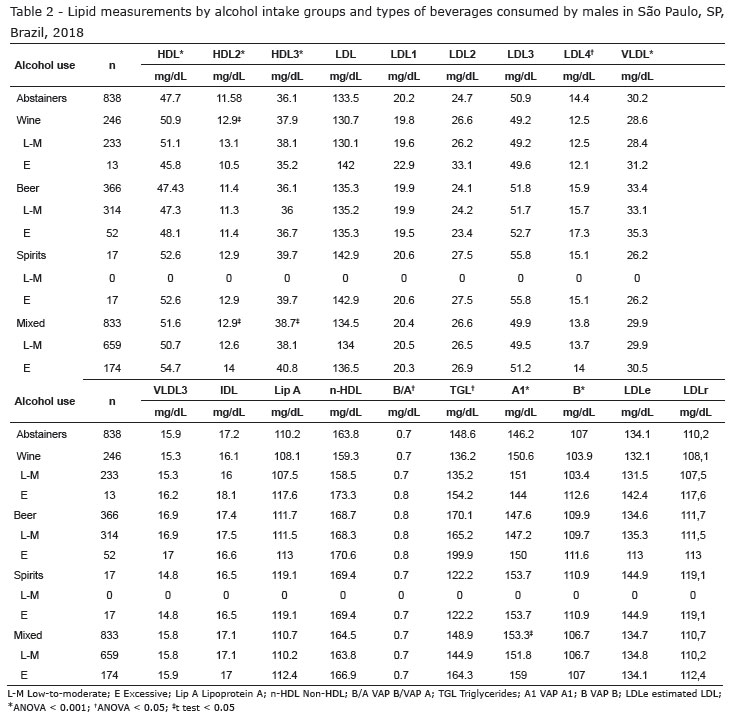
The mean lipid measurements for each sex stratum are shown in Tables 1, 2 and 3. The values are divided according to the amount of alcohol consumption and the type of alcoholic beverage consumed. HDL-cholesterol, HDL2-cholesterol, HDL3-cholesterol, LDL4-cholesterol, VLDL-cholesterol, VLDL3-cholesterol, VAP B/VAP A ratio, triglycerides and VAP A1 showed significant differences between abstainers and consumers of wine, beer, spirits and mixed beverages. And regarding the amount of alcoholic beverage consumed, statistically significant differences were only observed between consumers of mixed beverages, with higher values of HDL-cholesterol, HDL2-cholesterol, HDL3-cholesterol and VAP A1 for excessive consumers. For both males and females, no participants consumed spirits moderately.
Overall, there were lower levels of HDL-cholesterol among beer consumers and high levels among consumers of more than one type of alcoholic beverage; lower LDL-cholesterol values for wine consumers and higher levels for spirits consumers; lower VLDL-cholesterol values for those who consumed only spirits and higher values for those who consumed beer; lower triglyceride values for wine consumers and higher values for spirits consumers; lower VAP A1 values for spirits consumers and higher values for consumers of mixed beverages.
Regarding males, the values of HDL-cholesterol, HDL2-cholesterol, HDL3-cholesterol, LDL4-cholesterol, VLDL-cholesterol, triglycerides and VAP A1 showed statistically significant differences, and between the amounts of alcoholic beverages, a difference was observed between the amount of wine for HDL2-cholesterol and mixed beverages for HDL-cholesterol, HDL2-cholesterol, HDL3-cholesterol and VAP A1 (Table 2). In the male population, beer consumers showed lower values of HDL-cholesterol, HDL2-cholesterol and HDL3-cholesterol, and spirits consumers showed higher values; abstainers showed lower LDL2-cholesterol levels, and beer consumers showed higher levels; those who consumed more than one type of alcoholic beverage showed lower levels of IDL-cholesterol, and spirits consumers showed higher levels; consumers of more than one type of beverage showed lower triglyceride levels, and higher levels were observed for spirits consumers; spirits consumers showed lower VAP A1 levels, and consumers of mixed beverages showed higher levels.
As for females, only differences in HDL-cholesterol, HDL2-cholesterol, HDL3-cholesterol, LDL2-cholesterol, IDL-cholesterol, triglycerides and VAP A1 were shown (Table 3). Women who consumed only spirits showed lower levels of HDL-cholesterol, HDL2-cholesterol and HDL3-cholesterol, and women who consumed more than one type of alcoholic beverage showed higher levels; women who did not drink showed lower levels of LDL2-cholesterol, and women who consumed only beer showed higher levels; those who consumed more than one type of alcoholic beverage showed lower levels of IDL-cholesterol and triglycerides, and women who consumed only spirits showed higher levels; as to VAPA1, women who only consumed spirits had lower levels and women who consumed more than one type of alcoholic beverage showed higher levels.
Discussion
In this study, it was shown that alcohol consumption can result in significantly higher levels of HDL-cholesterol, HDL2-cholesterol and HDL3-cholesterol. The effect of alcohol consumption was similar for LDL2-cholesterol, IDL-cholesterol, triglycerides and VAP A1 for males and females. High consumption of spirits was associated with higher levels of IDL-cholesterol, LDL2-cholesterol and triglycerides. A difference was observed for wine consumption. Serum lipid levels, in response to wine consumption, were inverse between males and females. For females, the higher the wine consumption, the higher the levels of HDL-cholesterol, HDL2-cholesterol and HDL3-cholesterol, and for males, the opposite was found. Overall, our results have confirmed those of previous studies which associated alcohol consumption, regardless of the type of beverage, with higher levels of HDL-cholesterol, HDL2-cholesterol and HDL3-cholesterol when men and women were evaluated together. However, when stratifying by sex, opposite results were found.
The effects of alcohol consumption on lipid profiles were firstly investigated in males. Early studies involving females did not perform analyses by sex. The few studies that evaluated such relationship in separate male and female populations indicated that the association of alcohol consumption differed between men and women, and that wine consumption increased HDL-cholesterol levels in women, which corroborates our findings(11,14-15). This result may be associated with the fact that females are more sensitive to the effects of alcohol than males, especially with regard to liver function. Alcohol concentrations also differ between men and women. Higher alcohol concentrations are found in women after the intake of the same amount of alcohol. This effect is attributed to lower gastric metabolism in women. In this study, HDL-cholesterol levels were higher with spirits in males and lower in females, which had also been previously identified(16-17). Overall, differences in lipid levels and alcohol consumption were found in males and females, but these results should not be extrapolated due to the lack of more detailed metabolic and biochemical measures.
The differences in lipid response between males and females are clear. For males, there was a difference regarding the consumption amount of mixed alcoholic beverages for HDL-cholesterol, HDL2-cholesterol and HDL3-cholesterol, but not for females. Males who consumed mixed alcoholic beverages excessively were associated with higher levels of HDL-cholesterol when compared to those who consumed low-to-moderate amounts. Previous studies by ELSA-Brasil have shown the population profile and demonstrated that HDL-cholesterol, HDL2-cholesterol and HDL3-cholesterol are inversely associated with insulin resistance and subclinical inflammation(18), that alcohol consumption increased risk for high blood pressure(19) and that alcohol consumption, when associated with meals, showed a more favorable lipid profile(20).
As regards triglyceride values, they were lower for males who only consumed spirits excessively and higher for those who consumed only beer. Females who consumed mixed beverages showed lower triglyceride levels, while those who consumed them excessively had even lower levels. Women who consumed spirits showed higher triglyceride levels. Some studies show a strong relationship between alcohol intake and increased triglycerides, especially the effects that alcohol has on genetic variation, particularly on genes related to alcohol metabolism(21).
Previous studies have shown conflicting results between the relationship of alcohol consumption and LDL-cholesterol(22). It has been recently proposed that the differences may be associated with genetic variations in the apolipoprotein metabolism, particularly apolipoprotein A5 polymorphisms(21).
Although the mechanism for differences between males and females is not fully understood, they may be due to body composition, insulin and glucose metabolism and genetic factors(23). Such a contrast between the sexes is intriguing, as the exact mechanism by which alcohol affects lipid measurements remains largely unknown(8,24-27). These differences may be explained by genetic differences, and to that end, further studies are needed. Clinical and epidemiological studies suggest that it is mainly the red wine that would help protect against cardiovascular disease, atherosclerosis and metabolic syndrome, possibly because of the polyphenols found in it, such as resveratrol, anthocyanin, flavonol and catechin, which are beneficial to health. In addition, the metabolites themselves may be the main players in cardiovascular protection. In beer, xanthohumol and its metabolites isoxanthohumol and phytoestrogen 8-phenylnaringenin also have healthy properties. In addition, any healthy effects of wine and beer are greatest in combination with a healthy diet, rich in fruit, vegetables and whole grains. There is evidence that polyphenols have synergistic effects with compounds found in other food groups(28). However, it is recommended that excessive alcohol consumers or abstainers should not be encouraged to use alcohol in order to protect their lipid profiles, as the deleterious consequences of alcohol may outweigh the possible benefits involved.
The limitations of the study are due to the fact that the data collection on alcohol consumption was based on self-reporting, since especially when it comes to alcohol consumption, research participants tend to provide answers that are socially desirable. Therefore, alcohol consumption may be underestimated, especially in groups of individuals who drink excessively. The study design is also another limitation. Although ELSA-Brasil is a longitudinal investigation, this study was cross-sectional, and it is not possible to make causal inferences. Finally, the classification used could underestimate the numbers of episodic alcohol compulsion.
Conclusion
Overall, this study has shown that alcohol consumption, regardless of the type of alcoholic beverage consumed, resulted in significantly higher levels of HDL-cholesterol, HDL2-cholesterol and HDL3-cholesterol in both females and males. Alcohol consumption has been shown to contribute to a better lipid profile, which has been reported in the literature. Previous research showed an inverse association between alcohol consumption and cardiovascular disease in both males and females.
References
1. Friedman LA, Kimball AW. Coronary heart disease mortality and alcohol consumption in Framingham. Am J Epidemiol. 1986;124(3):481-9. doi.org/10.1093/oxfordjournals.aje.a114418. [ Links ]
2. Renaud SC, Guéguen R, Siest G, Salamon R. Wine, beer, and mortality in middle-aged men from eastern France. Arch Intern Med. 1999;159(16):1865-70. doi:10.1001/archinte.159.16.1865. [ Links ]
3. Keil U, Chambless LE, Döring A, Filipiak B, Stieber J. The relation of alcohol intake to coronary heart disease and all-cause mortality in a beer-drinking population. Epidemiology. 1997;8(2):150-6. doi:10.1001/jama.282.3.239. [ Links ]
4. Stampfer MJ, Colditz GA, Willett WC, Speizer FE, Hennekens CH. A prospective study of moderate alcohol consumption and the risk of coronary disease and stroke in women. N Engl J Med. 1988;319(5):267-73. doi: 10.1056/NEJM198808043190503. [ Links ]
5. Gaziano JM, Buring JE, Breslow JL, Goldhaber SZ, Rosner B, VanDenburgh M, et al. Moderate alcohol intake, increased levels of high-density lipoprotein and its subfractions, and decreased risk of myocardial infarction. N Engl J Med. 1993;329(25):1829-34. doi: 10.1056/NEJM199312163292501. [ Links ]
6. Suh I, Shaten BJ, Cutler JA, Kuller LH. Alcohol use and mortality from coronary heart disease: the role of high-density lipoprotein cholesterol. The Multiple Risk Factor Intervention Trial Research Group. Ann Intern Med. 1992;116(11):881-7. doi: 10.7326/0003-4819-116-11-881. [ Links ]
7. Srivastava LM, Vasisht S, Agarwal DP, Goedde HW. Relation between alcohol intake, lipoproteins and coronary heart disease: the interest continues. Alcohol Alcohol. 1994;29(1):11-24. doi.org/10.1093/oxfordjournals.alcalc.a045479. [ Links ]
8. Savolainen MJ, Kesäniemi YA. Effects of alcohol on lipoproteins in relation to coronary heart disease. Curr Opin Lipidol. 1995;6(4):243-50. PMID: 17326330. [ Links ]
9. Patsch W, Sharrett AR, Sorlie PD, Davis CE, Brown SA. The relation of high density lipoprotein cholesterol and its subfractions to apolipoprotein A-I and fasting triglycerides: the role of environmental factors. The Atherosclerosis Risk in Communities (ARIC) Study. Am J Epidemiol. 1992;136(5):546-57. doi: 10.1093/oxfordjournals.aje.a116532. [ Links ]
10. Rimm EB, Williams P, Fosher K, Criqui M, Stampfer MJ. Moderate alcohol intake and lower risk of coronary heart disease: meta-analysis of effects on lipids and haemostatic factors. BMJ. 1999;319(7224):1523-8. doi: https://doi.org/10.1136/bmj.319.7224.1523. [ Links ]
11. Parker DR, McPhillips JB, Derby CA, Gans KM, Lasater TM, Carleton RA. High-density-lipoprotein cholesterol and types of alcoholic beverages consumed among men and women. Am J Public Health. 1996;86(7):1022-7. doi: 10.2105/AJPH.86.7.1022. [ Links ]
12. Ruidavets JB, Ducimetière P, Arveiler D, Amouyel P, Bingham A, Wagner A, et al. Types of alcoholic beverages and blood lipids in a French population. J Epidemiol Commun Health. 2002;56(1):24-8. doi: 10.1136/jech.56.1.24. [ Links ]
13. Wannamethee SG, Shaper AG. Type of alcoholic drink and risk of major coronary heart disease events and all-cause mortality. Am J Public Health. 1999;89(5):685-90. doi: 10.2105/AJPH.89.5.685. doi:10.1001/archinte.161.11.1413. [ Links ]
14. Criqui MH, Cowan LD, Heiss G, Haskell WL, Laskarzewski PM, Chambless LE. Frequency and clustering of nonlipid coronary risk factors in dyslipoproteinemia. The Lipid Research Clinics Program Prevalence Study. Circulation. 1986;73(1 Pt 2):I40-50. doi:10.1001/archinte.161.11.1413. [ Links ]
15. Weidner G, Connor SL, Chesney MA, Burns JW, Connor WE, Matarazzo JD, et al. Sex differences in high density lipoprotein cholesterol among low-level alcohol consumers. Circulation. 1991;83(1):176-80. doi: 10.1210/jc.2013-1016. [ Links ]
16. Saunders JB, Davis M, Williams R. Do women develop alcoholic liver disease more readily than men? Br Med J (Clin Res Ed). 1981;282(6270):1140-3. doi.org/10.1080/09595238380000201. [ Links ]
17. Frezza M, di Padova C, Pozzato G, Terpin M, Baraona E, Lieber CS. High blood alcohol levels in women. The role of decreased gastric alcohol dehydrogenase activity and first-pass metabolism. N Engl J Med. 1990;322(2):95-9. doi: 10.1056/NEJM199001113220205 [ Links ]
18. Generoso G, Bensenor IM, Santos RD, Santos IS, Goulart AC, Jones SR, et al. Association between high-density lipoprotein subfractions and low-grade inflammation, insulin resistance, and metabolic syndrome components: The ELSA-Brasil study. J Clin Lipidol. 2018. doi: 10.1016/j.jacl.2018.05.003. [ Links ]
19. Santana NMT, Mill JG, Velasquez-Melendez G, Moreira AD, Barreto SM, Viana MC, et al. Consumption of alcohol and blood pressure: Results of the ELSA-Brasil study. PLoS One. 2018;13(1):e0190239. doi: 10.1371/journal.pone.0190239. [ Links ]
20.Cervato AM, Vieira VL. Índices dietéticos na avaliação da qualidade global da dieta. Rev. Nutr. ed. Campinas 2003. doi: 10.1590/S1415-52732003000300012. [ Links ]
21. Brinton EA. Effects of Ethanol Intake on Lipoproteins. Current Atherosclerosis Reports. 2012;14(2):108. doi: 10.1007/s11883-012-0230-7. [ Links ]
22. Perissinotto E, Buja A, Maggi S, Enzi G, Manzato E, Scafato E, Matrangelo G, Frigo AC, Coin A, Crepaldi G, Sergi G. Alcohol consumption and cardiovascular risk factors in older lifelong wine drinkers: the Italian Longitudinal Study on Aging. Nutr Metab Cardiovasc Dis. 2010;20(9);647-55. doi: 10.1016/j.numecd.2009.05.014. [ Links ]
23. Volcik KA, Ballantyne CM, Fuchs FD, Sharrett AR, Boerwinkle E. Relationship of alcohol consumption and type of alcoholic beverage consumed with plasma lipid levels: differences between Whites and African Americans of the ARIC study. Ann Epidemiol. 2008;18(2):101-7. doi: 10.1016/j.annepidem.2007.07.103. [ Links ]
24. Hines LM. Genetic modification of the effect of alcohol consumption on CHD. Proc Nutr Soc. 2004;63(1):73-9. doi: 10.1079/PNS2003321. [ Links ]
25. Zakhari S. Alcohol and the cardiovascular system: molecular mechanisms for beneficial and harmful action. Alcohol Health Res World. 1997;21(1):21-9. doi.org/10.1016/j.jacc.2005.02.075 [ Links ]
26. Camargo CA, Hennekens CH, Gaziano JM, Glynn RJ, Manson JE, Stampfer MJ. Prospective study of moderate alcohol consumption and mortality in US male physicians. Arch Intern Med. 1997;157(1):79-85. doi:10.1001/archinte.1997.00440220083011. [ Links ]
27. Rimm EB, Giovannucci EL, Willett WC, Colditz GA, Ascherio A, Rosner B, et al. Prospective study of alcohol consumption and risk of coronary disease in men. Lancet. 1991;338(8765):464-8. doi: https://doi.org/10.1016/0140-6736(91)90542-W. [ Links ]
28. Arranz S, Chiva-Blanch G, Valderas-Martínez P, Medina-Remón A, Lamuela-Raventós RM, Estruch R. Wine, beer, alcohol and polyphenols on cardiovascular disease and cancer. Nutrients. 2012;4(7):759-81. doi:10.3390/nu4070759. [ Links ]
Received: Apr 1st 2019 Authors' contributions: Ludmila Macêdo Naud participated in the phases of Research conception and design, Data analysis and interpretation, Statistical analysis and Manuscript writing; lsabela Judith Martins Bensenor and Paulo Andrade Lotufo participated in Critical manuscript review for important intellectual content. Corresponding author:
Corresponding author:
Ludmila Macêdo Naud
E-mail: ludmilanaud@gmail.com
Accepted: Jul 30th 2019
All authors approved the final version of the text.
Conflict of interest: The authors have stated that there are no conflicts of interest.
* Paper extracted from doctoral dissertation "Determinação dietética das subfrações lipídicas por ultracentrifugação vertical e ressonância nuclear magnética", presented to, Universidade de São Paulo, Faculdade de Saúde Pública, Departamento de Epidemiologia, São Paulo, SP, Brazil.


{kind=link}
{kind=link}
{kind=link}