










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versión On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.16 no.2 Ribeirão Preto abr./jun. 2020
http://dx.doi.org/10.11606/issn.1806-6976.smad.2020.154623
ORIGINAL ARTICLE
Substance use among adults living on the streets and association with mindfulness
Daniela Prado Rocha Silva ; Marina Monzani da Rocha
; Marina Monzani da Rocha
Universidade Presbiteriana Mackenzie, Centro de Ciências Biológicas e da Saúde, São Paulo, SP, Brazil
ABSTRACT
OBJECTIVE: to analyze the relationship between mindfulness traits and problematic use of alcohol and other drugs.
METHODS: a cross-sectional study was conducted with 40 users of a coexistence service for adults living in the streets or shelters. They answered, during an interview, the MAAS scale (Mindful Attention Awareness Scale), CAGE (Cut down, Annoyde by criticims, Guilty and Eye-opener) and AUDIT (Alcohol Use Disorders Identification Test), as well as a sociodemographic questionnaire.
RESULTS: high prevalence of substance abuse in this sample, and a negative correlation between the problematic use of alcohol and drugs and the level of mindfulness, which may indicate that low levels of mindfulness may be a risk factor for the addicted population.
CONCLUSION: the use of meditation in interventions with this population is suggested.
Descriptors: Alcohol; Drugs; Mindfulness; Homeless Persons.
Introduction
Mindfulness is a Buddhist construct that has been adopted by Western psychology to refer to one's ability to be present in the "here and now", the ability to pay attention at this moment purposefully and without judgment(1). It is a skill that can be developed through mindfulness meditative practices(1). Although there are mindfulness-based intervention protocols aimed at treating substance abuse, such as the Mindfulness-Based Relapse Prevention (MBRP) protocol, a model developed at the Addictive Behaviors Research Center at University of Washington, United States, brought and adapted to Brazil with the help of the protocol's creator, Dr. Sarah Bowen(2), Few studies have investigated, so far, impairments in mindfulness among psychoactive substance users. Given this situation, it is important to investigate the relationship between mindfulness and addictive behaviors.
A US study investigated attention levels in adults referred for treatment due to psychoactive substance use(3). The authors found that users achieved mindfulness scores below the US national average(3). The results were even worse when the mindfulness of multiple drug users who scored even lower than single users was analyzed. These results confirm the hypothesis that there are deficits in drug users' mindfulness, which support the use of strategies to increase this skill during the treatment of substance abuse(3).
In a study with objectives similar to the previous one(3), the mindfulness construct was evaluated in 107 adults seeking substance abuse treatments(4). No differences were found between men and women or between alcohol users and users of other drugs. However, differences in users' mindfulness were found compared to the normative sample of the instrument used to assess the construct, and users achieved lower mindfulness levels compared to non-drug users. The same authors also verified the relationship between mindfulness traits and probable diagnoses of depression and posttraumatic stress in substance users(5). The results indicated that patients with a probable diagnosis of depression or posttraumatic stress reported less mindfulness than patients without these disorders. In particular, it was found that those with comorbidities between the different diagnoses achieved the lowest levels of mindfulness, indicating that low levels of mindfulness may be a risk factor for the development or maintenance of substance use, especially when there are other psychopathologies in comorbidities(5).
Although the studies mentioned indicate that there is a relationship between mindfulness and substance use, this relationship needs to be further explored, especially in at-risk populations. The National Survey on Homeless Population(6) points out that problems with alcoholism and drug addiction are among the main causes for people to live and live on the street (35.5%). The vulnerability of this population and the dependence on alcohol and drugs lead to difficulties in maintaining work activities and fragility in social and family ties, generating a population that deals with poor living conditions and uses the streets as the only option for housing and survival(7). Given this scenario, the objective of this paper is to verify the relationship between addiction and mindfulness in homeless or sheltered adults.
Method
A cross-sectional, quantitative and descriptive study was performed. The project was approved by the Research Ethics Committee of Mackenzie Presbyterian University (Opinion No. 2,541,680). All participants had their dignity and autonomy respected, according to Resolution No. 466 of December 12, 2012, of the National Health Council. Participants had prior access to the Free and Informed Consent Term (FICT), which was signed by them. The risks to participants were minimal, such as possible discomfort in answering questions.
Forty people aged between 20 and 57 years (mean = 38.3 years, standard deviation = 10.6 years) participated in this study, 37 men (92.5%) and three women (7.5%). Participants are users of a homeless adult shelter service. The inclusion criterion was to declare not to be influenced by any psychoactive substance at the time of the research. Regarding race / color, 52.5% self-declared brown; 27.5% white; 17.5%, black and 2.5%, indigenous. Most participants (90%) were single, with only 5% married. With regard to employment, 50% are unemployed, 42.5% have informal employment and another 7.5% have formal employment. In addition, 55.0% reported receiving some government benefit. The educational level of the sample ranged from incomplete elementary school (30%) to higher education (attending, complete or incomplete) (7.5%).
Below is a description of the instruments used.
Sociodemographic Questionnaire: designed to conduct research with indicators such as education, if you are homeless or in a shelter, use tobacco or other drugs, and if you have participated in meditation interventions.
Mindfulness Awareness and Attention Scale (MAAS-BR): assesses the mindfulness factor and consists of 15 items focused on the assessment of mindfulness, using a six-point scale, ranging from one (almost always) to six (almost never)(8). High scores reflect greater capacity for mindfulness(9). The mindfulness construct consists of two factors, awareness and attention, which operationalize the one-factor mindfulness construct(9). The MAAS-BR was adapted with a Brazilian sample (N=395)(10) in a study that corroborated its one-dimensional structure (α = 0.83). In addition to Cronbach's alpha, the authors performed the test-retest (r = 0.80) and split half (0.67) as methods to estimate measurement accuracy.
CAGE (acronym for its four questions in English: Cut down, Annoyed by critics, Guilty and Eye-opener): is an instrument for screening drug abuse or dependence that, through four questions, seeks to detect cases of addiction. of alcohol. Correction is made by assigning one point for each affirmative answer and the score of two points or more indicates a high possibility of alcohol dependence(11).
AUDIT (Alcohol Use Disorders Identification Test): Identifies different levels of alcohol use. Ten multiple choice questions are presented with scores from zero to four points indicating the amount and frequency of alcohol consumption in the last 12 months. After counting points, dependency is classified into one of four axes showing the indicated intervention: Zone I - Primary Prevention (0-7 points); Zone II - Basic Orientation (8-15 points); Zone III - Brief Intervention and Monitoring (16-19 points); Zone IV - Referral to Specialized Service (20-40 points)(12).
All instruments were answered by participants during an individual interview with the researcher. The interview was held in a room of the social service reserved to guarantee the privacy of the participants.
The corrections of the CAGE, AUDIT and MAAS-BR instruments were made according to the instructions of the authors of the validation and standardization studies for the Brazilian population. Descriptive statistical analyzes (mean, standard deviation, percentage, minimum, maximum, etc.) were performed to characterize the sample with regard to substance use and mindfulness. The results of the different instruments were correlated (Pearson Bivariate Correlation) in order to test the association between the variables. In addition, the Mann-Whitney U test was used to compare the means obtained by participants divided into groups according to the number of substances used (non-users x single users x multi-users) and Pearson's chi-square test for the analysis of categorical data. All tests were performed using SPSS 23.0 software. For the inferential statistical analyzes, the significance level p <0.05 was adopted.
Results
Of the 40 participants, 22 (52.5%) reported using tobacco and 19 (47.5%) using alcohol. It is revealed, considering only alcohol and other drugs, that 19 participants were considered non-users (47.5%); eight were single users (20%) and 13 were multi-users (32.5%). Among the poliusuaries, the average of substances used was 2.46 (SD = 0.97).
The CAGE score ranged from zero to four, with a mean of 1.35 (standard deviation = 1.29). In all, 17 (42.5%) participants achieved a score indicating risk of alcohol dependence on CAGE response (more than two positive responses). The result of the level of alcohol use, according to the AUDIT classification, indicated that 35% were in the Primary Prevention stage; 22.5% in Basic Orientation; 7.5% for Brief Intervention + Monitoring and 35% for Referral for Service.
Figure 1 shows the distribution of the results obtained by the participants in the MAAS response. The vertical line indicates the median of the Brazilian sample in the MAAS validation study(10).
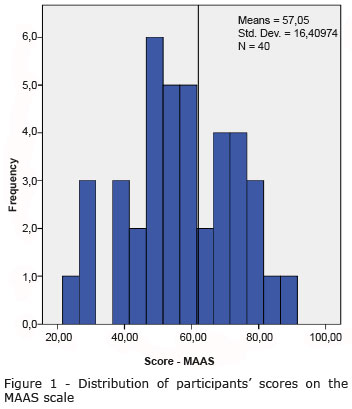
The average score obtained by the participants in the MAAS was 57.07 (SD = 16.41) and the median was 56.5, which is lower than the median of the Brazilian normative sample.
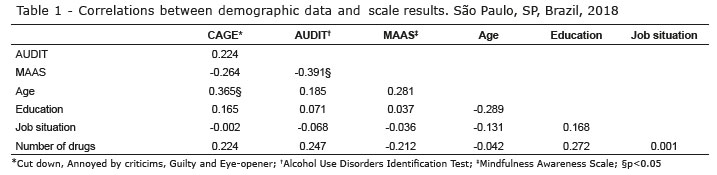
The correlations found between demographic data (age, education, employment status and number of drugs used) and the results obtained by participants in the CAGE, AUDIT and MAAS scales are presented in Table 1.
There was no association between the different variables, except for the moderate negative correlation between MAAS and AUDIT and moderate positive correlation between age and CAGE score, ie: the results show that the higher the alcohol dependence, the lower the attention rates and that the older you are, the greater the likelihood of alcohol dependence.
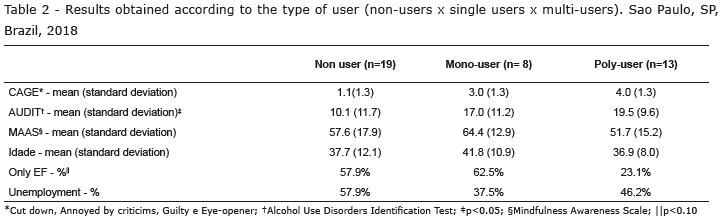
The results obtained at different scales were analyzed according to the type of user (non-users x single users x multi-users). In addition, it was verified if there was a difference between the types of users regarding age, education level and employment status. The results are presented in Table 2.
There was a higher prevalence of people with low levels of education (up to elementary school) among non-users and single users. Only 23.1% of the poliusuaries had completed elementary school, while the others had higher education levels. In addition, single-users and multi-users scored higher on AUDIT compared to non-users.
Finally, the participants were divided into three groups according to the level of mindfulness. For this, the mean and standard deviation obtained in the Brazilian MAAS validation study were used. Those who scored within the mean plus or minus one standard deviation were considered "average" mindfully. Those whose scores were more than one below-average standard deviation were classified as "Low" and those who scored at least one above-average standard deviation had their full attention classified as "High." Table 3 shows the results obtained by the participants of the three groups in CAGE, AUDIT and sociodemographic variables.
The chi-square test showed no significant difference between participants with low, medium and high mindfulness in CAGE scores (p = 0.387), level of education (p = 0.837), and employment status (p = 0.919) and in the type of user (p = 0.547). In AUDIT, a significant difference was found as a function of the level of mindfulness (p = 0.048). Participants who used alcohol with indication for Primary Prevention and Basic Counseling presented, more frequently, medium and high levels of mindfulness, while those who had indication for Brief Intervention and Monitoring, as well as Referral for Specialized Services, presented higher frequency, Low scores on MAAS. In addition, a difference in meditation practice was found in the three groups, and only 16.7% of those who reported having contact with meditation had a low MAAS score.
Discussion
To meet the goal of studying the full relationship and substance use in a population with a high level of social vulnerability, 40 homeless adults were interviewed. Of these, 14 (35%) indicated behaviors compatible with probable risk of dependence, according to the results of alcohol use level according to the AUDIT classification. In the evaluation with CAGE, 17 (42.5%) reached the risk range of dependencies and, in this sense, it is understood that the results of this study confirm the demand, already highlighted in other studies(7), for care due to substance use for the homeless population. Due to the degree of vulnerability to which these subjects are subjected, there are, in the usual practice of health services, demands for recurrent physical and mental health care as a result of abstinence from the use of psychoactive substances(7). Another issue addressed by the authors is access to health services, which becomes a challenge in the care of this population, since often the homeless person does not access such services or poor access(7).
The participants of this study were separated into non-users, single users and multi-users as in another study(3). The difference between AUDIT results, depending on the type of user found in this study, may indicate that problematic alcohol use is related to illicit drug use. One study establishes alcohol as a "gateway" to other drugs, which contrasts with the common sense that marijuana is responsible for driving a person to use multiple drugs(13). Thus, the need for public policies focused on the abuse of alcohol is emphasized, especially among those who live on the streets.
In addition, there was a higher prevalence of people with low levels of education (up to elementary school) among non-users and single users. In addition, single-users and multi-users had higher AUDIT scores compared to non-users. There is a tendency for higher use of multiple drugs by people with higher education, unlike studies found(14), because years of schooling were negatively correlated with illicit drug use(14). However, educational level was positively correlated with intelligence quotient (IQ) and negatively correlated with impulsivity, two characteristics that are also correlated with drug use and were not assessed in the study participants. Thus, the negative correlation between education and drug use(14) It may reflect issues that are correlated with education and not education itself. In Brazil, university students are known to have more frequent and intense drug use than other portions of the population(15). This data may explain the result found in this paper.
As expected, based on the results obtained in previous studies(3-5), a large part of the study sample, achieved below average attention scores in the MAAS, using as a parameter the data from the Brazilian validation of the instrument(10). In addition, the results indicated that participants who had experiences with meditation obtained higher scores on the scale, which reinforces the validity of the instrument.
Regarding the relationship between substance use and the mindfuness construct, the results indicated a negative correlation between AUDIT and MAAS, which corroborates the hypothesis that the more the substance abuser (in this case, alcohol), the lower your level of mindfulness. Other cross-sectional baseline studies that used MAAS as an instrument to assess mindfulness traits and correlate with drug use also yielded the same results(3-4). Samples with alcohol and other drug use disorders score lower than expected for the general population on scales that measure mindfulness(3-4), except for opioid users(5). These results suggest that mindfulness deficits may be common in the drug abuse or addiction population. Higher levels of mindfulness may be a protective factor against drug use, as being focused at this time would help you cope with emotions as they are without having to flee to alcohol or other drugs, and more quickly identify triggers prior to use. They also indicate that mindfulness deficits may be common in individuals seeking treatment for psychoactive substance use, leading to the hypothesis that such deficits lead to increased subject vulnerability, may represent a risk factor for the development or maintenance of substance use disorders. Longitudinal studies should be performed in the future to verify this hypothetical causal relationship.
Studies have shown that Acceptance and Commitment Therapy (ACT), compared with other usual opioid addiction treatments (methadone use and the Alcoholics Anonymous twelve-step program), had a greater decrease in drug use compared to two other treatments at six-month follow-up(16). There are positive results data on the effectiveness of Dialectical Behavioral Therapy (DBT) in drug-dependent patients with Bordeline Personality Disorders, as most studies have found better abstinence rates, lower use of psychoactive substances and advances in emotional regulation in subjects who adhered to this treatment modality(17). Both ACT and DBT include mindfulness-based interventions. Thus, it is understood that contextual behavioral therapies, which adopt principles of mindfulness in their interventions(16-17), have a positive impact on reducing addictive behaviors, but as such therapies involve other interventions, it can be hypothesized that other variables are related to decreased use, such as the relationship between therapist and patient.
To date, the only specific attention protocol for substance use disorders, MBRP, has been established for outpatient treatment of substance use(18). The MBRP protocol, compared with the usual treatments (twelve-step program and psychoeducation), and the Relapse Prevention Treatment (RP). Participants assigned to MBRP and RP reported a significantly lower risk of substance use relapse and alcohol abuse, and among those who used substances significantly fewer days of substance use and heavy drinking in the six months of follow-up. Cognitive behavioral RP showed an advantage over MBRP in time to first drug use. At the 12-month follow-up, MBRP participants reported significantly fewer days of substance use and significantly decreased heavy consumption compared to RP and usual treatment. Targeted mindfulness practices can support long-term results as they strengthen the ability to skillfully monitor and cope with the discomfort associated with negative desire or affect(18).
Thus, it is understood that interventions using meditation and mindfulness techniques are promising to be used in addition to usual drug treatments, as such studies indicate that contextual therapy interventions have shown effectiveness and longitudinal outcomes for such disorders(16-17). Mindfulness exercises can also provide a rewarding and relaxing alternative to drug use(3) and, in fact, mindfulness-based interventions are believed to help reduce the risk of relapse(18).
This study has some limitations, such as the small number of participants, the sample being predominantly male and homeless or sheltered, the choice of a single unifactor instrument to measure mindfulness and the cross-sectional design of the study, which limits the determination of causality between the variables. Thus, it is understood that a future study using more sophisticated and broader mindfulness measures to determine whether different facets of mindfulness are more strongly associated with the constructs examined, and a larger and larger sample could help to further examine the association of various factors with impairment in mindfulness and other aspects of mindfulness. In addition, longitudinal studies could answer causality questions among the variables.
Conclusion
Despite the limitations presented, the findings of this study suggest that there is impairment in mindfulness in substance-using and homeless adults, which suggests that this population may benefit from intervention that includes training in mindfulness techniques.
References
1. Ludwig DS, Kabat-Zinn J. Mindfulness in Medicine. JAMA. 2008;300(11):1350-2. doi: 10.1001/jama.300.11.1350 [ Links ]
2. Weiss I, Noto AR. Tratamentos em grupo baseados em mindfulness. In: Neufeld CB, Rangé BP, organizadores. Terapia cognitivo-comportamental em grupos: das evidências à prática. Porto Alegre: Artmed; 2017. p. 238-e300. [ Links ]
3. Dakwar E, Mariani JP, Levin FR. Mindfulness impairments in individuals seeking treatment for substance use disorders. Am J Drug Alcohol Abuse. 2011;37:165-9. doi: 10.3109/00952990.2011.553978. [ Links ]
4. Shorey RC, Brasfield H, Anderson S, Stuart GL. Mindfulness deficits in a sample of substance abuse treatment seeking adults: a descriptive investigation. J Subst Use. 2013;19(1-2):194-8. doi: 10.3109/14659891.2013.770570 [ Links ]
5. Shorey RC, Brasfield H, Anderson S, Stuart GL. Differences in trait mindfulness across mental health symptoms among adults in substance use treatment. Subst Use Misuse. 2014;49(5):595-600. doi: 10.3109/10826084.2014.850310. [ Links ]
6. Ministério do Desenvolvimento Social e Combate à Fome (BR). Meta Instituto de Pesquisa de opinião. Pesquisa Nacional sobre a População em situação de rua; 2008. Disponível em: https://fpabramo.org.br/acervosocial/estante/pesquisa-nacional-sobre-populacao-em-situacao-de-rua/. [ Links ]
7. Mendes CRP, FillipeHorr J. Vivência nas ruas, dependência de drogas e projeto de vida: um relato de experiência no CAPS-ad. Rev Psicol Saúde. [Internet]. 2014 Jun; 6(1):90-7. Disponível em: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S2177-093X2014000100012&lng=pt. [ Links ]
8. Brown KW, Ryan RM. The benefits of being present: Mindfulness and its role in psychological well-being. J Personal Soc Psychol. 2003; 84(4):822-48. doi: 10.1037/0022-3514.84.4.822 [ Links ]
9. Pires JG, Nunes MFO, Demarzo MMP, Nunes CHSS. Instrumentos para avaliar o construto mindfulness: uma revisão. Aval Psicol. [Internet]. 2015 Dez; 14(3):329-38. Disponível em: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1677-04712015000300005&lng=pt. [ Links ]
10. Barros VV, Kozasa EH, Souza ICW, Ronzani TM. Evidences of validity of the Brazilian version of the Mindful Attention Awareness Scale (MAAS). Psicol Reflexão Crítica. 2015;28(1):87-95. doi: 10.1590/1678-7153.201528110. [ Links ]
11. Masur J, Monteiro M. Validation of the CAGE alcoholism screening test in Brazilian Psychiatry inpatient hospital setting. J Biol Res. 1983 Oct;16(3):215-8. PMID: 6652293. [ Links ]
12. Lima CT, Freire ACC, Silva APB, Teixeira RM, Farrell M, Prince M. Concurrent and construct validity of the AUDIT in an urban Brazilian sample. Alcohol Alcoholism. 2005;40:584-9. doi: 10.1093/alcalc/agh202. [ Links ]
13. Barry AE, King J, Sears C, Harville C, Bondoc I, Joseph K. Prioritizing alcohol prevention: Establishing alcohol as the gateway drug and linking age of first drink with illicit drug use. J School Health. 2016;86:31-8. doi: 10.1111/josh.12351. [ Links ]
14. Heyman G, Dunn BJ, Mignone J. Disentangling the correlates of drug use in a clinic and community sample: a regression analysis of the associations between drug use, years-of-school, impulsivity, IQ, working memory, and psychiatric symptoms. Front Psychiatry. 2014; 5: 70. doi: 10.3389/fpsyt.2014.00070. [ Links ]
15. Ministério da Saúde. Secretaria Nacional de Políticas sobre Drogas (BR). I Levantamento Nacional sobre o Uso de Álcool, Tabaco e Outras Drogas entre Universitários das 27 Capitais Brasileiras. Brasília: SENAD; 2010. Disponível em: http://www.grea.org.br/userfiles/GREA-ILevantamentoNacionalUniversitarios.pdf [ Links ]
16. Hayes SC, Wilson KG, Gifford EV, Bissett R, Piasecki M, Batten SV, et al. A preliminary trial of twelve-step facilitation and Acceptance and Commitment Therapy with polysubstance-abusing methadone-maintained opiate addicts. Behav Therapy. 2004;35:667-88. doi: 10.1016/S0005-7894(04)80014-5. [ Links ]
17. Oppermann CMO, Lewgoy LB, Araújo RB. Terapia comportamental dialética para dependentes químicos. Ver Bras Ter Cogn. 2015; 11(2):113-8. doi: 10.5935/1808-5687.20150016. [ Links ]
18. Bowen S, Witkiewitz K, Clifasefi SL, Grow J, Chawla N, Hsu SH, et al. Relative Efficacy of Mindfulness-Based Relapse Prevention, Standard Relapse Prevention, and Treatment as Usual for Substance Use Disorders: A Randomized Clinical Trial. JAMA Psychiatry. 2014;71(5):547-56. doi: 10.1001/jamapsychiatry.2013.4546. [ Links ]
Received: Feb 11th 2019 Author's contributions: Study design and planning: Daniela Prado Rocha Silva, Marina Monzani Da Rocha. Data collection: Daniela Prado Rocha Silva. Data analysis and interpretation: Daniela Prado Rocha Silva, Marina Monzani Da Rocha. Writing of the manuscript: Daniela Prado Rocha Silva, Marina Monzani Da Rocha. Critical revision of the manuscript: Daniela Prado Rocha Silva, Marina Monzani Da Rocha. Corresponding Author:
Corresponding Author:
Marina Monzani da Rocha
E-mail: marinamonzani@gmail.com
Accepted: Aug 27th 2019
All authors approved the final version of the manuscript.
Conflict of interest: The authors declare no conflict of interest.


{kind=link}
{kind=link}
{kind=link}