










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.16 no.3 Ribeirão Preto jul./set. 2020
http://dx.doi.org/10.11606/issn.1806-6976.smad.2020.165513
ORIGINAL ARTICLE
Effects of the Mindfulness-Based Cognitive Therapy Program on stress, self-efficacy and mindfulness in university students*
Mariana Ladeira de Azevedo ; Carolina Baptista Menezes
; Carolina Baptista Menezes
Universidade Federal de Santa Catarina, Florianópolis, SC, Brazil
ABSTRACT
OBJECTIVE: to verify the effects of Mindfulness-Based Cognitive Therapy program on stress, self-efficacy, and dispositional mindfulness as outcomes in a sample of undergraduate students.
METHOD: quasi-experimental longitudinal study in a sample of 13 students. The variables perceived stress, perceived general self-efficacy and dispositional mindfulness were analyzed, measured by self-report instruments answered by the participants before the first session and at the end of the eighth session of the intervention. The intervention lasted eight weeks.
RESULTS: comparing scores at the beginning and at the end of the program, perceived stress reduced and there was an increase in general perceived self-efficacy and mindfulness. Correlations between outcomes indicated that older age is related to greater general self-efficacy and mindfulness; stress reduction is related to increased general self-efficacy and mindfulness; and increased self-efficacy is related to increased mindfulness.
CONCLUSION: data indicate that Mindfulness-Based Cognitive Therapy can help develop mindfulness skills, reduce perceived stress and increase general perceived self-efficacy, possibly contributing to coping with challenging situations in the academic context, during college, and in future professional practice.
Descriptors: Mindfulness; Cognitive Behavioral Therapy; Student Health Services; Stress, Psychological; Self Efficacy.
Introduction
In the scientific context, mindfulness is a term widely used to designate both a mental quality - personality characteristics (trait), skill set or psychological status - and the practices themselves, in the form of isolated techniques or intervention programs(1). Referred to as mental quality, it is called dispositional mindfulness.
One of the most used definitions for the mindfulness construct is the awareness that emerges when paying attention to the internal or external experience that occurs in the present moment, deliberately and without judgment(2). There is no consensus on the operational definition of mindfulness, and it can be considered as a unidimensional or multidimensional construct(1, 3-4). For this study, we used the multidimensional concept of mindfulness composed of five factors(5): a) observing, referring to noticing internal and external experiences, such as cognitions, emotions, physical sensations, sight, sounds, tastes and smells; b) describing, referring to naming the characteristics of the internal experiences; c) acting consciously, referring to being attentive to the activities of the moment, being the opposite of what is called automatic pilot, a mechanical behavior while attention is focused on something else; d) non-judgment of the internal experience, referring to adopting a non-evaluative and non-judgmental posture in relation to thoughts and feelings; and e) non-reactivity to the internal experience, referring to allowing thoughts and feelings to come and go, not allowing oneself to be affected or taken by them.
The term has gained visibility since the emergence of the manual brief intervention protocols - involving the practice of mindfulness - called Mindfulness-Based Programs (MBPs). The systematization, application and validation of the MBPs started with the first program, Mindfulness-Based Stress Reduction (MBSR), developed in the 1970s and used with people in a hospital context at the University of Massachusetts, USA(6-7). From it, other programs were created, such as the Mindfulness-Based Cognitive Therapy (MBCT), which adds cognitive and psychoeducational principles and techniques, based on Cognitive Therapy, to the original MBSR program(8). The MBCT is mainly used to prevent relapse in depression, but it has also shown effective results on other psychological aspects, such as anxiety and well-being(9-11).
Considering the high prevalence of anxiety, stress and depression among university students, interventions to assist in the management and prevention of these conditions have emerged in the university context(12-15). Among these, the MBPs for the university population have gained space, indicating favorable results on stress, anxiety and depression when compared to the control group(16-18).
There is no standardization regarding the application of MBPs in the university context, and the programs vary in terms of duration (for example: from 5 to 8 weeks) or suffer adaptations from the original curricula based on which most studies for validation (randomized controlled clinical trials) are conducted, hindering the comparison between the intervention criteria. In addition, some studies lack clarification on the qualification and professional training of those who provide the interventions. Therefore, there are limitations in conducting systematic reviews of these interventions in the university context for undergraduate students in general(1).
In Brazil, the diffusion of the mindfulness protocols is at an early stage. The National Policy for Integrative and Complementary Practices in Health (Política Nacional de Práticas Integrativas e Complementares em Saúde, PNPIC)(19) is the regulatory point for incorporating programs like these in Brazil. In other countries, such as the United Kingdom, mindfulness programs like the MBCT are reference therapeutic practices based on evidence in the national health systems(20-21).
There are few studies on mindfulness-based interventions in Brazil(22-23). A study on the MBCT in a clinical population verified the understanding and applicability of this program in the Brazilian population, being considered understandable and acceptable(24). Although there are no specific studies on the MBCT in the university population in the country, it would be possible to hypothesize that the benefits of these programs could also extend to undergraduate students.
As justifications for this study, offering MBPs to undergraduate students could be a way of providing techniques and opportunities for the development of skills that allow them to deal with the stress of academic life, acting preventively in mental health and promoting quality of life and well-being. Thus, this pilot study aimed to verify the effects of participation in the Mindfulness-Based Cognitive Therapy Program on stress, self-efficacy, and dispositional mindfulness in undergraduate students. Based on this pilot, it was possible to consider the feasibility of carrying out future controlled studies with the MBCT in the university population.
Method
This quasi-experimental and longitudinal pilot study compared the scores of perceived stress, perceived general self-efficacy, and dispositional mindfulness before and after participation in the intervention. The sample consisted of undergraduate students from a federal university, recruited from the participants of an introductory lecture on mindfulness, open to the academic community without course restrictions, featuring convenience sampling. The inclusion criteria were age between 18 and 65 years old, having active enrollment in the university, and having participated in the introductory lecture to the program. The exclusion criteria were declaring to have previously completed another undergraduate course, making use of medication whose dosage has not been stabilized for a minimum of three months, making use of medication without medical supervision, declaring some mental disorder without undergoing psychotherapeutic monitoring, declaring prior diagnosis of personality disorders, schizophrenia and psychotic disorders, declaring to be in active substance abuse, being absent in the first session of the program, and being absent in two or more sessions of the program. These criteria followed the guidelines of the MBCT program curriculum and other research studies on MBPs with clinical and non-clinical samples(8, 25-26).
Initially, the participants attended the introductory lecture that addressed concepts, fundamentals and research results with mindfulness-based interventions, detailing the MBCT program and the conditions for participation. The lecture was published on electronic forums and e-mail lists of undergraduate courses and enrollments were made online. The place where the lecture was held had a capacity for 60 people, with 43 students attending. At the end of the lecture, 31 students interested in participating in the program signed a clinical evaluation questionnaire and the Free and Informed Consent Form (FICF). As there were more interested individuals than places available for the program, after the pre-screening using the clinical evaluation questionnaire according to the inclusion and exclusion criteria, a simple random selection was carried out by means of a draw to select 15 students. As it is a pilot study, no sample calculation was performed and the sample size was defined in view of the physical capacity of the group room of the Psychology school-clinic where the program was carried out. The interested students who were not selected received feedback by e-mail informing them of the result of the selection and offering them priority to participate in the next edition of a mindfulness-based program.
Subsequently, the pre-screened participants were contacted to schedule the screening interview. A digital leaflet containing complementary guidance on participation in the program was also sent to the participants' e-mail and it was requested to be read in advance of the interview. The individual interviews with the participants took place one week before the beginning of the intervention and followed the screening script adapted from the MBCT program(8). The interview addressed questions about the participant's health history, treatments, and medical and psychotherapeutic monitoring, in addition to the items that are part of the inclusion and exclusion criteria. It was also an opportunity to answer questions, provide additional information about the survey or the MBCT, and confirm participation in the program.
Fifteen students confirmed their participation and started the program according to the screening criteria. The participants were from the areas of Engineering, Arts, and Human Sciences. On the same day before starting the first session and immediately at the end of the eighth session, the participants filled out the printed instruments to measure perceived stress, perceived general self-efficacy, and mindfulness. Thirteen participants concluded their participation in the program, constituting the total sample of this study for a per-protocol analysis.
In order to measure the perceived stress, general perceived self-efficacy, and dispositional mindfulness outcomes, the following self-reporting instruments adapted and validated in Brazil were used: Perceived Stress Scale (PSS, α = 0.82))(27-28), containing 14 items and a total score ranging from zero to 56, indicating the lowest and highest level of perception of situations as stressful; Five Facets of Mindfulness Questionnaire (FFMQ-BR, α = 0.81)(5, 29) composed of 39 items with a final score ranging from 39 to 195 points, indicating the lowest and highest level of mindfulness; and Perceived General Self-Efficacy Scale (PGSES, α = 0.85)(30-33), containing 10 statements in which the total score ranges from 10 to 40 points where the higher the score, the greater the respondent's capacity in terms of organizing and carrying out activities.
The Mindfulness-Based Cognitive Therapy (MBCT)(8) program, with evidence of efficacy recorded in research and clinical trial reports(11), was taught in groups in the first semester of 2019, totaling eight meetings (one per week) lasting 2.5 hours each. The intervention was carried out on the university's psychological care clinic, in a specific room for group activities. The teaching methodology of the program was experiential and strictly followed the MBCT curriculum, where information on long formal practices, brief informal practices, and psychoeducational content can be accessed. The participants received a handout with complementary content and audios in mp3 format each week to carry out the practices between sessions.
The study was conducted in accordance with Resolution No. 466, of December 12th, 2012, of the National Health Council and was approved by the Ethics Committee in Research with Human Beings (Comitê de Ética em Pesquisa com Seres Humanos, CEPSH), of the Federal University of Santa Catarina (opinion No. 3, 499, 336). The program was applied voluntarily by a professional with 20 years of experience in contemplative practices (Buddhism and oriental arts, such as yoga and tai chi chuan), graduation in Psychology, post-graduation in cognitive-behavioral psychotherapy, training in mindfulness-based programs, including Mindfulness-Based Cognitive Therapy by the Oxford Mindfulness Centre (OMC), and met the ethical requirements of the professional practice in Psychology in Brazil(34) and international guidelines for teaching mindfulness-based programs (35), under professional supervision of a British professor linked to the OMC while conducting the program. The MBCT was carried out on the Psychology school-clinic of a public university in the state of Santa Catarina.
The data were analyzed using the Stata software, version 14.0. Descriptive statistics of absolute frequency and proportions were used to characterize the sample and participation in the program. The Wilcoxon's test for dependent samples was used to compare the scores of the pre- and post- intervention scales, Spearman's correlation to verify the association of the difference between the pre- and post- scores with the sample characteristics, and Pearson's partial correlation to control variables and investigate their influences on the outcomes. For all the inferential analyses, a significance level of p < 0.05 was adopted.
Results
The participants were students aged between 19 and 30 years old (M = 22.5; SD = 3.1), seven (53.9%) were female and six (46.1%) were male. Their presence in the sessions ranged from 6 to 8 sessions (M = 7.9; SD = 0.65) and the mean frequency of practice between sessions ranged from 1 to 6 days a week (M = 3.5; SD = 1.5). As for the mean duration of the daily practices, one (7.7%) participant practiced only during the face-to-face sessions. Among those who performed the practice on more days of the week, three (23.1%) practiced less than 10 minutes, three (23.1%) between 10 and 19 minutes, one (7.7%) between 20 and 29 minutes, and five (38.4%) between 30 and 39 minutes.
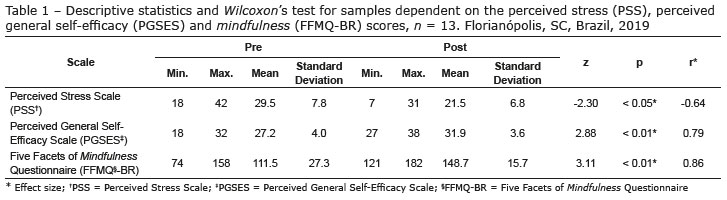
With statistical significance and moderate effect size, the results indicated that the perceived stress level decreased (PSS: z = -2.30; p < 0.05; r = -0.64), and that the levels of perceived general self-efficacy and mindfulness increased (PGSES: z = 2.88; p < 0.01; r = 0.79; FFMQ-BR: z = 3.11; p < 0.01; r = 0.86) in the comparison between scores at the end and beginning of the program (Table 1).
The Spearman's correlation test was performed between age, number of sessions, mean frequency of weekly practice between sessions, and the scores of the instruments answered after the MBCT program. There was a moderate correlation between the PSS and FFMQ-BR scores (rs = -0.59; p < 0.05); that is, the lower the perceived stress, the higher the mindfulness indexes. No relation was verified between age, number of sessions attended, and mean frequency of practice and the PSS, PGSES and FFMQ-BR scores.
The change index of the three instruments, namely, PSS, PGSES and FFMQ-BR, was calculated through the differences between the post- and pre-program scores for each participant, verifying if there was an increase or reduction in the outcomes as a result of the intervention. With these data, the Spearman's correlation test was performed to verify if there was a relation between the changes in the outcomes resulting from the MBCT program. There was a significant positive correlation with age and change in PGSES (rs = 0.63; p < 0.05) and in FFMQ-BR (rs = 0.58; p < 0.05), that is, the greater the age, the higher the index of general perceived self-efficacy and mindfulness. There was a negative correlation of PSS with PGSES (rs = -0.96; p < 0.01) and FFMQ-BR (rs = -0.84; p < 0.01), indicating that the reduction in perceived stress is related to increased perceived self-efficacy and increased mindfulness. Additionally, the positive correlation between the PGSES and FFMQ-BR variables (rs = 0.82; p < 0.01) suggests that the higher the self-efficacy index, the higher the mindfulness index (Table 2).
To deepen the understanding of the relations verified in Table 2, the effects of the PSS, PGSES and FFMQ-BR variables were controlled using Pearson's partial correlation test. The FFMQ-BR index maintained a significant and moderate correlation with the PSS index when the PGSES index was isolated (r = -0.63; p < 0.05). In turn, the PSS index maintained a significant and moderate correlation with the PGSES index (r = -0.64; p < 0.05) when the FFMQ-BR index was controlled. However, the relation between the FFMQ-BR index and the PGSES index becomes weak and not significant when the PSS index is controlled (r = 0.07; p = 0.83). Therefore, the reduction in stress correlated with the increase in mindfulness (controlling the effect of general self-efficacy) and the reduction in stress correlated with the increase in general self-efficacy (controlling the effect of mindfulness). However, mindfulness and general self-efficacy did not correlate when controlling the stress variable. Thus, even in a preliminary manner, it can be hypothesized that the effect of the intervention on the variables of mindfulness and self-efficacy may be moderated by the stress reduction.
Discussion
This study aimed to verify the effects of participation in the Mindfulness-Based Cognitive Therapy Program on stress, self-efficacy, and dispositional mindfulness in undergraduate students, comparing scores of measurement instruments before and after the intervention. The reduction in perceived stress and the increase in general perceived self-efficacy and mindfulness after the intervention indicated that the MBCT program benefited these outcomes. This finding was also verified in other studies that taught MBPs to students in the health area and that used, among psychometric measures related to mental health, cognition and/or attention, the PSS, PGSES and FFMQ instruments(16, 36).
The correlation between the change indexes (difference between post- and pre-scores) of PSS, PGSES and FFMQ-BR reinforces that the effects on perceived stress, perceived general efficacy, and mindfulness would be due to participation in the MBCT. The data from this study also indicated a significant correlation between the reduction of perceived stress and the increase in mindfulness. The negative and significant correlation between perceived stress (PSS) and dispositional mindfulness measured through the FFMQ was also verified in university students in the United States(37), pointing out that the increase in dispositional mindfulness requires a continuous practice that can be learned through mindfulness-based interventions. In addition, one of the mechanisms involved in the learning process of mindfulness skills is cognitive reevaluation, in which the perception of stressful situations is modified, and it is verified that the practice of mindfulness leads to an increase in positive evaluation, consequently acting on the stress levels(38). The significant relation between reduction in perceived stress and increase in perceived general self-efficacy, verified in the results of this study, suggests that the stress reduction is related to the perception or acquisition of more personal resources and coping strategies to deal with challenging and stressful contexts(39-40).
The results also indicated that there was no significant relation between the level of participation in the sessions and the outcomes. This finding is consistent with other studies that used mindfulness-based interventions which lasted between four and eight weeks and also had effective results, although the amount of practice did not moderate the effect(16, 36). Similarly, another study comparing control groups, of four-week and eight-week mindfulness-based interventions, indicated that there was no significant difference in the main outcomes, including mindfulness, when the four- and eight-week groups were compared; but both showed differences when compared to the control group(41).
The frequency of daily practice also did not present a significant correlation with the outcomes, which is consistent with another study that indicated the absence of correlation between the frequency and duration of the daily practice of mindfulness with psychological measures of stress, trait and state anxiety, mindfulness, psychological well-being, and satisfaction with life(42). One hypothesis is that the amount of practice can become a significant moderator of the impact on the outcomes when evaluating a longer time of practice, as shown by other studies(43).
Although there is no standardization in the format of the MBPs taught in the university context, the results seem promising, indicating a potential for the inclusion of such programs as part of the academic curriculum or their offer as interventions and complementary courses for students. A survey on the offer of mindfulness-related activities at medical schools in the United States indicated that 79% (111 of 140) provided some kind of mindfulness-related activity. More specifically, 87 (62%) offered mindfulness activities for well-being, 47 (34%) offered clinical mindfulness activities, and 43 (30%) included mindfulness in the curriculum. Of the academic mindfulness centers associated with medical schools (33; 24%) the most used MBPs were Mindfulness-Based Stress Reduction (MBSR) (22 of 33; 67%); Mindful Movement (MMOV) (13 of 33; 39%); and Mindfulness-Based Cognitive Therapy (MBCT) (13 of 33; 39%), indicating that Medicine has become receptive to mindfulness, at least as a voluntary way of learning and practicing self-care(44).
Although this study did not comprise a complete experiment, and although there is not a large enough sample to perform analyses of a moderating effect, the partial correlations (based on the changes indexes of the scores) suggest that the reduction in perceived stress was correlated with the increase in general perceived self-efficacy and mindfulness, even when controlling each of these variables. At the same time, the increase in mindfulness and in perceived general self-efficacy no longer have a significant correlation when the reduction in perceived stress was controlled.
These data are preliminary and should be interpreted with caution, in view of the limitations of a design without a control group and of a partial correlation analysis. Nevertheless, they could indicate the hypothesis that the effect of the intervention in increasing mindfulness and overall self-efficacy may be moderated by stress reduction, differing from findings that most often take mindfulness as a moderator of the relation between stress, or other factors, on outcomes related to health(45-48). Another alternative explanation for the results of partial correlations could be a mediation relation, in which increasing mindfulness helps to reduce stress, and reducing stress helps to increase self-efficacy. These relations cannot be interpreted conclusively with the present design and with the sample size, and should be considered as hypotheses to be verified by future studies with complete experimental designs and with a sample that allows testing these premises.
This study has limitations regarding the sample due to its size, selection criteria, and absence of a control group. However, it is considered that the character of a pilot study fulfilled the objective of preliminarily verifying the feasibility of conducting similar studies in the university context, enabling the realization of future controlled and randomized clinical trials.
Additionally, it was decided to use a general perceived self-efficacy scale instead of a specific self-efficacy scale for higher education. However, the study had no emphasis on the effects of stress or self-efficacy on academic tasks and/or performance specifically, but on the perception about the ability to deal with stress in general, expanding to different areas of life, and the qualitative reports at the end of the program confirmed this intention. Future Brazilian studies with a university population may use specific self-efficacy for higher education as a complement, even comparing the effects of MBPs on academic performance through achievement and frequency rates.
Finally, to date, there are no studies published using MBCT in academic populations in Brazil, making it difficult to compare the findings with other regional results. Therefore, it is expected that this pilot study will be a starting point for carrying out other research studies using this type of intervention in the university context.
Conclusion
Participation in the Mindfulness-Based Cognitive Therapy program had beneficial effects on perceived stress, perceived general self-efficacy, and dispositional mindfulness, reinforcing the relation between stress and general self-efficacy in university students. Since it is not possible to confirm the moderating effects of the practice of mindfulness through the present design, future studies should consider different explanatory models involving the dispositional mindfulness, perceived stress, and/or perceived general self-efficacy variables.
It was considered feasible to carry out the MBCT program in the university context with the support of infrastructure from the higher education institution and having trained and qualified facilitators, following the international recommendations for teaching mindfulness-based programs. It is suggested that the development of skills acquired in MBPs can contribute to the management of stressful situations arising both from the academic context and training and from future professional performance. Although this is a pilot study, the results provide favorable preliminary evidence for expanding the offer of mindfulness-based programs, taught by trained professionals to the academic population and in the context of Brazilian universities.
References
1. Van Dam NT, van Vugt MK, Vago DR, Schmalzl L, Saron CD, Olendzki A, et al. Mind the hype: a critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspect Psychol Sci. [Internet]. 2018 Jan [cited 2019 Nov 26];13(1):36-61. Available from: <http://journals.sagepub.com/doi/10.1177/1745691617709589> [ Links ]
2. Williams JM, Teasdale JD, Segal ZV, Kabat-Zinn J, editors. The mindful way through depression: freeing yourself from chronic unhappiness. New York (NY): Guilford Press; 2007. 273 p. [ Links ]
3. Tomlinson ER, Yousaf O, Vittersø AD, Jones L. Dispositional mindfulness and psychological health: a systematic review. Mindfulness. [Internet]. 2018 Feb [cited 2018 May 20];9(1):23-43. Available from: <http://link.springer.com/10.1007/s12671-017-0762-6> [ Links ]
4. Pires JG, Nunes MF, Demarzo MM, Nunes CH. Instruments for assessing the construct mindfulness: a review. Aval Psicol. [Internet]. 2016 Feb [cited 2018 Apr 5];14(3):329-38. Available from: <http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1677-04712015000300005&lng=en&nrm=iso&tlng=pt> [ Links ]
5. Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment. [Internet]. 2006 Mar [cited 2018 Nov 24];13(1):27-45. Available from: <http://journals.sagepub.com/doi/10.1177/1073191105283504> [ Links ]
6. Kabat-Zinn J, Lipworth L, Burney R. The clinical use of mindfulness meditation for the self-regulation of chronic pain. J Behav Med. 1985 Jun;8(2):163-90. [ Links ]
7. Kabat-Zinn J, Massion AO, Kristeller J, Paterson LG, Fletcher KE, Pbert L, et al. Effectiveness of a meditation-based stress reduction program in the treatment of anxiety disorders. AJP. [Internet]. 1992 Jul [cited 2019 Jun 3];149(7):936-43. Available from: <http://psychiatryonline.org/doi/abs/10.1176/ajp.149.7.936> [ Links ]
8. Segal ZV, Williams JM, Teasdale JD. Mindfulness-based cognitive therapy for depression. 2nd ed. New York (NY): Guilford Press; 2013. 451 p. [ Links ]
9. Gu J, Strauss C, Bond R, Cavanagh K. How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clin Psychol Rev [Internet]. 2015 Apr [cited 2019 Dec 12];37:1-12. Available from: <https://linkinghub.elsevier.com/retrieve/pii/S0272735815000197> [ Links ]
10. Hofmann SG, Sawyer AT, Witt AA, Oh D. The effect of mindfulness-based therapy on anxiety and depression: a meta-analytic review. J Consult Clin Psychol. [Internet]. 2010 [cited 2018 Nov 26];78(2):169-83. Available from: <http://doi.apa.org/getdoi.cfm?doi=10.1037/a0018555> [ Links ]
11. Kuyken W, Warren FC, Taylor RS, Whalley B, Crane C, Bondolfi G, et al. Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse: an individual patient data meta-analysis from randomized trials. JAMA Psychiatry. [Internet]. 2016 Jun [cited 2018 Nov 12];73(6):565. Available from: <http://archpsyc.jamanetwork.com/article.aspx?doi=10.1001/jamapsychiatry.2016.0076> [ Links ]
12. Stillwell SB, Vermeesch AL, Scott JG. Interventions to reduce perceived stress among graduate students: a systematic review with implications for evidence-based practice: interventions to reduce perceived stress. Worldviews Evid Based Nurs. [Internet]. 2017 Dec [cited 2019 Dec 12];14(6):507-13. Available from: <http://doi.wiley.com/10.1111/wvn.12250> [ Links ]
13. Regehr C, Glancy D, Pitts A. Interventions to reduce stress in university students: a review and meta-analysis. J Affect Disord. [Internet]. 2013 May [cited 2019 Dec 12];148(1):1-11. Available from: <https://linkinghub.elsevier.com/retrieve/pii/S0165032712007793> [ Links ]
14. Rith-Najarian LR, Boustani MM, Chorpita BF. A systematic review of prevention programs targeting depression, anxiety, and stress in university students. J Affect Disord. [Internet]. 2019 Oct [cited 2019 Dec 12];257:568-84. Available from: <https://linkinghub.elsevier.com/retrieve/pii/S016503271832754X> [ Links ]
15. Breedvelt JJF, Amanvermez Y, Harrer M, Karyotaki E, Gilbody S, Bockting CL, et al. The effects of meditation, yoga, and mindfulness on depression, anxiety, and stress in tertiary education students: a meta-analysis. Front Psychiatry. [Internet]. 2019 Apr [cited 2019 12 Dec];10:193. Available from: <https://www.frontiersin.org/article/10.3389/fpsyt.2019.00193/full> [ Links ]
16. O'Driscoll M, Byrne S, Mc Gillicuddy A, Lambert S, Sahm LJ. The effects of mindfulness-based interventions for health and social care undergraduate students - a systematic review of the literature. Psychol Health Med. [Internet]. 2017 Aug [cited 2019 Jun 19];22(7):851-65. Available from: <https://www.tandfonline.com/doi/full/10.1080/13548506.2017.1280178> [ Links ]
17. Daya Z, Hearn JH. Mindfulness interventions in medical education: a systematic review of their impact on medical student stress, depression, fatigue and burnout. Med Teach. [Internet]. 2018 Feb [cited 2018 Dec 17];40(2):146-53. Available from: <https://www.tandfonline.com/doi/full/10.1080/0142159X.2017.1394999> [ Links ]
18. Yusufov M, Nicoloro-SantaBarbara J, Grey NE, Moyer A, Lobel M. Meta-analytic evaluation of stress reduction interventions for undergraduate and graduate students. Int J Stress Manag. [Internet]. 2018 May [cited 2018 Dec 17]; Available from: <http://doi.apa.org/getdoi.cfm?doi=10.1037/str0000099>http://revistaseletronicas.pucrs.br/ojs/index.php/revistapsico/article/view/11691/8037 [ Links ]
19. Ministério da Saúde (BR) [Internet]. Portaria nº 971, de 3 de maio de 2006: aprova a política nacional de práticas integrativas e complementares (PNPIC) no sistema único de saúde [Acesso 17 dezembro de 2019]. Disponível em: <http://bvsms.saude.gov.br/bvs/saudelegis/gm/2006/prt0971_03_05_2006.html> [ Links ]
20. National Collaborating Centre for Mental Health. Depression: the treatment and management of depression in adults (Updated Edition) [Internet]. Leicester: The British Psychological Society and The Royal College of Psychiatrists; 2010 [cited 2019 Dec 17]. (NICE Clinical Guidelines). Available from: <https://www.nice.org.uk/guidance/cg90/evidence/full-guideline-pdf-4840934509> [ Links ]
21. The Mindfulness Initiative. The Mindfulness Initiative [Internet]. 2018 [cited 2018 Aug 14]. Available from: <http://www.themindfulnessinitiative.org.uk/> [ Links ]
22. Lopes SA, Vannucchi BP, Demarzo M, Cunha AG, Nunes MP. Effectiveness of a mindfulness-based intervention in the management of musculoskeletal pain in nursing workers. Pain Manage Nurs. [Internet]. 2019 Feb [cited 2020 Jan 26];20(1):32-8. Available from: <https://linkinghub.elsevier.com/retrieve/pii/S1524904217304216> [ Links ]
23. Pizutti LT, Carissimi A, Valdivia LJ, Ilgenfritz CA, Freitas JJ, Sopezki D, et al. Evaluation of Breathworks' mindfulness for stress 8-week course: effects on depressive symptoms, psychiatric symptoms, affects, self-compassion, and mindfulness facets in Brazilian health professionals. J Clin Psychol. [Internet]. 2019 Jun [cited 2020 Jan 26];75(6):970-84. Available from: <https://onlinelibrary.wiley.com/doi/abs/10.1002/jclp.22749> [ Links ]
24. Rodrigues MF, Campos C, Pelucio L, Barreto I, Machado S, Appolinario JC, et al. Patients' comprehension of Mindfulness-Based Cognitive Behavioral therapy in an outpatient clinic for resistant depression: a cross-sectional study. Front Psychol. [Internet]. 2019 Feb [cited 2020 19 May];10:271. Available from: <https://www.frontiersin.org/article/10.3389/fpsyg.2019.00271/full> [ Links ]
25. Britton W, Lindahl J. Meditation Safety Toolbox [Internet]. 2018 [cited 2018 Nov 10]. Available from: <https://www.brown.edu/research/labs/britton/resources/meditation-safety-toolbox> [ Links ]
26. Santorelli SF, Meleo-Meyer F, Koerbel L, Kabat-Zinn J. Mindfulness-Based Stress Reduction (MBSR) authorized curriculum guide [Internet]. Massachusetts: Center for Mindfulness in Medicine, Health Care and Society; 2017 [cited 2018 May 26]. 65 p. Available from: <https://www.umassmed.edu/globalassets/center-for-mindfulness/documents/mbsr-curriculum-guide-2017.pdf> [ Links ]
27. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. [Internet]. 1983 Dec [cited 2019 Dec 17];24(4):385. Available from: <http://www.jstor.org/stable/2136404?origin=crossref> [ Links ]
28. Luft CD, Sanches SO, Mazo GZ, Andrade A. Versão brasileira da escala de estresse percebido: tradução e validação para idosos. Rev Saúde Pública. [Internet]. Ago 2007 [Acesso 5 de abril de 2018];41(4):606-15. Disponível em: <http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-89102007000400015&lng=pt&tlng=pt> [ Links ]
29. Barros VV, Kozasa EH, Souza IC, Ronzani TM. Validity evidence of the brazilian version of the five facet mindfulness questionnaire (FFMQ). Psicol: Teor e Pesq. [Internet]. 2014 Sep [cited 2018 Apr 5];30(3):317-27. Available from: <http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-37722014000300009&lng=en&tlng=en> [ Links ]
30. Sbicigo JB, Teixeira MA, Dias AC, Dell'Aglio DD. Propriedades psicométricas da escala de autoeficácia geral percebida (EAGP). Psico. [Internet]. 2012 [Acesso 5 de dezembro de 208];43(2):139-46. Disponível em: https://revistaseletronicas.pucrs.br/ojs/index.php/revistapsico/article/view/11691 [ Links ]
31. Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In: Measures in health psychology: a user's portfolio. Causal and control beliefs. Windsor (BRK): NFER-NELSON; 1995. p. 35-7. [ Links ]
32. Souza I, Souza MA. Validação da escala de auto-eficácia geral e percebida. Rev Univ Rural, Sér Ciênc Hum. 2004;26(1-2):12-7. [ Links ]
33. Gomes-Valério JO. Apresentação da versão brasileira definitiva da escala de autoeficácia geral percebida. ENJUPSI XIII; Ago 2016; Juiz de Fora, MG. [ Links ]
34. Conselho Federal de Psicologia. Resolução CFP nº 010/05, de 21 de julho de 2005: aprova o código de ética profissional do psicólogo [Internet]. 2005 [Acesso 10 nov 2018]. Disponível em: <https://site.cfp.org.br/wp-content/uploads/2012/07/codigo-de-etica-psicologia.pdf> [ Links ]
35. The British Association of Mindfulness-Based Approaches [BAMBA]. Good practice guidelines for teaching mindfulness-based courses [Internet]. 2015 [cited 2020 Jan 26]. Available from: <https://bamba.org.uk/wp-content/uploads/2019/12/GPG-for-Teaching-Mindfulness-Based-Courses-BAMBA.pdf> [ Links ]
36. McConville J, McAleer R, Hahne A. Mindfulness training for health profession students-the effect of mindfulness training on psychological well-being, learning and clinical performance of health professional students: a systematic review of randomized and non-randomized controlled trials. Explore. [Internet]. 2017 Jan [cited 2019 Dec 18];13(1):26-45. Available from: <https://linkinghub.elsevier.com/retrieve/pii/S1550830716301616> [ Links ]
37. Bodenlos JS, Wells SY, Noonan M, Mayrsohn A. Facets of dispositional mindfulness and health among college students. J Altern Complement Med. [Internet]. 2015 Oct [cited 2020 Feb 29];21(10):645-52. Available from: <http://www.liebertpub.com/doi/10.1089/acm.2014.0302> [ Links ]
38. Hölzel BK, Lazar SW, Gard T, Schuman-Olivier Z, Vago DR, Ott U. How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspect Psychol Sci. [Internet]. 2011 Nov [cited 2018 Apr 5];6(6):537-59. Available from: <http://journals.sagepub.com/doi/10.1177/1745691611419671> [ Links ]
39. Burger K, Samuel R. The role of perceived stress and self-efficacy in young people's life satisfaction: a longitudinal study. J Youth Adolescence. [Internet]. 2017 Jan [cited 2020 Feb 29];46(1):78-90. Available from: <http://link.springer.com/10.1007/s10964-016-0608-x> [ Links ]
40. Molero Jurado MM, Pérez-Fuentes MC, Oropesa Ruiz NF, Simón Márquez M M, Gázquez Linares JJ. Self-efficacy and emotional intelligence as predictors of perceived stress in nursing professionals. Medicina. [Internet]. 2019 Jun [cited 2020 Feb 29];55(6):1-14. Available from: <https://www.mdpi.com/1010-660X/55/6/237> [ Links ]
41. Demarzo MM, Montero-Marin J, Puebla-Guedea M, Navarro-Gil M, Herrera-Mercadal P, Moreno-González S, et al. Efficacy of 8- and 4-session mindfulness-based interventions in a non-clinical population: a controlled study. Front Psychol. [Internet]. 2017 Aug [cited 2018 5 Apr];8. Available from: <http://journal.frontiersin.org/article/10.3389/fpsyg.2017.01343/full> [ Links ]
42. Ruths FA, de Zoysa N, Frearson SJ, Hutton J, Williams JM, Walsh J. Mindfulness-based cognitive therapy for mental health professionals: a pilot study. Mindfulness. [Internet]. 2013 Dec [cited 2019 Dec 18];4(4):289-95. Available from: <http://link.springer.com/10.1007/s12671-012-0127-0> [ Links ]
43. Soler J, Cebolla A, Feliu-Soler A, Demarzo MM, Pascual JC, Baños R, et al. Relationship between meditative practice and self-reported mindfulness: the MINDSENS composite index. Zhang N, organizador. PLoS ONE. [Internet]. 2014 Jan [cited 2020 Jan 5];9(1):e86622. Available from: <https://dx.plos.org/10.1371/journal.pone.0086622> [ Links ]
44. Barnes N, Hattan P, Black DS, Schuman-Olivier Z. An examination of mindfulness-based programs in US medical schools. Mindfulness. [Internet]. 2017 Apr [cited 2019 Dec 18];8(2):489-94. Available from: <http://link.springer.com/10.1007/s12671-016-0623-8> [ Links ]
45. Lu F, Xu Y, Yu Y, Peng L, Wu T, Wang T, et al. Moderating effect of mindfulness on the relationships between perceived stress and mental health outcomes among chinese intensive care nurses. Front Psychiatry. [Internet]. 2019 Apr [cited 2020 Jan 4];10:260. Available from: <https://www.frontiersin.org/article/10.3389/fpsyt.2019.00260/full> [ Links ]
46. Lee AC, Harvey WF, Price LL, Morgan LP, Morgan NL, Wang C. Mindfulness is associated with psychological health and moderates pain in knee osteoarthritis. Osteoarthr Cartil. [Internet]. 2017 Jun [cited 2020 Jan 4];25(6):824-31. Available from: <https://linkinghub.elsevier.com/retrieve/pii/S1063458416301534> [ Links ]
47. Pleman B, Park M, Han X, Price LL, Bannuru RR, Harvey WF, et al. Mindfulness is associated with psychological health and moderates the impact of fibromyalgia. Clin Rheumatol. [Internet]. 2019 Jun [cited 2020 Jan 4];38(6):1737-45. Available from: <http://link.springer.com/10.1007/s10067-019-04436-1> [ Links ]
48. Firth AM, Cavallini I, Sütterlin S, Lugo RG. Mindfulness and self-efficacy in pain perception, stress and academic performance: the influence of mindfulness on cognitive processes. PRBM. [Internet]. 2019 Jul [cited 2019 Dec 17];Volume 12:565-74. Available from: https://www.dovepress.com/mindfulness-and-self-efficacy-in-pain-perception-stress-and-academic-p-peer-reviewed-article-PRBM. [ Links ]
Received: Jan 6th 2020 Author's Contribution Corresponding Author:
Corresponding Author:
Mariana Ladeira de Azevedo
E-mail: mariana_azevedo@hotmail.com
Accepted: June 12th 2020
Study concept and design: Mariana Ladeira de Azevedo and Carolina Baptista Menezes. Obtaining data: Mariana Ladeira de Azevedo and Carolina Baptista Menezes. Data analysis and interpretation: Mariana Ladeira de Azevedo and Carolina Baptista Menezes. Statistical analysis: Mariana Ladeira de Azevedo and Carolina Baptista Menezes. Drafting the manuscript: Mariana Ladeira de Azevedo and Carolina Baptista Menezes. Critical review of the manuscript as to its relevant intellectual content: Mariana Ladeira de Azevedo e Carolina Baptista Menezes.
All authors approved the final version of the text.
Conflict of interest: the authors have declared that there is no conflict of interest.
* This article refers to the call "Mindfulness and other contemplative practices".


{kind=link}
{kind=link}