










Serviços Personalizados
artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versão On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.16 no.3 Ribeirão Preto jul./set. 2020
http://dx.doi.org/10.11606/issn.1806-6976.smad.2020.166027
REVIEW ARTICLE
Mindfulness-based interventions for adults and older adults with mental disorders: an integrative review*
Paula Hayasi Pinho ; Lígia Maffei Carnevalli; Renata Oliveira Santos; Luanna Carolyne Silva De Lacerda
; Lígia Maffei Carnevalli; Renata Oliveira Santos; Luanna Carolyne Silva De Lacerda
Universidade Federal do Recôncavo da Bahia, Centro de Ciências da Saúde, Santo Antônio de Jesus, BA, Brazil
ABSTRACT
OBJECTIVE: to analyze the evidence of how the practice of mindfulness-based interventions has been used therapeutically and what are the effects of these interventions on adults and the elderly affected by mental disorders.
METHOD: integrative review of articles published between 2008 and 2018, based on: Virtual Health Library, Scientific Electronic Library Online and PubMed. After applying the inclusion and exclusion criteria and the PRISMA methodology, 37 articles were selected to be analyzed.
RESULTS: variability was found in the methods of mindfulness-based interventions, with Mindfulness-Based Stress Reduction (MBSR), Mindfulness-Based Cognitive Therapy (MBCT) and Mindfulness-Based Relapse Prevention (MBRP) the most widely used. The practices of mindfulness-based interventions have shown physiological benefits, improved psychological and emotional well-being and have been shown to modulate social interaction. Positive influences were observed in the management of stress, in the reduction of the degree of anxiety and symptoms of depression and in the development of attention. Promising findings have been found on the use of these practices in individuals with psychotic symptoms.
CONCLUSION: it is suggested that the practice of mindfulness-based interventions develops skills that assist in the therapeutic process of various mental disorders.
Descriptors: Mindfulness; Therapeutics; Mental Disorders; Mental Health; Adult; Aged.
Introduction
In the clinical health context, meditation was brought to the USA in the late 1970s by Kabat-Zinn, who created an 8-10 week program initially for those suffering from chronic pain, with no medical possibilities(1). Subsequently, the program was expanded to anxious individuals and obtained promising results for the reduction of anxiety and depression(1). This program, at that time, was entitled "Mindfulness-Based Stress Reduction Therapy" (MBSR), and is a model for several adaptations made in research studies.
It is important to highlight that mindfulness, when translated into Portuguese, is synonymous with full attention. And practicing it is to being consciously and intentionally aware of the present moment and the experience of the moment, without feeling absorbed by it(2).
Training mindfulness or full attention develops the ability to be less reactive to everyday events; however, it requires regular practice to maintain the benefits(3). Mindfulness practices are divided into formal and informal(3). Meditation refers to the formal practice, which allows for the training of attention through disciplined introspection and the experience of mindfulness at deep levels, through breathing or movement exercises: conscious progressive muscle relaxation. The informal practice, on the other hand, occurs through the application of mindfulness abilities in daily life(3), that is, directed to listening to ambient sounds, describing emotions or perceiving bodily sensations, or the taste and texture of food, for example.
Among chronic diseases, and occupying a large space in relation to worldwide prevalence, there are mental disorders (MDs), of multiple etiologies, which can affect individuals regardless of sex, gender and social class. In this context, the therapeutic effect of mindfulness has been positive for depression(4), generalized anxiety(5), social anxiety, abuse of alcohol and other drugs(5), and post-traumatic stress disorder, among others.
High rates of disability and mortality among people with MD are evidenced from a study(7) on the global burden of diseases, injuries and risk factors (GBD). In the American continent, GBD estimates point to alcohol abuse and suicide as the main causes of disability and mortality(7). In Brazil, according to data from the World Health Organization(8), it is estimated that, for every 100 people, 30 may come to develop mental health problems, such as depression (5.8%) and anxiety (9.3%).
In this sense, from the perceived need of auxiliary practices for those in psychological distress, in contrast to hegemonic practices that induce the medicalization of life, the objective was to conduct an integrative literature review to analyze the evidence of how the practice of the mindfulness-based interventions has been used therapeutically and what the effects are of these interventions in adults and the older adults affected by mental disorders.
Method
This is an integrative literature review in which both theoretical and empirical elements can be used(9). The stages leading to this review were the following: identification of the theme and selection of the research question; establishment of inclusion and exclusion criteria for data collection; identification of the pre-selected and selected studies and categorization of the selected studies; evaluation of the studies included in the integrative review; analysis and interpretation of the results and presentation of the knowledge review/synthesis(10).
It was sought to answer the following research question: "What is the scientific production on the practice of mindfulness in adults and in older adults with some mental disorder?", elaborated by means of the "Population/Problem, Interest and Context" (PICo) strategy. Strategy based on the segmentation of the research question allowing the researcher to select words that bring out the appropriate definition to the initial questioning, identifying the best scientific information on the topic(11).
Data collection took place in August 2019. The following databases were used to select these articles: Virtual Health Library (Biblioteca Virtual em Saúde, BVS), Scientific Electronic Library Online (SCIELO) and PubMed. The descriptors in health sciences (DeCS) being used and combined were the following: "mindfulness" AND "mental health".
Original studies and literature reviews written in the form of electronic articles were included from 2008 to 2018, in Portuguese, English and Spanish. The following were excluded: theses, dissertations, editorials, non-scientific materials, articles in which no relationship with the theme was identified, duplicates, or that did not address the adult and older adult population.
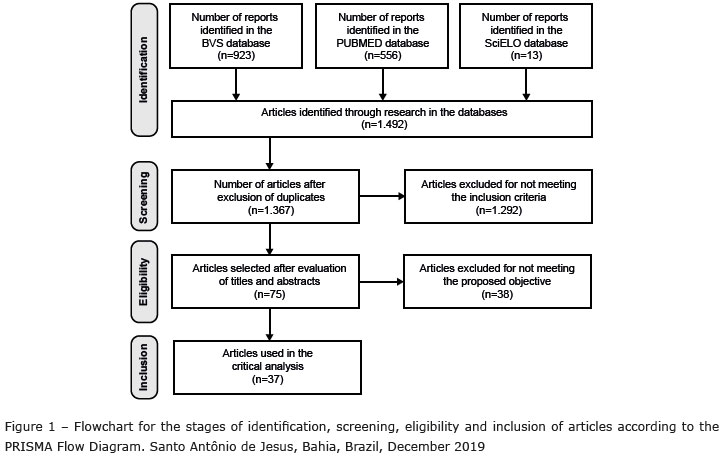
Two reviewers carried out the search and selection of the articles independently, conferring greater accuracy to this procedure. Initially, the studies were selected by reading the titles and abstracts based on the inclusion and exclusion criteria. From this selection, the remaining articles were read in full, with the objective of including only the relevant publications pertinent to the problem of this study. Figure 1 shows the study selection process according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses(12) (PRISMA) protocol.
The corpus of analysis consists of 37 studies, which were submitted to new reading for extraction of relevant information, considering the guiding question of this study. To organize the data collected, the researchers developed an instrument including the following information: authors, year of publication, language, location and type of study.
In this review, the type of study/level of evidence was classified into: Level I: Systematic review or meta-analysis of randomized controlled trials or clinical guidelines based on systematic reviews of randomized controlled trials; Level II: At least one well-designed randomized controlled clinical trial; Level III: Well-designed clinical trials without randomization; Level IV: Well-designed cohort or case-control studies; Level V: Systematic review of descriptive and qualitative studies; Level VI: A single descriptive or qualitative study; Level VII: Authority opinion and/or expert committee report(13).
Results
From the search in online platforms, 1, 492 articles were found. Of these, following the PRISMA methodology, 37 were selected to compose the database of this integrative review. The studies were published as original articles (89.1%), review articles (5.4%), case reports (2.7%) and meta-analyses (2.7%) between 2008 and 2018, with 2016 being the year with the largest number of publications (35.1%). The place where the studies were carried out varied mostly between the United States (48.6%), the United Kingdom (13.5%), and Australia (8.1%). All were published in English (Figure 2).
According to the systematization of levels of evidence(13), the largest and smallest number of articles have been classified as Level VI(19, 21, 23-24, 28-30, 35-37, 40, 42, 45, 48) (37.8%) and Level I(25.49) (5.4%), respectively; none of the 37 items were classified as levels V and VII; 21.6% corresponded to Level II(20, 27, 32, 38-39, 44, 46-47); 18, 9% to Level III(15, 17, 22, 24, 33-34, 43); and 16.2%, to Level IV(14, 16, 18, 31, 41, 50). As for the design of the studies, 43.2% have a quantitative characteristic(15-18, 20, 26-27, 32-34, 38, 41, 43-44, 46-47), 40.5% qualitative(19, 21, 23-25, 28-29, 35-37, 40, 42, 48-49) and 16.2% quanti-qualitative(14, 22, 30-31, 39-50).
The target audience of the studies, previously established as adults and older adults (individuals over 18 years old), showed a variation among undergraduate and/or graduate students(14, 16-18, 22, 32, 34, 37, 41), health professionals(29, 31, 35), and mental-health teams(23, 30), among others.
The practice of Mindfulness-based interventions in adults and older adults with some MD was explored in different aspects in the articles. In addition to variations in the way the technique is applied, the types of MD submitted by the study participants are also varied, including those derived from and/or aggravated in work environments.
From the central themes identified in the reviewed studies, four thematic categories emerged: (1) Types of interventions in mindfulness(14, 18-20, 23-24, 30-31, 36-40, 42-43, 45-49); (2) Mindfulness and mental disorders(14-16, 18-28, 30-32, 34-50); (3) Mindfulness and the work environment(14, 17, 23, 29, 31, 34-35); and (4) Benefits of mindfulness(14, 16-20, 23, 25-33, 35, 37, 39, 41-42, 44, 47).
In the "Types of interventions in mindfulness" category, there are studies that explore the methodology and principles of applying mindfulness. In the "Mindfulness and mental disorders" category, MDs presented by the study participants are addressed, seeking to relate possible effects of the practice of mindfulness on the characteristic behaviors and symptoms. Also in this context, in "Mindfulness and the work environment", there are studies that cover mindfulness interventions in organizations/corporations in order to prevent burnout and/or mitigate it. Finally, studies regarding the effects perceived from the practice of mindfulness in physiological, psycho-emotional, social, physical and/or environmental spheres were gathered in the "Benefits of mindfulness" category.
Among the types of mindfulness-based interventions (MBIs), a variety of methodologies and purposes of application of the technique were noted, and distinctions such as: whether the interventions occur in a group or individually, and in a face-to-face manner or online.
The best known intervention among the MBIs is the Mindfulness Based Stress Reduction (MBSR) program, which takes place in eight weekly sessions lasting two hours to practice full attention through meditation exercises, psychoeducation and group discussions, and a full day in a silent retreat between the sixth and seventh week(42). University students(14, 18, 37, 41) and health professionals(23, 30) were the major targets for this intervention among the analyzed articles.
Also in this context, there is the Mindfulness Based Cognitive Therapy (MBCT), in which individuals who practice MBCT are taught to recognize and disengage from the rumination of thoughts, becoming aware of them and of their feelings so as not to overvalue them and thus prevent and reduce depressive thinking and possible relapses(43).
When considering the relationship between the commitment to the mindfulness practices and their results, the effectiveness is discussed of treatments based on full attention when performed via Internet, another type of MBI. Despite the adaptations, the reduction in anxiety, depression and insomnia symptoms, and a moderate improvement in quality of life, adherence remains a limitation of the treatment(20).
The relationship between the engagement of the practice of mindfulness and its results can be associated with less emotional suffering and with a more positive mental state among the users(39) of psychoactive substances (PAS) that integrate another type of intervention found in the articles: Mindfulness Based Relapse Prevention (MBRP).
The practice of mindfulness-based interventions provided significant reductions in anxiety symptoms, increased well-being and quality of life(41, 45). More attentive perception of internal and external experiences, improved attention, and greater awareness of daily activities were other abilities acquired(31, 42).
Regarding the practice of mindfulness-based interventions for people with depression, the information is conflicting because, despite not finding significant changes in the score(41) of this MD, there is evidence for remission(36) of the anxiety and depression symptoms. With regard to recurrent depression, the regular practice of mindfulness can reduce residual symptoms of depression(47). Furthermore, even within depressive disorders, the MBIs can reduce the risk of suicidal ideation or its severity in individuals with severe depression(22), including those with previous suicidal behavior(24).
As far as psychological stress is concerned, the practice of mindfulness-based interventions has positively influenced the practitioners' well-being and quality of life, increasing acceptance, observational abilities and self-compassion, as well as reducing perceived stress(16, 31). They also enabled greater awareness and control of stress, as well as the development of abilities to manage it(14). In contrast, another study(18) found no statistically significant reduction in the stress levels, despite presenting increased acceptance and improved observational abilities. Therefore, full attention was only considered as a possible protective factor for stress(18, 26).
For people with psychotic symptoms, the practice of mindfulness-based interventions led to a reduction of anxiety and depression symptoms and relieved the negative symptoms of people with schizotypia, as it is a practice that develops consciousness centered on the present(15). In contrast, no relationship was found between mindfulness and negative symptoms of schizophrenia, but the practice is associated with decreased inhibitory behaviors, increased adaptability of emotional regulation, and ease of coping with dysfunctional attitudes in people living with this disease(50). In a ward for individuals with chronic psychosis and resistant to treatment, mindfulness practices were perceived as a relaxing, comfortable and accessible therapy, being considered acceptable in this environment(40).
There is evidence on mindfulness practices in the care of people with PAS-related disorders as a possibly effective practice in managing the consequences of this use(48) and the withdrawal symptoms(21). The ability to maintain attention in the immediate experience and acceptance in relation to the experiences lived are the main beneficial points worked on in this practice, as they understand the process of associative learning, developing a critique on the fissure for the use of PAS(21). From this, the conscious change related to the desire from non-judgment would provide concrete and effective changes in the abusive use of the substances.
The practice of mindfulness-based interventions was also observed in the treatment of the Burnout Syndrome(17, 29, 33, 35) perceived among the target audiences studied by the articles on mindfulness and work environment included in this review: psychiatric resident physicians(17); a mental health ward team for adolescents(23); psychologists(29); multidisciplinary health team(30); nurses(30); and social service professionals(35).
Lower burnout levels were associated with the practice of mindfulness-based interventions(29, 31, 34, 39); and improved communication abilities, increased awareness of their actions, and increased awareness of emotional and cognitive patterns were reported after the practices(17, 23, 30-31). Empathy was another ability developed from mindfulness practices that was highlighted(17, 23), being related to lower burnout levels, better relationships with co-workers and greater attention with the patients(17, 23). In addition, there was an increase in listening abilities(17); greater ability to focus at the consultation times(17, 23); and improved ability to communicate internal experiences through words(31).
Since interpretations of everyday events are affected by the practice of full attention and the development of non-judgmental thinking, it was identified that mental flexibility and the ability to see distressing thoughts and emotions as transient events reduces the negative impact of stressful events(19). On a physiological level, the perceived effects are related to decreased cortisol levels(26), increased telomerase activity, and maintenance of blood pressure and heart rate at healthy levels(19).
Other aspects perceived and expressed in relation to quality of life and well-being are autonomy(21, 23, 31), the ability to calm down with mindfulness techniques alone(16, 31) and self-care(18, 31). The relationship between the practice of mindfulness and feeling capable was linked to reports on how the practice promotes the stimulus to become active self-healers and agents for change(37), as well as the improvement of psychological health through self-care(18). Finally, in addition to the changes at a personal level, mindfulness can appear as a modulating tool for social interaction(37).
Discussion
For Mindfulness-Based Interventions (MBIs) to be considered as such, they must be based individually or separately on the observation of the body, sensations, mind and mental attitudes(51), the foundations of full attention explained in Satipatthana Sutta(52). The most widely used technique in the analyzed studies, Mindfulness Based Stress Reduction (MBSR), is applied as prevention(53) and mitigation(54) for the physical or emotional exhaustion in healthy individuals, and in those subjects facing stress episodes, respectively.
In relation to depressive conditions and relapses of depression, it is by encouraging participants to focus in detail on the environment around them and accept the sensitive experiences that arise, without judgment and without avoiding them, that the Mindfulness Based Cognitive Therapy (MBCT) refines awareness and the withdrawal of repetitive negative thinking(55), one of the symptoms present in depressive conditions(56).
In treating individuals affected by depression, however, feasibility and effectiveness should consider the difficulty of these individuals in adhering to sessions of mindfulness-based interventions(24). Thus, for a better outcome of their effects, the choice of the appropriate time for their practice is important(14), since greater benefits are perceived from greater engagement with the sessions(18). This is because the longer the time devoted to meditation, the greater the chances of results in the ability to apply full attention to daily events and therefore better psychological benefits(42).
The relationship between engagement and results is also important in Mindfulness Based Relapse Prevention (MBRP), an approach aimed at users of psychoactive substances (PAS) that integrates the principles of MBSR and MBCT(57). This MBI works on raising awareness of early warning signs of relapse, recognition of triggers and internal reactions associated with the use of PAS, the development of effective coping abilities and encouraging behavioral choices focused on acceptance and tolerance(57). The cultivation of full attention can be associated with less emotional suffering and with a more positive mental state among users(39) of PAS. Thus, the aim is to reduce the impetus in order to alleviate the discomfort associated with the use, promoting the prevention of relapse and stimulating interpersonal relationships that reinforce this protection network(58).
In the context of mindfulness-based interventions applied to MDs, stress management, anxiety reduction and focus development can be achieved through MBIs(59). Nevertheless, caution is recommended when indicating the practice of mindfulness for individuals with anxiety disorders, as the poorly applied technique may, for example, generate more anxiety in an already anxious person, hindering therapy(59). Encouraging the individual not to create expectations regarding the results of each meditation contributes to a better practice and greater motivation of the subject(60).
Besides the reduction of residual symptoms of depression(47), it was also perceived that the greater the risk of relapse, the greater the effectiveness of the MBCT practice(61). This practice can be as effective as the use of antidepressant drugs, in a period of two years(61), because its practices help to reduce symptoms, increase quality of life and the level of attention(43), since it allows understanding the moment of relapse of the disease by stimulating the autonomy to get out of it with the help of the MBCT techniques(62). Moreover, the practice has been considered effective in reducing suicide ideation(63-64).
The effectiveness of mindfulness-based interventions was classified as moderate for the reduction of negative symptoms, affective symptoms and improved quality of life for psychotic patients(65). These practices can be considered as a safe and effective strategy for reducing levels of depression, improving the ability to observe emotions and act with awareness for people with early psychosis(66), who felt more calm, found it a pleasant experience and reported an improvement in the perception of living with a MD(67). In general, it is interesting to note that mindfulness-based interventions may come to help reducing the suffering associated with psychotic symptoms, as it helps in the perception of emotions and openness to internal experiences(68).
Regarding the mental disorders related to the use of PAS, MBIs can assist in cognitive control in situations of emotional vulnerability, helping the individual to deal with these moments and interrupt automatic behaviors. The greater ability to describe emotional experiences; the implicit emotional adaptation and self-regulating emotional response provided by the practice of mindfulness-based interventions are responsible for the reduction of deficits and of the negative emotional states in these patients(69).
In general, the mindfulness approach is considered advantageous over other approaches because it has a moderate impact on anxiety and depressive symptoms; and high for perceived desire levels, negative affectivity and post-traumatic symptoms(70).
Regarding the MBIs and the work environment, it should be considered that the increasingly precarious work environment, surrounded by a framework of increasing competition and insecurity for the workers(71), impacts on their health and influences their well-being and productivity, resulting in physical and mental illness and, cyclically, in greater precariousness of the work environment(72). In this context, MBIs become a tool for improving the quality of life and well-being of the workers(73).
In the case of the Burnout Syndrome, which is related to chronic exposure to stressful factors in the work environment and consists of the dimensions of emotional exhaustion (EE), depersonalization (DE) and low professional achievement (LPA) (74) in order to affect the health of the worker dealing with the direct care of the subjects(75-76), the MBIs and self-compassion are suggested as effective practices in their prevention(29, 34-35), as they work with the reduction of perceived stress and tension(77). In addition to the improvement in the social abilities related to communication and interpersonal relationships(78), essential to care and assistance(79-80) and, in addition, they are workspace requirements(81).
In relation to productivity, MBIs help to increase dedication to work, decrease job turnover and distraction, increase performance within this space, and help in emotional regulation(73).
The benefits of mindfulness, finally, are about the positive effects of this practice in physiological, psychoemotional, social, physical and/or environmental spheres. Basal cortisol levels decreased linearly and significantly after the MBIs(82-83), and the ability to maintain telomerase activity was increased through the meditation practice, which leads to the individuals experiencing less stress, anxiety and depression(84).
From the methodology of full attention to behaviors and body sensations, connections between body sensory stimuli and mental processes can be amplified and strengthened(85). Through meditation focused on one's own heartbeat, for example, MBI results indicate improved activity in the insular, somatomotor and cingulate cortices(86). Such changes in cortical levels from the practice of mindfulness are possibly responsible for the improvement of the brain functions linked to attention, memory, executive function, processing speed and general cognition(19, 87).
In studies conducted with older adults, these positive effects in cognitive domains configure a factor of better emotional health(19, 26), since greater awareness of their actions interferes with mental and physical health(88). Thus, the practice of mindfulness is indicated as positively related to vitality, satisfaction and quality of the relationship with oneself and of interpersonal relationships(89).
Finally, the use of MBI practices as modulators for social interaction is possible, because this practice helps to develop a consciousness focused on the present, where the physical presence of other people can be enough to provoke greater social attention and enable the development of empathy and simple social decision-making(90-91). In addition, it is worth highlighting the importance of the social network strengthened in cases of MBIs focused on substance users, since social reinsertion involves behaviors of internal and external acceptance and tolerance that configure a new lifestyle, preventing relapse in the face of daily situations faced by the subjects(58).
Final Considerations
Mindfulness-based intervention practices have been therapeutically employed in adults and older adults affected by mental disorders as purpose-specific programs. Mindfulness Based Stress Reduction (MBSR), Mindfulness Based Cognitive Therapy (MBCT), and Mindfulness Based Relapse Prevention (MBRP) have been the most widely used programs in the analyzed articles. The results of the MBIs were dependent on the variations in the purposes of each technique and in the dimensions of the practices, requiring attention to the population in which the technique will be used, the context and the objectives to be achieved. The use of mindfulness practices via Internet must be emphasized because, although some studies present benefits on these, there are limitations regarding adherence to the therapeutic process, besides obstacles regarding therapeutic orientation and social interaction, which are not very effective via Internet.
The MBIs showed promising effects and results in the adult and older adult population, such as its association with the reduction of anxiety and depression symptoms, apart from being effective in the prevention of relapses and in the control of emotions; the reduction of the suicidal ideation risk in patients with severe depression; and the reduction of anxiety and depression symptoms in individuals with psychotic conditions. For the latter, the improvement in negative symptoms and affections was not unanimous in the studies, but even so, the practice brought benefits to the patients, especially in dealing with emotions. Moreover, in work environments, lower burnout levels were associated with the practice of MBIs, and can be considered effective in preventing the syndrome and developing abilities that result in improvements in the work environment, productivity and well-being of the individual.
Finally, caution must be used in the application of any MBI and attention must be paid to the specificities of each population. It is important to observe how the subjects interpret the practice of mindfulness in their life, availability, motivation, and engagement, as well as the creation of expectations and the anxiety developed about the practices and their results.
References
1. Kabat-Zinn J, Massion AO; Kristeller J; Peterson LG; Fletcher KE; Pbet L; Lenderking WR; Santorelli SF. Effectiveness of a Meditation Based Stress Reduction Program in the Treatment of Anxiety Desorders. Am J Psychiatry. 1992;149: 936-43. doi: 10.1176/ajp.149.7.936. [ Links ]
2. Kabat-Zinn J. Full Catastrophe Living: Using the Wisdom of your Mind to Face Estresse. Pain and Illness. [Kindle Version]. New York: Dell Publishing; 1990. [ Links ]
3. Germer CK. Mindfulness: o que é? Qual a sua importância? In: Germer CK, Siegel RD, Fulton P. Mindfulness e Psicoterapia. 2. ed. Porto Alegre: Artmed; 2016. p. 19-46. [ Links ]
4. Keng SL, Smoski MJ, Robins CJ. Effects of Mindfulness on Psychological Health: A Review of Empirical Studies. Clin Psychol Rev. 2011; 31(6): 1041-56. doi: 10.1016/j.cpr.2011.04.006. [ Links ]
5. Hölzel BK, Carmody J, Vangel M, Congleton C, Yerramsetti SM, Gard T et al. Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Res. 2011; 191(1):36-43. doi: 10.1016/j.pscychresns.2010.08.006. [ Links ]
6. Witkiewitz K, Bowen S, Douglas H, Hsucl SH. Mindfulness-Based Relapse Prevention for Substance Craving. Addict Behav. 2013; 38(2). doi: 10.1016/j.addbeh.2012.04.001. [ Links ]
7. James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018 Nov; 392(10159): 1789-858. doi: 10.1016/S0140-6736(18)32279-7. [ Links ]
8. World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates [internet]. Geneva: World Health Organization; 2017. p. 24. [acesso em 18 nov 2019]. Disponível em: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf. [ Links ]
9. Souza MT, Silva MD, Carvalho R. Integrative review: what is it? How to do it? Einstein. 2010; 8(1):102-6. doi: 10.1590/s1679-45082010rw1134. [ Links ]
10. Botelho L, Cunha C, Macedo M. O método da revisão integrativa nos estudos organizacionais. Gestão e Sociedade. 2011 dez; 5(11):121-36. doi: 10.21171/ges.v5i11.1220. [ Links ]
11. Karino ME, Felli VEA. Enfermagem Baseada em Evidências: avanços e inovações em revisões sistemáticas. Ciênc Cuid Saúde. 2012; 11:11-5. doi: 10.4025/cienccuidsaude.v11i5.17048. [ Links ]
12. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009 Jul 21; 6(7):e1000097. doi: 10.1371/journal.pmed.1000097. [ Links ]
13. Melnyk BM, Fineout-overholt E. Evidence-based practice in nursing and health care: a guide to best practice. Philadelphia: Lippincott; 2011. p. 577. [ Links ]
14. Aherne D, Farrant K, Hickey L, Hickey E, McGrath L, McGrath D. Mindfulness based stress reduction for medical students: optimising student satisfaction and engagement. BMC Med Educ. 2016 Ago; 16(1):209. doi: 10.1186/s12909-016-0728-8. [ Links ]
15. Antonova E, Amaratunga K, Wright B, Ettinger U, Kumari V. Schizotypy and mindfulness: Magical thinking without suspiciousness characterizes mindfulness meditators. Schizophr Res Cogn. 2016 May; 5:1-6. doi: 10.1016/j.scog.2016.05.001. [ Links ]
16. Beck AR, Verticchio H, Seeman S, Milliken E, Schaab H. A Mindfulness Practice for Communication Sciences and Disorders Undergraduate and Speech-Language Pathology Graduate Students: Effects on Stress, Self-Compassion, and Perfectionism. Am J Speech Lang Pathol. 2017 Ago; 26(3):893-907. doi: 10.1044/2017_AJSLP-16-0172. [ Links ]
17. Bentley PG, Kaplan SG, Mokonogho J. Relational Mindfulness for Psychiatry Residents: a Pilot Course in Empathy Development and Burnout Prevention. Acad Psychiatry. 2018 Out; 42(5):668-73. doi: 10.1007/s40596-018-0914-6. [ Links ]
18. Bergen-Cico D, Possemato K, Cheon S. Examining the efficacy of a brief mindfulness-based stress reduction (Brief MBSR) program on psychological health. J Am Coll Health. 2013; 61(6): 348-60. doi: 10.1080/07448481.2013.813853. [ Links ]
19. Berk L, Warmenhoven F, van Os J, van Boxtel M. Mindfulness Training for People With Dementia and Their Caregivers: Rationale, Current Research, and Future Directions. Front Psychol. 2018 Jun; 9:982. doi: 10.3389/fpsyg.2018.00982. [ Links ]
20. Boettcher J, Aström V, Påhlsson D, Schenström O, Andersson G, Carlbring P. Internet-based mindfulness treatment for anxiety disorders: a randomized controlled trial. Behav Ther. 2014 Mar; 45(2):241-53. doi: 10.1016/j.beth.2013.11.003. [ Links ]
21. Brewer JA, Elwafi HM, Davis JH. Craving to Quit: psychological models and neurobiological mechanisms of mindfulness training as treatment for addictions. Psychol Addict Behav. 2013 Jun; 27(2):366-79. doi: 10.1037/a0028490. [ Links ]
22. Buitron V, Hill RM, Pettit JW. Mindfulness Moderates the Association Between Perceived Burdensomeness and Suicide Ideation in Adults With Elevated Depressive Symptoms. Suicide Life Threat Behav. 2017 Oct; 47(5):580-88. doi: 10.1111/sltb.12314. [ Links ]
23. Byron G, Ziedonis DM, McGrath C, Frazier JA, deTorrijos F, Fulwiler C. Implementation of Mindfulness Training for Mental Health Staff: Organizational Context and Stakeholder Perspectives. Mindfulness. (NY) 2015 Ago; 6(4):861-72. doi: 10.1007/s12671-014-0330-2. [ Links ]
24. Chesin M, Interian A, Kline A, Benjamin-Phillips C, Latorre M, Stanley B. Reviewing Mindfulness-Based Interventions for Suicidal Behavior. Arch Suicide Res. 2016 Oct-Dec; 20(4):507-27. doi: 10.1080/13811118.2016.1162244. [ Links ]
25. Cramer H, Lauche R, Haller H, Langhorst J, Dobos G. Mindfulness- and Acceptance-based Interventions for Psychosis: A Systematic Review and Meta-analysis. Glob Adv Health Med. 2016 Jan; 5(1):30-43. doi: 10.7453/gahmj.2015.083. [ Links ]
26. Frias CM, Whyne E. Stress on health-related quality of life in older adults: the protective nature of mindfulness. Aging Ment Health. 2015; 19(3): 201-6. doi: 10.1080/13607863.2014.924090. [ Links ]
27. de Vibe M, Solhaug I, Tyssen R, Friborg O, Rosenvinge JH, Sørlie T, Bjørndal A. Mindfulness training for stress management: a randomised controlled study of medical and psychology students. BMC Med Educ. 2013 Ago; 13: 107. doi: 10.1186/1472-6920-13-107. [ Links ]
28. Desrosiersa A, Vineb V, Klemanskib DH, Nolen-Hoeksemab S. Mindfulness and Emotion Regulation in Depression and Anxiety: Common and Distinct Mechanisms of Action. Depress Anxiety. 2013 Jul; 30(7):654-61. doi: 10.1002/da.22124. [ Links ]
29. Di Benedetto M, Swadling M. Burnout in Australian psychologists: correlations with work-setting, mindfulness and self-care behaviours. Psychol Health Med. 2014; 19(6):705-15. doi: 10.1080/13548506.2013.861602. [ Links ]
30. Dobie A, Tucker A, Ferrari M, Rogers JM. Preliminary evaluation of a brief mindfulness-based stress reduction intervention for mental health professionals. Australas Psychiatry. 2016 Feb; 24(1):42-5. doi: 10.1177/1039856215618524. [ Links ]
31. dos Santos TM, Kozasa EH, Carmagnani IS, Tanaka LH, Lacerda SS, Nogueira-Martins LA. Positive Effects of a Stress Reduction Program Based on Mindfulness Meditation in Brazilian Nursing Professionals: Qualitative and Quantitative Evaluation. Explore (NY). 2016 Mar-Apr; 12(2):90-9. doi: 10.1016/j.explore.2015.12.005. [ Links ]
32. Galante J, Dufour G, Vainre M, Wagner AP, Stochl J, Benton A, et al. A mindfulness-based intervention to increase resilience to stress in university students (the Mindful Student Study): a pragmatic randomised controlled trial. Lancet Public Health. 2018 Feb; 3(2):72-81. doi: 10.1016/S2468-2667(17)30231-1. [ Links ]
33. Gawrysiak Michael J, Leongc SH, Grassettid SN, Waib M, Shoreye RC, Baime MJ. Dimensions of distress tolerance and the moderating effects on mindfulness-based stress reduction. Anxiety Stress Coping. 2016 Sep; 29(5):552-60. doi: 10.1080/10615806.2015.1085513. [ Links ]
34. Gerzina HA, Porfeli EJ. Mindfulness as a predictor of positive reappraisal and burnout in standardized patients. Teach Learn Med. 2012; 24(4):309-14. doi: 10.1080/10401334.2012.715255. [ Links ]
35. Harker R, Pidgeon AM, Klaassen F, King S. Exploring resilience and mindfulness as preventative factors for psychological distress burnout and secondary traumatic stress among human service professionals. Work. 2016 Jun 8; 54(3):631-7. doi: 10.3233/WOR-162311. [ Links ]
36. Hazlett-Stevens H. Mindfulness-based stress reduction for comorbid anxiety and depression: case report and clinical considerations. J Nerv Ment Dis. 2012 Nov; 200(11):999-1003. doi: 10.1097/NMD.0b013e3182718a61. [ Links ]
37. Hjeltnes A, Moltu C, Schanche E, Jansen Y, Binder PE. Both sides of the story: Exploring how improved and less-improved participants experience mindfulness-based stress reduction for social anxiety disorder. Psychother Res. 2018 Jan; 28(1):106-122. doi: 10.1080/10503307.2016.1169330. [ Links ]
38. Hoge EA, Guidos BM, Mete M, Bui E, Pollack MH, Simon NM. Effects of mindfulness meditation on occupational functioning and health care utilization in individuals with anxiety. J Psychosom Res. 2017 Apr; 95:7-11. doi: 10.1016/j.jpsychores.2017.01.011. [ Links ]
39. Hosseinzadeh Asl NR, Hosseinalipour F. Effectiveness of Mindfulness-Based Stress Reduction Intervention for Health-Related Quality of Life in Drug-Dependent Males. Iran Red Crescent Med J. 2014 Sep; 16(9):e12608. doi: 10.5812/ircmj.12608. [ Links ]
40. Jacobsen P, Morris E, Johns L. Mindfulness Groups for Psychosis; Key Issues for Implementation on an Inpatient Unit. Behav Cogn Psychother. 2011; 39:349-53. doi: 10.1017/S1352465810000639. [ Links ]
41. Kang YS, Choi SY, Ryu E. The effectiveness of a stress coping program based on mindfulness meditation on the stress, anxiety, and depression experienced by nursing students in Korea. Nurse Educ Today. 2009 Jul; 29(5):538-43. doi: 10.1016/j.nedt.2008.12.003. [ Links ]
42. Lacaille J, Sadikaj G, Nishioka M, Carrière K, Flanders J, Knäuper B. Daily Mindful Responding Mediates the Effect of Meditation Practice on Stress and Mood: The Role of Practice Duration and Adherence. J Clin Psychol. 2018 Jan; 74(1):109-22. doi: 10.1002/jclp.22489. [ Links ]
43. Lilja JL, Zelleroth C, Axberg U, Norlander T. Mindfulness-based cognitive therapy is effective as relapse prevention for patients with recurrent depression in Scandinavian primary health care. Scand J Psychol. 2016 Oct; 57(5): 464-72. doi: 10.1111/sjop.12302. [ Links ]
44. López-Navarro E, Del Canto C, Belber M, Mayol A, Fernández-Alonso O, Lluis J. Mindfulness improves psychological quality of life in community-based patients with severe mental health problems: A pilot randomized clinical trial. Schizophr Res. 2015 Oct; 168(1-2):530-6. doi: 10.1016/j.schres.2015.08.016. [ Links ]
45. Mitchell M, Heads G. Staying Well: A Follow Up of a 5-Week Mindfulness Based Stress Reduction Programme for a Range of Psychological Issues. Community Ment Health J. 2015 Nov; 51(8):897-902. doi: 10.1007/s10597-014-9825-5. [ Links ]
46. Oken BS, Goodrich E, Klee D, Memmott T, Proulx J. Predictors of Improvements in Mental Health From Mindfulness Meditation in Stressed Older Adults. Altern Ther Health Med. [Internet]. 2018 Jan [cited Dec 27 2019] ; 24(1):48-55. Available from: https://www.ncbi.nlm.nih.gov/pubmed/29332020. [ Links ]
47. Radford S, Eames C, Brennan K, Lambert G, Crane C, Williams JM. Trait mindfulness as a limiting factor for residual depressive symptoms: an explorative study using quantile regression. PLoS One. 2014 Jul; 9(7):e100022. doi: 10.1371/journal.pone.0100022. [ Links ]
48. Shorey R, Brasfield H, Anderson S, Stuart GL. Differences in Trait Mindfulness across Mental Health Symptoms among Adults in Substance Abuse Treatment. Subst Use Misuse. 2014 Apr; 49(5):595-600. doi: 10.3109/10826084.2014.850310. [ Links ]
49. Spijkerman MP, Pots WT, Bohlmeijer ET2. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin Psychol Rev. 2016 Apr; 45:102-14. doi: 10.1016/j.cpr.2016.03.009. [ Links ]
50. Tabak NT, Horanb WP, Green MF. Mindfulness in schizophrenia: Associations with self-reported motivation, emotion regulation, dysfunctional attitudes, and negative symptoms. Schizophr Res. 2015 Oct; 168(0):537-42. doi: 10.1016/j.schres.2015.07.030. [ Links ]
51. Coutiño AM. Terapias cognitivo-conductuales de tercera generación (ttg): la atención plena/mindfulness. Rev Int Psicol. 2012 Jul; 12(01). doi: 10.33670/18181023.v12i01.66. [ Links ]
52. Nikaya M [homepage na internet]. Satipatthana Sutta: El Sutra de los fundamentos de la atención [Acceso 20 dic 2019]. Disponíble en: http://www.librosbudistas.com/descargas/SATI.htm. [ Links ]
53. Khoury B, Sharma M, Rush SE, Fournier C. Mindfulness-based stress reduction for healthy individuals: A meta-analysis. J. Psychosom. Res. 2015; 78(6):519-28. doi: 10.1016/j.jpsychores.2015.03.009. [ Links ]
54. Song Y, Lindquist R. Effects of mindfulness-based stress reduction on depression, anxiety, stress and mindfulness in Korean nursing students. Nurse Educ. Today. 2015; 35(1):86-90. doi: 10.1016/j.nedt.2014.06.010. [ Links ]
55. Gu J, Strauss C, Bond R, Cavanagh K. How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clin Psychol Rev 2015; 37:1-12. doi: 10.1016/j.cpr.2015.01.006. [ Links ]
56. Faccioli JS. Efeitos do pensar sobre o passado: pensamentos contrafactuais de estudantes universitários com e sem indicativos de depressão [tese na internet]. São Carlos: Universidade Federal de São Carlos - UFSCAR; 2017 [Acesso 21 dez 2019]. Disponível em: https://repositorio.ufscar.br/handle/ufscar/9393. [ Links ]
57. Bowen S, Chawla N, Collins SE, Witkiewitz K, Hsu S, Grow J, et al. Mindfulness-Based Relapse Prevention for Substance Use Disorders: A Pilot Efficacy Trial. Subst Abus. 2009 Oct-Dec; 30(4):295-305. doi: 10.1080/08897070903250084. [ Links ]
58. Limberger J, Mello LTN, Schneider JA, Andretta I. Mindfulness no Treinamento em Habilidades Sociais para Usuários de Drogas. Rev Bras Ter Cogn. 2017; 13(2):84-91. doi: 10.5935/1808-5687.20170013. [ Links ]
59. Martins MSPP, Seixas PT, Meneses RM, Barreto ESS, Pinto PSP. Mindfulness: um estudo sobre a percepção dos terapeutas cognitivos no público soteropolitano. SEPA - Seminário Estudantil de Produção Acadêmica, UNIFACS; 2017. 16. Disponível em: https://revistas.unifacs.br/index.php/sepa/article/view/5010. [ Links ]
60. Mesquita TO, Furtado TMG. Tratamento da ansiedade através da aplicação de técnicas mindfulness: uma revisão de literatura. Rev Gestão Saúde [Internet]. 2019 [Acesso 27 dez 2019]; 20(1):65-78. Disponível em: http://www.herrero.com.br/files/revista/file1af9a584827d745aa7a4c571890c2cba.pdf. [ Links ]
61. Kuyken W, Hayes R, Barrett B, Byng R, Dalgleish T, Kessler D, Lewis G, Watkins E, Morant N, Taylor RS, Byford S. The effectiveness and cost-effectiveness of mindfulness-based cognitive therapy compared with maintenance antidepressant treatment in the prevention of depressive relapse/recurrence: results of a randomised controlled trial (the PREVENT study). Health Technol Assess. 2015 Sep; 19(73):1-124. doi: 10.3310/hta19730. [ Links ]
62. Williams CM, Meeten F, Whiting S. 'I had a sort of epiphany!' An exploratory study of group mindfulness-based cognitive therapy for older people with depression. Aging Ment Health. 2018 Feb; 22(2):208-17. doi: 10.1080/13607863.2016.1247415. [ Links ]
63. Rizzuti MS. Uso da terapia cognitiva baseada em mindfulness na prevenção de recaída para pacientes com depressão: revisão sistemática. Salvador: Universidade do estado da Bahia (UNEB); 2015 [Acesso 23 dez 2019]. Disponível em: http://www.saberaberto.uneb.br/bitstream/20.500.11896/651/1/TCC%20Mindfulness%20e%20Depressao.pdf. [ Links ]
64. Forkmann T, Wichers M, Geschwind N, Peeters F, van Os J, Mainz V, Collip D. Effects of mindfulness-based cognitive therapy on self-reported suicidal ideation: results from a randomised controlled trial in patients with residual depressive symptoms. Compr Psychiatry 2014;55(8):1883-90. doi: 10.1016/j.comppsych.2014.08.043. [ Links ]
65. Khoury B, Lecomte T, Gaudiano BA, Paquin K. Mindfulness interventions for psychosis: A meta-analysis. Schizophr Res 2013; 150(1):176-84. doi: 10.1016/j.schres.2013.07.055. [ Links ]
66. Miró MT, Arceo J, Ibáñez I. Mindfulness en la Psicosis: Un Estudio Piloto. Rdp. 2016; 27(103):37-56. doi: 10.33898/rdp.v27i103.103. [ Links ]
67. Tong ACY, Lin JJX, Cheung VYK, Lau NKM, Chang WC, Chan SKW, Hui CLM, Lee EHM, Chen EYH. A Low-Intensity Mindfulness-Based Intervention for Mood Symptoms in People with Early Psychosis: Development and Pilot Evaluation. Clin Psychol Psychother .2015; 23(6): 550-60. doi:10.1002/cpp.1981. [ Links ]
68. Carvalho DMH. Processamento da Ameaça na Psicose: o contributo da autoaversão, dos medos da compaixão e do mindfulness. Coimbra: Universidade de Coimbra - Faculdade de Psicologia e de Ciências da Educação UF/FPCE; 2015 [Acesso 29 dez 2019]. Disponível em: https://eg.uc.pt/handle/10316/31693. [ Links ]
69. Henriques ESC. Contributo da Regulação Emocional Implícita para a Eficácia do Treino de Mindfulness na População com Perturbação de Uso de Substâncias. Algarve: Faculdade de Ciências Humanas e Sociais, Universidaded do Algarve; 2018 [ Acesso 29 dez 2019]. Disponível em: https://sapientia.ualg.pt/handle/10400.1/12647. [ Links ]
70. Cavicchioli M, Movalli M, Maffei C. The Clinical Efficacy of Mindfulness-Based Treatments for Alcohol and Drugs Use Disorders: A Meta-Analytic Review of Randomized and Nonrandomized Controlled Trials. Eur Addict Res .2018; 24(3):137-62. doi:10.1159/000490762. [ Links ]
71. Cardoso AC, Morgado L. trabalho e saúde do trabalhador no contexto atual: ensinamentos da Enquete Europeia sobre Condições de Trabalho. Saúde Soc. 2019;28(1) https://doi.org/10.1590/S0104-12902019170507. [ Links ]
72. Duarte RF. Os riscos psicossociais no trabalho e as políticas públicas de preservação da saúde mental do trabalhador. Franca: Universidade Estadual Paulista "Júlio De Mesquita Filho"; 2018 [Acesso 29 dez 2019]. Disponível em: https://repositorio.unesp.br/handle/11449/180559. [ Links ]
73. Markus PMN, Lisboa CSM. Mindfulness e seus beneficios nas atividades de trabalho e no ambiente organizacional. Rev Graduação. [Internet]. 2015 [Acesso 29 dez 2019];8(1). Disponível em: http://revistaseletronicas.pucrs.br/ojs/index.php/graduacao/article/view/20733/0. [ Links ]
74. Aguiar CVN, Silva EEC, Carvalho BR, Ferreira JCM, Jesus KCO. Cultura organizacional e adoecimento no trabalho: uma revisão sobre as relações entre cultura, burnout e estresse ocupacional. Rev Psicol Divers Saúde 2017 Maio;6(2):121-31. doi: 10.17267/2317-3394rpds.v6i2.1157. [ Links ]
75. Silveira KA, Enumo SRF, Paula KMP; Batista EP. Estresse e enfrentamento em professores: uma análise da literatura. Educ Rev. [Acesso 29 dez 2019]; 2014;30(4):15-36. Disponível em: http://www.scielo.br/pdf/edur/v30n4/02.pdf. [ Links ]
76. Picheth CFP, Selow MLC, Toniolo RMM. A gestão de qualidade em profissionais enfermeiros diagnosticados com a síndrome de burnout. Rev Dom Acadêmico. [Internet]. 2016 Jul/Dez Acesso 29 dez 2019]; 1(1):89-109. Disponível em: https://domacademico.unidombosco.edu.br/index.php/domacademico/article/viewFile/11/11. [ Links ]
77. Gracia-Gracia P, Oliván-Blázquez B. Burnout and Mindfulness Self-Compassion in Nurses of Intensive Care Units. Holistic Nurs Practice 2017;31(4):225-33. doi:10.1097/hnp.0000000000000215. [ Links ]
78. Montezeli JH, Almeida KP, Haddad MCFL. Nurses' perceptions about social skills in care management from the perspective of complexity. Rev Esc Enferm USP. 2018;52:e03391. doiI: http://dx.doi.org/10.1590/S1980-220X2017048103391. [ Links ]
79. Albuquerque MCS, Souza DFS, Maynart WHC, Bezerra LFD, Cassimiro ARTS, Cavalcante JC. Empatia dos profissionais de enfermagem de um serviço hospitalar de emergência. Texto Contexto Enferm. 2019;2 e20170406. doi: http://dx.doi.org/10.1590/1980-265x-tce-2017-0406. [ Links ]
80. Almeida Q, Fófano GA. Tecnologias leves aplicadas ao cuidado de enfermagem na unidade de terapia intensiva: uma revisão de literatura. HU Rev. [Internet]. 2016 set/out [Acesso 29 dez 2019]. ;42(3):191-6. Disponível em: https://periodicos.ufjf.br/index.php/hurevista/article/view/2494/891. [ Links ]
81. Galdino CBT, Araujo CF, Cantilino A. Treinamento de Mindfulness aplicado em psicoterapeutas: uma Revisão Narrativa. Rev Bras Terap Cogn. 2014;10(2):65-72. doi: 10.5935/1808-5687.20180009. [ Links ]
82. Carpena MX, Menezes CB. Efeito da Meditação Focada no Estresse e Mindfulness Disposicional em Universitários. Psicologia: Teoria e Pesquisa. 2018. doi: 10.1590/0102.377e3441. [ Links ]
83. Fan Y, Tang YY, Posner MI. Cortisol level modulated by integrative meditation in a dose-dependent fashion. Stress Health. 2014 Feb;30(1):65-70. doi: 10.1002/smi.2497. [ Links ]
84. Alda M, Puebla-Guedea M, Rodero B, Demarzo M, Montero-Marin J, Roca M et al. Zen meditation, Length of Telomeres, and the Role of Experiential Avoidance and Compassion. Mindfulness.2016; 7:651-59. doi: 10.1007/s12671-016-0500-5. [ Links ]
85. Tang YY. The Neuroscience of Mindfulness Meditation. Cham: Palgrave Macmillan; 2017. p. 23-8. doi; 10.1007/978-3-319-46322-3_3. [ Links ]
86. Critchley HD, Wiens S, Rotshtein P, Ohman A, Dolan RJ. Neural systems supporting interoceptive awareness. Nat Rev Neurosci; 2004; 7:189-95. doi: 10.1038/nn1176. [ Links ]
87. Reis WGP. Evidências do papel de mindfulness no aprimoramento das funções executivas [monografia de internet]. Belo Horizonte: Universidade Federal de Minas Gerais, Instituto de Ciências Biológicas; 2014 [Acesso 22 dez 2019]. Disponível em: http://hdl.handle.net/1843/VRNS-9N4FVQ. [ Links ]
88. Silva ACC, Assumpção AA. A influência de mindfulness na qualidade de vida de idosos: revisão narrativa. Pretextos - Psicol Rev. [Internet]; 2018 [Acesso 22 dez 2019]; 3(6):37-51. Disponível em: http://periodicos.pucminas.br/index.php/pretextos/article/view/18404. [ Links ]
89. Antunes GMC. Mindfulness, stresse, psicopatologia e estratégias para a gestão de conflitos em cuidadores de pessoas com incapacidade intelectual [tese na internet]. Coimbra: Instituto Superior Miguel Torga, Escola Superior de Altos Estudos; 2015 [Acesso 22 dez 2019]. Disponível em: http://repositorio.ismt.pt/jspui/handle/123456789/592. [ Links ]
90. Thantrey HH. Relação entre mindfulness, pensamentos automáticos e autocompaixão em população adulta. Instituto de Psicologia Aplicada [tese de internet]. ISPA - Instituto Universitário; 2016 [Acesso 23 dez 2019]. Disponível em: http://repositorio.ispa.pt/handle/10400.12/5106. [ Links ]
91. Van Doesum NJ, Karremans JC, Fikke RC, Lange MA, Van Lange PAM. Social mindfulness in the real world: the physical presence of others induces other-regarding motivation. Soc Influence. 2018; 13(4):209-22. doi: 10.1080/15534510.2018.1544589. [ Links ]
Received: Jan 26th 2020 Author's Contribution Corresponding Author:
Corresponding Author:
Paula Hayasi Pinho
E-mail: paulahpinho@gmail.com
Accepted: May 26th 2020
Study concept and design: Paula Hayasi Pinho. Obtaining data: Paula Hayasi Pinho, Lígia Maffei Carnevalli, Renata Oliveira Santos and Luanna Carolyne Silva De Lacerda. Data analysis and interpretation: Paula Hayasi Pinho, Lígia Maffei Carnevalli, Renata Oliveira Santos and Luanna Carolyne Silva De Lacerda. Statistical analysis: Paula Hayasi Pinho and Luanna Carolyne Silva De Lacerda. Drafting the manuscript: Paula Hayasi Pinho, Lígia Maffei Carnevalli, Renata Oliveira Santos and Luanna Carolyne Silva De Lacerda. Critical review of the manuscript as to its relevant intellectual content: Paula Hayasi Pinho e Luanna Carolyne Silva De Lacerda.
All authors approved the final version of the text.
Conflict of interest: the authors have declared that there is no conflict of interest.
* This article refers to the call "Mindfulness and other contemplative practices".


{kind=link}
{kind=link}