










Servicios Personalizados
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkSMAD. Revista eletrônica saúde mental álcool e drogas
versión On-line ISSN 1806-6976
SMAD, Rev. Eletrônica Saúde Mental Álcool Drog. (Ed. port.) vol.17 no.3 Ribeirão Preto jul./set. 2021
http://dx.doi.org/10.11606/issn.1806-6976.smad.2021.182144
ORIGINAL ARTICLE
World Health Organization guidelines related to human resources in mental health*
Carla Aparecida Arena VenturaI ; Isabel Amélia Costa MendesI; Ana Beatriz Rizzo ZanardoI; Ítalo Rodolfo SilvaII
; Isabel Amélia Costa MendesI; Ana Beatriz Rizzo ZanardoI; Ítalo Rodolfo SilvaII
IUniversidade de São Paulo, Escola de Enfermagem de Ribeirão Preto, PAHO/WHO Collaborating Centre for Nursing Research Development, Ribeirão Preto, SP, Brazil
IIUniversidade Federal do Rio de Janeiro, Campus Macaé, Rio de Janeiro, RJ, Brazil
ABSTRACT
OBJECTIVE: to evaluate, based on key documents, the scope, potential and challenges for the performance of human resources in the mental health area.
METHOD: documentary, descriptive research, carried out based on the analysis of three public domain documents, considered central to the formulation of policies and programs in the mental health area, proposed and approved in the context of WHO and, therefore, applicable to all its member countries. The analytical categories were formulated from the analysis by comparing the data.
RESULTS: in a context in which most countries with low and medium income have few trained and available human resources, the documents demonstrate that the Brazilian reality is not isolated, but a reflection of a culture centered on a predominantly biomedical model in health and also in mental health.
CONCLUSION: the documents demonstrate the weaknesses of mental health services worldwide and the challenges experienced by human resources in this area, since many professionals do not have the appropriate training or are not attracted to work in mental health.
Descriptors: Mental Health; Mental Health Assistance; Workforce; Personnel Management.
Introduction
Mental health is a state of well-being in which an individual puts their own skills in practice, are able to deal with normal life stresses, can work productively and are able to contribute to the community. Several factors can place an individual's mental health at risk. Among them, rapid social changes, stressful working conditions, gender descrimination, social exclusion, an unhealthy lifestyle, violence, and human rights violations. Thus, it is essential to know that mental health is more than the absence of mental disorders as an integral and essential part of health(1).
Mental health has a complex definition, for, in addition to being tied to the question of normalcy or pathology, it involves a discussion on mental disorders and all the stigmas it entails(2). There are several types of mental disorders, with different presentations. Usually characterized by a combination of thoughts, perceptions, emotions, behavior and abnormal relationships with other parties. The burden of mental disorders continues to increase, with significant impacts on health and important social consequences involving human rights and the economy in all countries(3).
In this context, the Psychiatric Reform movement takes place daily seeking comprehensive care, and it is relevant that professionals acting in this context have knowledge regarding the entire network, since a person with mental disorders needs care networks that go beyond disciplinary and sectoral borders(4). Unlike other health sectors that act through harsh technologies, sophisticated devices and exams, in mental health, the technology is essentially human. This means that it is human resource dependent. Thus, mental health professional training assumes singular importance and should form professionals with skills and abilities to act in the different point of care in the health network(5).
However, reaching these goals is not a simple task(5), since the conception and development of global mental health policies constitute processes characterized by challenges and diversification. In this context, its implementation is long and gradual over the centuries, facing financing and human resource scarcity and administrative problems, both in developed and developing countries(6). In this perspective, considering human resources and mental health, a study with professionals belonging to the category shows dissatisfaction in the work, intention to rotate, meaning change departments, in addition to a high number of burnout syndrome cases. Emotional demands such as difficulty of working shifts associated with higher levels of exhaustion were also observed(7).
Furthermore, the curricular workload of medical courses, related to mental health/psychiatry is usually unsatisfactory, with a preponderant theoretical approach, lacking the offer of practical internships with appropriate supervision, giving way, instead to a biomedical model, centered around hospital care and that disregards psychosocial and community aspects(8). This importance is also emphasized(9) for nursing students, being it essential that they are able to experience the role of a nurse and the reality of multi-professional teams according to the precepts of the Psychiatric Reform in practice through the care services. As such, the lack of practical activities in courses involving mental health results in a reality where students do not have the contact needed with individuals and experience involving the care developed in the health care services provided to people with mental disorders, which could reflect in inappropriate training for the professionals of the area, since it is fundamental for these professionals to have communication, relationships, bonding and qualified listening as a basic instrument to the development of their work. Therefore, it is through the human contact established in activities performed within the care services focused on mental health that the student's skills are developed.
Additionally, in order to achieve an effective integration between the mental health services in Primary Health Care within the context of professional training, a few changes are needed, such as: modifications to the education system for health professionals so that the training in mental health can be broader and have a more practical approach, institute processes and appropriate protocols for dissemination and welcoming, referral and transfer of patients with mental health problems, allowing internal communication between the different levels of the health system and the community, and training primary health care professionals to manage and treat all mental health problems, only referring such cases when it is inevitable. In the long run, all of this can facilitate the mental health integration process and increase the distribution of health professionals in different points of attention within the health network to deal with the high workload issue and compromised quality of the care provided(10).
Even in the face of so many challenges, the struggle to make mental health a priority persists and, in this sense, two important events marked the years 2015/2016, signaling changes in the development of the international community and the commitment to address mental health globally: the first concerns the fact that the World Bank has endorsed mental health as a priority for the global development organization and the second was the explicit inclusion of mental health among the goals of the Sustainable Development Goals (2030 Agenda for Sustainable Development). These two events created a singular window of opportunities to work in all sectors and increase financing, research and the level of training in mental health programs(11).
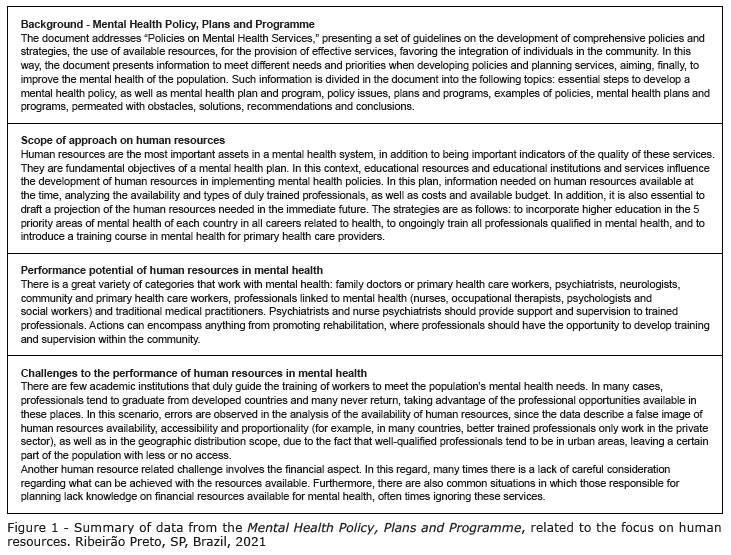
In this context, The World Health Organization (WHO) drafted important documents on mental health, corresponding to the main discussion form among the countries on agendas and priorities in the health industry. Among these documents, the Mental health policy, plans and programmes, stands out as an essential and powerful tool for mental health, based on the precept that when policies are appropriately formulated and implemented through plans and programs, they can lead to significant impact in the mental health of populations(12).
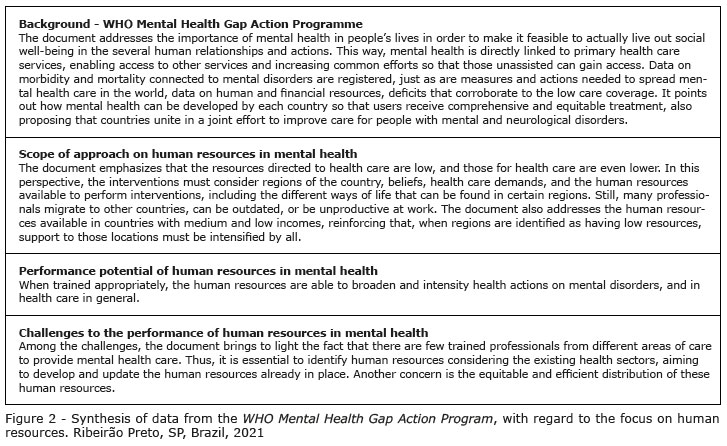
Another important initiative, implemented in 2018, is called the mhGaP Mental Health Gap Action Program and recognizes the need for actions that reduce the burden and increase the capacity of Member States to respond to the growing needs regarding mental and neurological disorders, and substance use, which are highly prevalent and costly worldwide. It also proposes that countries deal with the existing gap between what is needed urgently and what is available to reduce the load that is still too high. Thus, the mhGAP represents an action plan proposed by WHO to expand services meant for mental and neurological disorders, and substance abuse, for all countries, especially those with medium-low incomes(13).
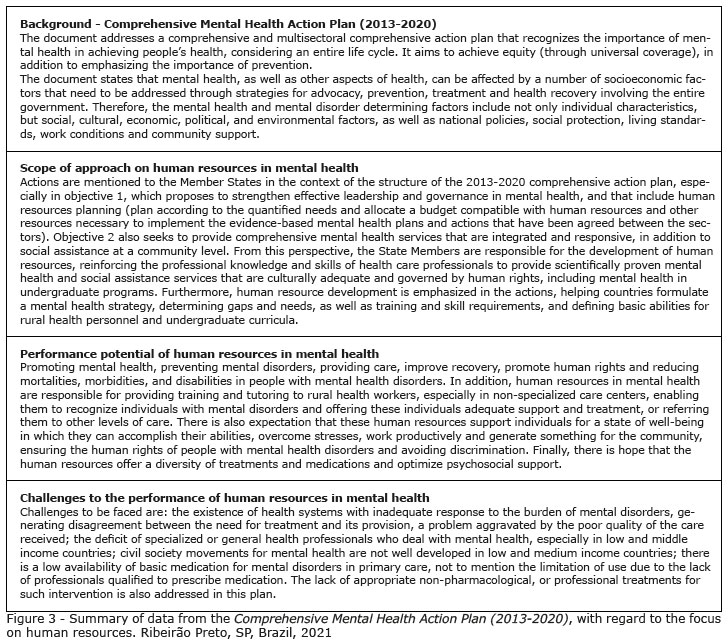
Finally, the Comprehensive Mental Health Action Plan (2013-2020) a comprehensive action plan developed through consultations with member states to civil society and other international partners, is emphasized. With a comprehensive and multisectoral approach, health and social sector service coordination, it grants special attention to the promotion, prevention, treatment, rehabilitation, care and recovery. It also establishes clear actions for Member States, WHO Office and partners at international, regional and national levels, proposing key indicators and targets that can be used to assess the implementation, progress and impact. Front and center of the action plan is the globally accepted principle that "there is no physical health without mental health"(14).
Considering the WHO initiatives and difficulties faced by human resources in mental health, the objective of this study is to assess the scope, potential and challenges to actions by human resources in mental health, based on key documents.
Method
This is a documentary, descriptive research, carried out by analyzing public domain documents. Documentary research refers to the analysis of documents that contain information on the studied phenomenon. It is used in the investigation and categorization of physical sources, most commonly documents. In this perspective, the documentary research method requires strict ethics and can be used in all fields(15).
That considered, this study was based on three documents considered central to the adoption of policies and programs in the area of mental health, formulated and approved within the context of WHO and, therefore, applicable to all member countries, namely: Mental Health Policy, Plans and Programme(12); mhGAP Mental Health Gap Action Programme(13) e Comprehensive Mental Health Action Plan (2013-2020)(14). The list was selected for presenting global proposals related to mental health to be met by the countries. Considering its broader scope, information on human resources in the mental health area was collected.
The documents were read repeatedly by independent researchers, authors of the study who each individually filled out a data collection form they had prepared as a team. This form was made up of the following items: Background; scope of approach on human resources, potential of human resources in mental health, and challenges for human resources in mental health.
The data collection and organization instrument favored the data description synthesis capacity. The comparative data analysis began on each analyzed report following the completion of each item that structured the instrument. This made it possible, for example, to establish the synthesis of the documents with regards the approach to human resources in mental health. The data of this research were collected between October and December 2020.
As they are official, public domain documents accessed online, it was unnecessary to register the research and, consequently, obtain approval from the Research Ethics Committee with human beings, exempting the Free and Informed Consent Term (FICF) for its documentary character. However, it is emphasized that the ethical aspects were respected, considering that the information exposed reflects what the legislation found comprises(16).
Results
Figures 1, 2 and 3 summarize the analysis of the key documents produced by WHO in the area of mental health, complying with the systematic organization of data analysis.
Considering the objective of this study, two thematic categories emerged from the analysis of the documents: Training in mental health as a potential to improve human resources in the area and Implications of mental health (under)financing for Human Resources.
Discussion
Training in mental health as a potential to improve human resources in the area.
Despite the changes identified in the context of practices in mental health care services, such as the implementation of new public policies for the area, there is still much to improve. Considering the growing need to qualify assistance, a rethinking of the professional training process for the development of skills and competences in mental health is undertaken. However, limits are observed in the academic training process of professionals in the area, as well as insufficient practical-theoretical workloads that are below that of other subjects and the lack of discussions around mental health in undergraduate courses(17). This way, the documents analyzed, especially the Mental Health Policy, Plans and Programme, emphasize the importance of establishing training guidelines based on scientific evidence.
In this perspective, human resources with appropriate and adequate training are needed to expand all health interventions, mainly those related to mental health, since care for those with mental disorders depends heavily on health care personnel, not technologies or equipment. The focus on primary care was also highlighted in the documents analyzed by this study.
In this context, it is noteworthy that most countries with low and middle income have few trained and available human resources and, many times, face difficulties to distribute them within the countries or regions (i.e., few personnel in rural areas or too many personnel in large institutional environments). The problem has been accentuated by the migration of trained professionals to other countries. Additionally, people with the needed skills can be outdated or may not meet the needs of the population(13).
Nonetheless, the numbers themself can many times describe a false image of human resource availability, accessibility and proportionality. For example, in many countries, the best trained professionals only act in the private sector. This can leave the majority of the population, especially those most vulnerable, with little to no access to a mental healthcare professional. Therefore, it is necessary to know which professionals are available both in the private and public sectors, and their areas of work, since it is very common all over the world for qualified professionals (including those who work with mental health) to be found mainly in urban areas(12).
In a 2018 survey in Brazil, there were 2.18 doctors in the country for every 1000 inhabitants and only 5 doctors specializing in Psychiatry per 100 thousand inhabitants. There are four specialties that represent 38.4% specialist titles in the country, which are: Medical Clinician, with 42,728 professionals, or 11.2% of the total, Pediatrics, with 39,234 professionals, or 10.3%, General Surgery that unites 34,065 specialists, or 8.9% of the total, and Gynecology and Obstetrics with 8% of holders, with 8% of professionals, or 30,415. The data corroborate the scarcity of mental health professionals in the country(18) .
Thus, what can be achieved in mental health is often limited by what is useful and feasible in terms of the availability of properly trained personnel, which is more pronounced in developing countries. Although in general, countries with few resources include the guarantee of human resources in their planning process (for example, training psychiatrists or mental health nurses, or use plans to guarantee the return of professionals who are already trained but abroad), good planning must take into account the current availability of human resources(12).
It is reinforced, then, that the scarcity of human resources requires pragmatic solutions. Community agents - after specific training and with the necessary support, e.g., telephone consultations with general practitioners - may offer some of the priority interventions(13). The mental health training process, be it academic training or even training and improvement strategies in services, implemented through ongoing education, is seen as a driving force for overcoming challenges, among them teamwork, its best performance, and articulation in the psychosocial scenario.
The need for greater efforts to encourage qualification in mental health, aimed at professionals, as a strategy for strengthening public policies and interventions in this field is recognized, being consolidated through innovative educational practices between services(17). Although, many low-income countries lack the infrastructure and facilities to continuously train health professionals. Other priority issues to be considered in this area are the impact of different training strategies for mental health care providers, treatment results based on traditional medical practices and the effects of different political decisions on access, equity and treatment results(12).
Thus, in order for human resources to be developed, it is necessary to strengthen the knowledge and skills of health professional to provide health care services and social assistance based on the human rights principals. To achieve such goal, one should seek to integrate mental health in undergraduate programs and health care professional training and guidance development in the field, especially in non-specialized care centers, so that the professionals have the ability to recognize people with mental disorders and offer them adequate treatment and support or refer them, as appropriate, to other levels of care(14).
With regard to undergraduate programs, it is vital that educational institutions in health involve their faculties, from all specialties, in discussions on mental health policies, so that they are exposed and conscious of the need to consider health care as comprehensive, including aspects of mental health in their lessons when mentioning other physical aspects. In this way, the faculty will gradually expose and awaken students during the course to a reality which they will face when taking a specific subject involving mental health. Curricula should not be comprised of impervious content. Many times, professionals fail to pay attention to the mental health of those they care for as a result of the curricular rigidity to which they were exposed in training. For this reason, simply investing in human resource development with this focus is insufficient. Such investment is needed, but not enough. Long-term investment, on the other hand, should focus on undergraduate courses and in the institutional policies of each course, involving faculties as a whole. It is in the transversality of curricular development that lies the success of a continuous approach, and in doses considered appropriate to certain themes, as is that of mental health. To achieve this, commitment and involvement from the entire faculty is needed.
Despite the existence of laws that regulate training and performance of health professionals, what is determined many times is not seen in the care practice, as it is in the process of construction. The dichotomy between the propositions contained in the documents directed at training a generalist professional, able to act in all levels of care, and the implementation of these proposals in a practical way faces obstacles related to a biologist and mechanistic view of faculty and professionals regarding the services in relation to psychosocial attention.
In Brazil's case, for example, in what regards comprehensive care for those with mental disorders, the changes advocated by the National Curriculum Guidelines, the Family Health Strategy and the Psychosocial Care Network produce resistance to a new look at the training process and for health care users. Aspects of the biological psychiatry and psychosocial care models are also observed, with relative predominance of the former in the academic training of health professionals. This fact contributed to a practice that is more focused on disease-specific interventions than comprehensive care to psychological suffering of people with or without mental disorders(19). The documents demonstrate that the Brazilian reality is not isolated, but a reflex of a culture centered on a predominantly biomedical model in health, and in mental health across the globe.
Implications of mental health (under)financing for Human Resources
Planning, organization and financing of health systems is a complex task that requires the participation of multiple stakeholders from different administrative levels. As utmost protectors of the population's mental health, governments are primarily responsible for establishing appropriate legal, financial and service institutions to ensure that all needs are met, and mental health is promoted for the population(14).
In most countries, financial resources are inadequate to achieve the objectives of mental health policies. Plans and programs are often developed without careful consideration of what can be achieves with the resources available. Obtaining additional resources for mental health constitutes an important goal for improving services. Still, in many countries, mental heal policy planners don't exactly the budget to be directed to mental health and ignore which services are being financed(12).
In Brazil, BRL 33 million were invested in mental health in 2018, and in 2019, BRL 97 million were invested in strengthening the Psychosocial Care Network (RAPS) of the Unified Health System (SUS). There was an increase of 200% in relation to 2018(20), but considering Brazil's population which is over 212 million(21), this results in an expenditure of less than BRL 0.46 in mental health, per inhabitant, in 2019. This scenario worsens when government spending with mental health in low- and medium-income countries is compared and the result is under USD 1 per capita (it is even lower in Brazil), while high-income countries spend more than USD 80 per capita with mental health(22).
In this perspective, the mobilization of financing is necessary to expand resources. The first step to defining realistic budgets is to estimate gaps in resources before they are mobilized. Different types of cost estimates are needed for different purposes. WHO developed a costing tool to estimate coverage costs defined by a series of integrated interventions(13).
The accuracy and precision of the information is vital for service planning. Although it is not a case of defending the fact that all mental health services must be concentrated within a single mental health budget, a dispersed budget makes it difficult to rationally plan mental health services, as well as prioritize them according to existing needs(12). The increase in the total health budget would imply an increase in services and offers; however, without a change in the organizational process, this growth would lose its potential in the face of a fragmented and irrational organizational logic. The debate on forms of governance and the organization of mental health services represents an agenda to be placed on the agenda of mental health and social control policy makers. The area's own financing needs to increase its relative percentage, since demand tends to increase(23).
Furthermore, without proper access to decent services and adequate protection, individuals with mental disorders and their families face a difficult choice: paying out of pocket for treatment of varying quality and, at times, of poor quality - often cutting other expenses and investments, or liquidating family assets or savings - or going untreated. The often high and potentially catastrophic costs for families deprive them of ensuring access to the health services they need. In addition, direct out-of-pocket payments represent a regressive form of health financing - penalizing those least able to pay for care - and are an obvious channel through which impoverishment can occur or deepen(24).
Despite all the progress achieved, there are still countless important challenges, which can only be faced if it is possible to define a policy centered on the priority needs of the populations, based on the most up-to-date scientific knowledge and in line with international human rights instruments. Simultaneously, it is necessary to involve all relevant actors in the field of mental health in its implementation. In this context, efforts should be made to build a consensus, which will allow the progress already achieved based on existing legislation and on the technical-scientific recommendations of the international organizations competent in this matter to continue(25).
When promoting efforts to move towards universal health coverage for people with mental disorders, it is necessary not only to improve access to a range of effective, efficient and accessible interventions, but also to offer protection against the risk of financial difficulties for individuals and families affected by a mental disorder. Since mental disorders pose a threat to the well-being and economic viability of families, governments have a responsibility to ensure that the costs incurred with care are largely or fully paid for through appropriate financial protection mechanisms(24).
Conclusion
The evaluation of some of the WHO key documents highlights the concern with human resources, and the need for their development to promote mental health. Among the emphasized challenges, the documents reinforce the need for national leaders to know more about mental disorders and the proportion they occupy among the global burden of diseases, generating significant demands on health systems.
Among the barriers to its development, there is the absence of mental health as a priority of the public health agenda, which generates its underfunding in most countries of the globe. In this context, the documents analyzed emphasize the need for the availability of an adequate number of competent, dedicated and well-trained health professionals, and that their distribution be equitable, incorporating university training in mental health in all careers related to health. In addition to training, the specific budget for mental health emerges as an important focus of discussions to strengthen this area of health within the scope of different health systems. In short, the documents demonstrate the weaknesses of mental health services worldwide and that indirectly relate these weaknesses to the challenges experienced by the problems faced by Human Resources in this area, since many professionals do not have the appropriate training or are not attracted to this area. Thus, it is suggested that more studies be conducted to better determine why health professionals are not attracted to the area of mental health, and develop possible strategies to deal with the challenges discussed in this article.
The authors of this study interpreted the documents analyzed jointly in order to deal with possible biases in document analysis.
In addition, despite only focusing on three key documents for the training of human resources in mental health, this paper brings important contributions on the directions related to international policies on the subject within the scope of WHO.
References
1. Pan-American Health Organization. PAHO/WHO supports governments to strengthen and promote the mental health of the population [Internet]. 2016 [cited 2021 Mar 25]. Available from: https://www.paho.org/bra/index.php?option=com_content&view=article&id=5263:opas-oms-apoia-governos-no-objetivo-de-fortalecer-e-promover-a-saude-mental-da-populacao&Itemid=839 [ Links ]
2. Gama CAP, Campos RTO, Ferrer AL. Mental health and social vulnerability: the direction of treatment. Rev Latinoam Psicopatol Fundam. [Internet]. 2014 Mar [cited 2021 Mar 25];17(1):69-84. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-47142014000100006&lng=pt&tlng=pt [ Links ]
3. World Health Organization. Mental disorders [Internet]. 2019 [cited 2021 Mar 25]. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-disorders [ Links ]
4. Eslabão AD, Coimbra VCC, Kantorski LP, Pinho LB de, Santos EO. Mental health care network: the views of coordinators of the Family Health Strategy (FHS). Rev Gaúcha Enferm. [Internet]. 2017 [cited 2021 Mar 25];38(1). Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1983-14472017000100418&lng=pt&tlng=pt [ Links ]
5. Dal Poz MR, Lima JCS, Perazzi S. Task force on mental health in Brazil: challenges of the psychiatric reform. Physis Rev Saúde Coletiva. [Internet]. 2012 Jun [cited 2021 Mar 25];22(2):621-39. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-73312012000200012&lng=pt&tlng=pt [ Links ]
6. Zhou W, Yu Y, Yang M, Chen L, Xiao S. Policy development and challenges of global mental health: a systematic review of published studies of national-level mental health policies. BMC Psychiatry. [Internet]. 2018 Dec 18 [cited 2021 Mar 25];18(1):138. Available from: https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-018-1711-1 [ Links ]
7. Scanlan JN, Still M. Relationships between burnout, turnover intention, job satisfaction, job demands and job resources for mental health personnel in an Australian mental health service. BMC Health Serv Res. [Internet]. 2019 Dec 23 [cited 2021 Mar 25];19(1):62. Available from: https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-018-3841-z [ Links ]
8. Pereira A de A, Andrade DCL. Mental Health Educational Program for Primary Health Care Physicians. Rev Bras Educ Med. 2018 Jan;42(1):6-14. doi: https://doi.org/10.1590/1981-52712015v41n4rb20160021 [ Links ]
9. Baião JJ, Marcolan JF. Mental health policy, nursing education and difficulties in care practice. Res Soc Dev. [Internet]. 2020 Apr 28 [cited 2021 Mar 25];9(7):e85973815. Available from: https://rsdjournal.org/index.php/rsd/article/view/3815 [ Links ]
10. Wakida EK, Okello ES, Rukundo GZ, Akena D, Alele PE, Talib ZM, et al. Health system constraints in integrating mental health services into primary healthcare in rural Uganda: perspectives of primary care providers. Int J Ment Heal Syst. 2019;13:16. doi: https://dx.doi.org/10.1186/s13033-019-0272-0 [ Links ]
11. Wainberg ML, Scorza P, Shultz JM, Helpman L, Mootz JJ, Johnson KA, et al. Challenges and Opportunities in Global Mental Health: a Research-to-Practice Perspective. Curr Psychiatry Rep. [Internet]. 2017 May 19 [cited 2021 Mar 25];19(5):28. Available from: http://link.springer.com/10.1007/s11920-017-0780-z [ Links ]
12. World Health Organization. Mental health policy, plans and programmes (updated version 2) [Internet]. Geneva: WHO; 2005 [cited 2020 Dec 7]. Available from: https://www.who.int/mental_health/policy/services/2_policy plans prog_WEB_07.pdf?ua=1 [ Links ]
13. World Health Organization. mhGAP Mental Health Gap Action Programme [Internet]. Geneva: WHO; 2008 [cited 2020 Dec 7]. Available from: https://apps.who.int/iris/bitstream/handle/10665/43809/9789241596206_eng.pdf?sequence=1&isAllowed=y [ Links ]
14. World Health Organization. Mental health action plan 2013-2020 [Internet]. Geneva: WHO; 2013 [cited 2020 Dec 7]. Available from: https://apps.who.int/iris/bitstream/handle/10665/97488/9789243506029_spa.pdf?sequence=1 [ Links ]
15. Ahmed JU. Documentary Research Method: New Dimensions. Indus J Manag Soc Sci. 2010;4(1):1-14. [ Links ]
16. Cogo SB, Lunardi VL. Early Directives: a Documental Analysis in The World Context. Texto Contexto Enferm. 2018 Aug 6;27(3). doi: https://doi.org/10.1590/0104-070720180001880014 [ Links ]
17. Pessoa JM Júnior, Santos RCA, Clementino FS, Nascimento EGC, Miranda FAN. Mental health education and professional practice in the psychiatric hospital. Texto Contexto Enferm. 2016;25(3). doi: https://doi.org/10.1590/0104-07072016003020015 [ Links ]
18. Scheffer M, Cassenote A, Guilloux AGA, Miotto BA, Mainardi GM. Demografia médica no Brasil 2018. [Internet]. São Paulo, SP: FMUSP; CFM; Cremesp; 2018 [Acesso 7 dez 2020]. 286 p. Disponível em: https://jornal.usp.br/wp-content/uploads/DemografiaMedica2018.pdf [ Links ]
19. Rodrigues W, Mourão L, Almeida A, Oliveira G. Limits of theoretical-pratical mental health education in health professional training. Rev Port Enferm Saúde Mental. 2016 Oct;(spe4). doi: http://dx.doi.org/10.19131/rpesm.0149 [ Links ]
20. Investimento em Saúde Mental cresceu quase 200%. [Internet]. Governo do Brasil; 2020 [Acesso 25 mar 2021]. Disponível em: https://www.gov.br/pt-br/noticias/saude-e-vigilancia-sanitaria/2020/01/investimento-em-saude-mental-cresceu-quase-200 [ Links ]
21. Instituto Brasileiro de Geografia e Estatística. Números do Censo 2021. [Internet]. 2021 [Acesso 25 mar 2021]. Disponível em: https://censo2021.ibge.gov.br/sobre/numeros-do-censo.html#:~:text=Veja%2Caseguir%2Calgumasinformações,aseremvisitados%2C5570municípios. [ Links ]
22. Organização Pan-Americana de Saúde. Mental health: it is necessary to increase resources worldwide to reach global goals [Internet]. 2018 [cited 2021 Mar 25]. Available from: https://www.paho.org/bra/index.php?option=com_content&view=article&id=5694:saude-mental-e-necessario-aumentar-recursos-em-todo-o-mundo-para-atingir-metas-globais&Itemid=839 [ Links ]
23. Trapé TL, Campos RO. The mental health care model in Brazil: analyses of the funding, governance processes, and mechanisms of assessment. Rev Saude Pública. 2017;51. doi: https://doi.org/10.1590/s1518-8787.2017051006059 [ Links ]
24. Chisholm D, Docrat S, Abdulmalik J, Alem A, Gureje O, Gurung D, et al. Mental health financing challenges, opportunities and strategies in low- and middle-income countries: findings from the Emerald project. [Internet]. BJPsych Open. 2019 Aug [cited 2021 Mar 25];5(5):e68. Available from: https://www.cambridge.org/core/product/identifier/S2056472419000243/type/journal_article [ Links ]
25. Almeida JMC. Mental health policy in Brazil: what's at stake in the changes currently under way. Cad Saúde Pública. [Internet]. 2019 [cited 2021 Mar 25];35(11). Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2019001300502&tlng=pt [ Links ]
 Corresponding author:
Corresponding author:
Carla Aparecida Arena Ventura
E-mail: caaventu@eerp.usp.br
Received: Feb 19th 2021
Accepted: Apr 5th 2021
Author's contribution
Study concept and design: Carla Aparecida Arena Ventura, Isabel Amelia Costa Mendes, Ana Beatriz Rizzo Zanardo, Ítalo Rodolfo Silva.
Obtaining data: Carla Aparecida Arena Ventura, Isabel Amelia Costa Mendes, Ana Beatriz Rizzo Zanardo, Ítalo Rodolfo Silva.
Data analysis and interpretation: Carla Aparecida Arena Ventura, Isabel Amelia Costa Mendes, Ana Beatriz Rizzo Zanardo, Ítalo Rodolfo Silva.
Drafting the manuscript: Carla Aparecida Arena Ventura, Isabel Amelia Costa Mendes, Ana Beatriz Rizzo Zanardo, Ítalo Rodolfo Silva.
Critical review of the manuscript as to its relevant intellectual content: Carla Aparecida Arena Ventura, Isabel Amelia Costa Mendes, Ana Beatriz Rizzo Zanardo, Ítalo Rodolfo Silva.
All authors approved the final version of the text.
Conflict of interest: the authors have declared that there is no conflict of interest.
* The publication of this article in the Thematic Series "Human Resources in Health and Nursing" is part of Activity 2.2 of Reference Term 2 of the PAHO/WHO Collaborating Centre for Nursing Research Development, Brazil.


{kind=link}
{kind=link}
{kind=link}