










Serviços Personalizados
Journal

artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores
Compartilhar

 Permalink
PermalinkRevista Brasileira de Terapias Cognitivas
versão impressa ISSN 1808-5687versão On-line ISSN 1982-3746
Rev. bras.ter. cogn. vol.11 no.1 Rio de Janeiro jun. 2015
https://doi.org/10.5935/1808-5687.20150002
RELATOS DE PESQUISAS RESEARCH REPORTS
Early maladaptive schemas in hospitalized patients for suicide attempt
Esquemas iniciais desadaptativos em pacientes internados por tentativa de suicídio
Cristina Pilla Della MéaI; Sabrina ZancanellaII; Vinícius Renato Thomé FerreiraIII; Márcia Fortes WagnerIV
IPsicóloga, Especialista em Psicoterapia Cognitivo-comportamental (UNISINOS) e Especialista em Psicologia Clínica (IMED). Mestranda em Envelhecimento Humano (UPF). Professora do Curso de Psicologia da Faculdade Meridional - IMED Passo Fundo - RS - Brasil
IIPsicóloga, Pós-graduanda em Terapia Cognitivo-comportamental
IIIPsicólogo, Doutor em Psicologia pela PUCRS. Professor do Curso de Psicologia da Faculdade Meridional - IMED
IVPsicóloga, Doutora em Psicologia PUCRS. Professora do Curso de Psicologia da Faculdade Meridional - IMED)
ABSTRACT
Suicidal behavior is an important issue for mental health, and a proper assessment of its occurrence and association with psychological factors are critical for risk monitoring and treatment. Early Maladaptive Schemas (EMS), which are long-lasting emotional and cognitive patterns originated in childhood and are repeated throughout life, may be related to this behavior. This study consisted of a quantitative research, with exploratory and correlational design, which aimed to identify EMS present in 15 patients with suicide attempt admitted to a psychiatric hospital compared to 25 people in a non-clinical sample who answered a socio-demographic questionnaire and the Young Schema Questionnaire - short version (YSQ-S2). The results showed that the clinical sample had more impairments in all EMS compared to the non-clinical sample; furthermore, defectiveness/shame, social isolation and disconnection were the EMS that showed the greatest number of strong correlations with others. Proper evaluation of these EMS may have clinical relevance in evaluating suicidal behavior.
Keywords: suicide, early maladaptive schemas, schema therapy.
RESUMO
O comportamento suicida é uma questão importante para a saúde mental, e uma adequada avaliação de sua ocorrência e dos fatores psicológicos associados é fundamental para o monitoramento de riscos e para o tratamento. Esquemas iniciais desadaptativos (EIDs), que são padrões emocionais e cognitivos duradouros originados na infância e que se repetem ao longo da vida, podem estar relacionados a esse comportamento. O presente trabalho consistiu em uma pesquisa quantitativa, com delineamento exploratório e correlacional, que teve como objetivo identificar EIDs presentes em 15 pacientes internados em hospital psiquiátrico devido a tentativa de suicídio, em comparação com 25 pessoas de uma amostra não clínica, que responderam a um questionário sociodemográfico e ao Questionário de Esquemas de Young - versão breve (YSQ-S2). Os resultados demonstraram que a amostra clínica apresentou prejuízo em todos os EIDs em comparação com a amostra não clínica; além disso, os EIDs que mais apresentaram maior número de correlações fortes com outros foram Defectividade/Vergonha, Isolamento Social e Desconexão. A adequada avaliação dos EIDs, especialmente dos três citados, pode ter relevância clínica na avaliação de comportamento suicida.
Palavras-chave: suicídio, esquemas iniciais desadaptativos, terapia do esquema.
INTRODUCTION
"Suicide" etymology comes from the Greek terms sui = itself and ceades = action to kill (Corrêa & Barrero, 2006; Viana Zenkner, Sakae, & Escobar, 2008), consisting of death attempts caused by the actual victim with the voluntary intention to end his/her own life (Durkheim, 2000; Nock, Borges, Bromet, Alonso et al., 2008). Suicidal ideation can be defined as images, thoughts or fantasies that can lead someone to kill him/herself (American Psychiatric Association [APA], 2014; Chehil & Kutcher, 2012). Suicide attempt and consummated suicide have the same features, differing only by their results (Bertolote, Mello-Santos, & Botega, 2010).
Suicide is considered a serious public health problem (Brasil, 2006; Chehil & Kutcher, 2012; Gvion & Apter, 2012; World Health Organization [WHO], 2014). More than 800,000 people every year commit suicide worldwide, corresponding to 1.4% of the total amount of deaths due to diseases and represent an overall rate of 11.4 people per 100,000 (WHO, 2014). Suicide is also responsible for about half of violent deaths in the world (Chehil & Kutcher, 2012). It is estimated that in 2020 suicide rates will reach 2.4% (Brasil, 2006) and it is estimated that about 1.53 million people will die by suicide (WHO, 2014; Nock, Borges, Bromet, Cha et al., 2008). In Brazil, suicide mortality rates in the last two decades were between 3.5 and 4.6 deaths for 100,000 inhabitants. The Brazilian southern region has one of the highest suicide and attempt rates, reaching 14 suicides per 100,000 for males and between 3.2 and 4.7 deaths per 100,000 for females; it is possible to find suicide rates in this region of 21.42 per 100,000 inhabitants (Barros, Oliveira, & Marín-Léon, 2004; Ferreira & Trichês, 2014).
Related risks with suicide behavior includes loss of close people, breaking relationships, history of suicide attempts, poverty, genetic predispositions, suicide family history, substance use, sexual or physical abuse in childhood, and social withdrawal. Access to firearms, pesticides and medications, disabling diseases, and the presence of mental disorders such as depression, bipolar affective disorder and schizophrenia, may also be associated with suicide behavior (Bertolote et al, 2010;Brasil, 2006; Gvion & Apter, 2012; Large, Smith, Sharma, Nielssen, & Sing, 2011; Wenzel, Brown, & Beck, 2010; Werlang & Botega, 2004). Proper treatment of suicidal behavior includes psychological interventions and psychiatric hospitalization if necessary, since handling requires several therapeutic approaches (Botega & Werlang, 2004).
Several psychological factors are taken into account in the assessment and treatment of suicidal behavior. Jeffrey Young has developed a therapeutic strategy called Schema Therapy (ST) in order to help patients with chronic order conditions such as personality disorders, addiction, and patients with suicidal behavior. ST emphasizes a deeper level of cognition called Early Maladaptive Schemas (EMS) that are understood as lasting cognitive and emotional patterns originated in childhood and are repeated throughout life (Martin & Young, 2010; Young, 2003; Young, Klosko, & Weishaar, 2008). The EMS are formed by unconditional beliefs of individuals about themselves and the environment they live in, involving emotions, memories and bodily sensations that can become significantly dysfunctional. EMS are structures not easily changed generating clinically significant distress. Most schemas are caused by continuous patterns of preliminary experiments closely related with relatives and significant people (Martin & Young, 2010; Young et al., 2008).
YSQ has 15 EMS distributed into five domains (Young, 2003; Young et al., 2008). In the Brazilian version, these domains are Disconnection and Rejection, Restricted Autonomy and Performance, Reduced Limits, Targeting to the Other, and Hyper vigilance and Inhibition, and they aim to assess different dimensions in EMS. In the first domain, Disconnection and Rejection, people are not able to establish safe and satisfactory relationships, being characterized by traumatic childhood experiences that hinder the establishment of interpersonal relationships; EMS related to this domain are emotional deprivation, abandonment, mistrust/abuse, social isolation and defectiveness/shame. In the second domain, Restricted Autonomy and Performance, individuals have difficulty in relationship with others; EMS in this domain are failure, dependence/incompetence, vulnerability to harm, and illness and enmeshment. Reduced Limits is the third domain, associated with difficulty in establishing interpersonal limits and manage permissive environments; the two EMS for reduced limits are entitlement and insufficient self-control/ self-discipline. The fourth domain is Targeting to the Other; it shows a tendency to excessively satisfy needs of others over their own, showing a strong need for approval and difficulties in dealing with rejection; subjugation and self-sacrifice are the EMS of this domain. Finally, Hypervigilance and Inhibition is the fifth domain, covering excessive inhibition of feelings which can hamper the establishment of intimate interpersonal relationships; emotional inhibition and unrelenting standards are the EMS for this domain (Cazassa & Oliveira, 2012). The Brazilian YSQ version has found two more EMS, which are insufficient selfcriticism and disconnection (Cazassa, 2007), not related to the English version's domains.
All EMS are reinforced by feelings, thoughts and behavior, favoring the perpetuation of symptomatic behaviors (Young et al., 2008). Maintaining EMS is related to three basic mechanisms: cognitive distortions, the self-defeating life patterns and coping styles. Cognitive distortions difficult the proper environment adaptation and thus individuals erroneously perceive events, enhancing the schema (Beck, 2013). Self-defeating patterns are closely linked to harmful behaviors that the individual chooses, causing a destructive feedback. Regarding coping styles, it can be said that are maladaptive responses to avoid contact with strong emotions caused by the schemas (Rafaeli, Bernstein, & Young, 2011; Young, 2003; Young et al, 2008).
This study aimed to identify whether patients admitted to a psychiatric hospital for suicide attempt have more EMS comparing with a non-clinical sample, and if there are differences which EMS are most affected.
METHOD
The research was quantitative with a quasi-experimental design, including a clinical sample of 15 patients admitted for attempted suicide in a psychiatric hospital and a comparison sample with 25 people from the general population, characterizing the non-clinical group. The clinical group inclusion criteria were of patients over 18, men and women, admitted to the psychiatric institution for suicide attempt, and the criteria for excluding patients who had no educational, physical and/or psychological conditions for answering the surveys. This sample was non-randomic, comprised by invitation to patients who have shown interest in participating in the study and contemplate the criteria described above. For the constitution of the non-clinical group, results of Young Schema Questionnaire short version (YSQ-S2) (Cazassa, 2007) form a previous research with general population were used. The instruments applied were a socio-demographic questionnaire, prepared in order to know gender, age, education, marital status, suicide attempts, among other relevant information, and YSQ-S2, which has 75 items on a Likert scale of 6 points to evaluate 17 early maladaptive schemas (EMS) grouped into 5 domains, validated for the Brazilian population (Cazassa, 2007; Cazassa & Oliveira, 2012).
The research followed ethical Brazilian procedures, being approved by the Ethics Research Committee, and followed the National Health Council Resolution 466/12 (CAAE 31609914.9.00005319). The researches contacted the psychiatric hospital psychology department to allow the development of the survey. After that, a proper room was provided for the study, where the questionnaires were applied. In the first contact with patients were explained the main research objectives and explained the research informed consent term (TCLE) to those patients who met the inclusion criteria and presented no exclusion criteria. After that, they answered the forms and YSQ-S2. Patients responded to the survey instruments a day or two before leaving the hospital, and possibly there were little impairment of responses due to a confusion of frame by use of medications.
RESULTS
The clinical sample was mainly composed by female patients (n = 10, 66.67%) with a mean age of 41.27 years (SD 7.37), main with incomplete elementary school education (n = 7, 46.67%), married (n = 6, 40%) and with offspring (n = 11, 73.33%). Almost all of that were not working (n = 13, 86.67%) and were mostly living with the nuclear family (n = 6, 40%). The average number of suicide attempts was 7.27 (SD 5.99). The non-clinical sample was constituted mainly of females (n=15, 60%) with a mean age of 32.64 years (SD = 8), predominant with concluded high school (n = 17, 68%), married (n = 11, 44%) and working (n = 23, 92%). Offspring have not been evaluated in this sample as this information was not included in the original database.
Suicide attempts in clinical sample occurred mainly using weapon (n = 12, 34.29%) and drugs (n = 11, 31.43%), summing 65.72% of attempts. Other forms include threw (n=5, 14.29%), hanging (n = 4, 11.43%), firearm, fire, and swallowing of glass (each n = 1, 2.86%). The diagnosis presented by the patients included comorbidities: mood disorders (n = 11, 55%), substance abuse (n = 4, 20%), personality disorder (n = 1, 5%), and schizophrenia (n = 1, 5%). Most patients reported having or having had psychological care (n = 13, 86.67%).
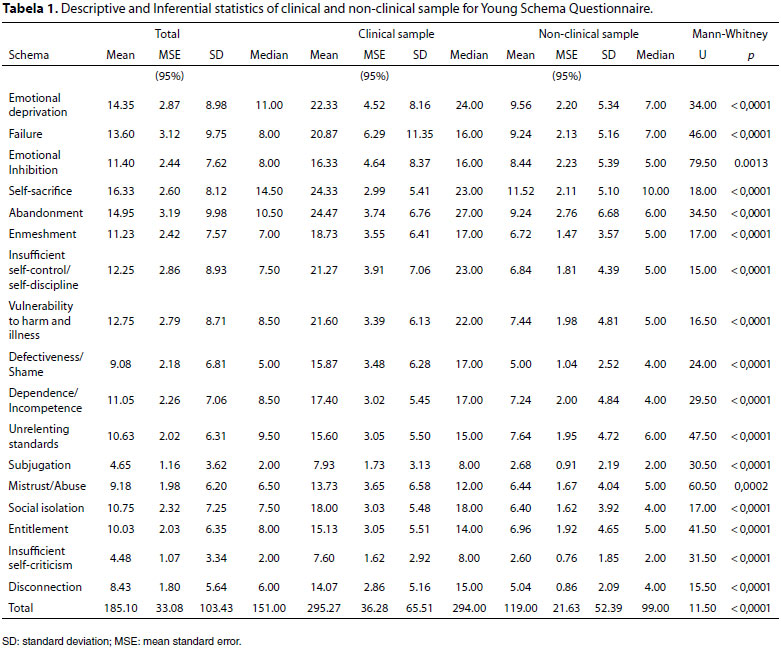
Comparing clinical and non-clinical sample showed more prejudice in all 17 EMS using Mann-Whitney test, considering the small sample size, the existence of an ordinal scale and the absence of normal distribution for YSQ-S2 (Dancey & Reidy, 2013). All differences found showed significance levels p < 0.05; higher p values were found in EMS emotional inhibition (p = 0.0013) and mistrust/abuse (p = 0.0002), but clearly lower than 0.05; other EMS showed p-values < 0.0001 considering the onetailed hypothesis, namely that the clinical sample would present greater impairments in EMS than non-clinical sample (Table 1).
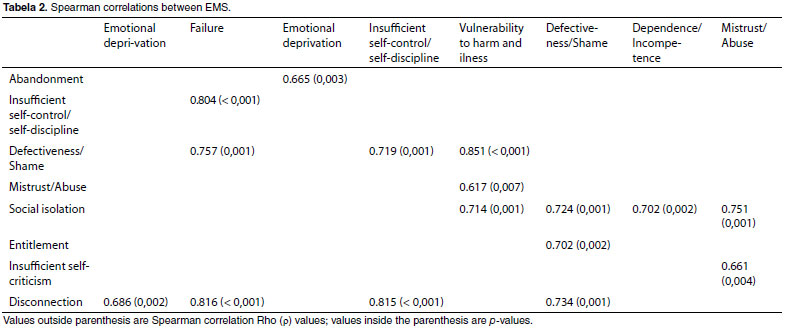
The EMS scores from the clinical sample were correlated by Spearman test (Rho, ρ) (Dancey & Reidy, 2013). Rho values equal or over 0.6 (ρ > 0.6) indicating moderate to strong correlations were highlighted, summing 16 of 153 possible combinations between EMS (Table 2). It was identified that which had more correlated EMS were defectiveness/shame (6 correlations), social isolation and disconnection (4 correlations each).
DISCUSSION
The results showed higher frequency of women in the clinical sample, with mean age of 41.27 years, matching with similar studies (Ferreira & Trichês, 2014). It is expected that more women try suicide than men, and usually men are more effective in obtaining result (Ferreira & Trichês, 2014; WHO, 2014). The ages of clinical sample with suicide attempts in this research ranged from 32 to 58 years, agreeing with other epidemiological studies that showed ages between 20 to 39 years (Souza et al., 2011) and 25 to 35 years (Macente, Santos, & Zandonade, 2009) as the most common ages for suicide attempts.
The prevailing school level was of incomplete elementary school, married with children, living with nuclear family, and unemployed. These data agree with another study that found the majority of individuals who attempted suicide were married (n = 75, 45.73%) and had basic schooling (n = 34, 45.73%) (Ferreira & Triches, 2014); furthermore, statistics show that unemployment is associated with risk of suicide (Cataldo Neto, Gauer, & Furtado, 2003; Qin, Agerbo, & Mortensen, 2003; B. J. Sadock & Sadock, 2007).
Regarding the suicide attempts, the most frequent methods were weapons and use of drugs/poisoning, matching with other studies (Ferreira & Trichês, 2014; Almeida, Guedes, Nogueira, França, & Silva, 2009; Meneghel, Victora, Faria, Carvalho, & Falk, 2004). Suicide attempt strategies are influenced by the occasion (Värnik et al., 2011). The method used to attempt suicide also involves cultural factors, and in Rio Grande do Sul, hanging is the cause of 60% of suicides (Ferreira & Trichês, 2014).
The presence of mental disorders was identified in all participants (100%); substance abuse and mood disorders were the most common comorbidity. The presence of mental disorder is considered a risk factor for new suicide attempts (Brasil, 2006; Gvion & Apter, 2012; Large et al., 2011). Approximately 90% of cases of suicide attempt satisfy diagnostic criteria for mental disorders, especially for major depressive disorder and substance use (Gvion & Apter, 2012). The presence of depressive symptoms and hopelessness can raise the risk of suicide, especially in hospitalized patients (Beck, Kovacs, & Weissman, 1975; Beck, Steer, Kovacs, & Garrison, 1985; Wenzel et al., 2010). Patients with suicidal behavior tend to express negative beliefs about themselves, about the world and about the future; while such beliefs are not only these patients; some research showed that they have more dysfunctional attitudes than other psychiatric patients. Hospitalized suicidal patients have a higher number of dysfunctional attitudes than others without suicidal behavior (Ellis & Ratliff, 1986).
Clinical sample showed a higher number of searches for psychological care, considering the low number of people with suicide attempt that search for psychotherapy (Botega & Werlang, 2004). Psychologists play an important role in cases involving suicide attempts, helping the patient, the family and the multidisciplinary staff in a hospital setting. Before discharge, referral for psychotherapy is necessary (Botega, Rapeli & Casi, 2006; Toro, Nucci, Toledo, Oliveira, & Prebianchi, 2013). It is necessary to assess the degree of lethality, psychological distress, and seek motives that will help patients stay alive (Fukumitsu, 2014).
Comparing the performance of the clinical and non-clinical sample by the YSQ-S2, the presence of statistically significant difference was identified in all EMS favoring the non-clinical sample. The occurrence of impairments has been identified in EMS in patients with mental disorders and suicidal behavior, and more risk factors improve the chances of being involved in a suicidal behavior (Hawke & Provencher, 2012; Wenzel et al., 2010). It is important to consider that in the past, EMS may have been useful and functional, but in adulthood they become dysfunctional and may be associated to suffering and suicide behaviors (Young, 2003; Wenzel et al., 2010). Suicide attempt is a dysfunctional strategy of coping with life problems, and people with EMS may find a maladaptive way of dealing with the issues involved and especially with the emotional needs. Dysfunctional schemes result from a distorted processing of information in which the cognitions experienced in a situation are determined by previous experiences, by stressful events and the occurrence of a psychiatric disorder (Wenzel et al., 2010), and these schema may lead to a suicidal behavior.
The most frequent EMS correlations were found in defectiveness/shame, social isolation, and disconnection, which may be indicators of increased risk of suicide. These findings may help to assess the clinical potential of suicide risk; it was already found that these three EMS are present in patients with repetitive suicide behaviors (Dale, Power, Kane, Stewart, & Murray, 2010). Defectiveness/shame involves inferiority beliefs, being a bad person, faulty and not desired, and therefore the person is not worthy to receive love; they may have an increased sensitivity to criticism, feeling rejected and accuse others, and involves a sense of shame related to perceived defects; in suicide, these symptoms may lead to a conclusion that the person does not deserve to keep alive. Social isolation scheme is characterized by the feeling of being different and cannot fit in a broader context outside the family, and it is a risk factor for suicidal behavior, and can reinforce the conclusion that no one may miss him or her, and therefore suicide is not a bad thing at all (Bertolote et al., 2010; Young et al., 2008). Finally, disconnection is related to an insecure, unstable environment, with little empathy and criticism. Positive feelings and acceptation are less common in these experiences, leading someone to insecure and unstable behavior patterns (Young et al., 2008).
CONCLUSION
The study allowed identifying evidences between EMS and the risk of suicide. Schemes that showed more losses in the clinical sample were defectiveness/shame, social isolation, and disconnection, indicating a possible association between behavior patterns originated in childhood and the increased risk of suicide.
It is possible to point out that the size of the clinical sample was a factor that must be considered as one of the limitations of this study, and further investigations with a broader sample may confirm or not these relationships. In the same way, we suggest that a better link between suicide behavior and comorbidity may shed light over these relationships; it is possible that these comorbidities may produce bias over the EMS and suicidal behavior.
It is clear that the presence of EMS is not the only cause associated with suicidal behavior, but it is important to take into account their presence when treating patients who have already made suicide attempts. The clinical impairments identified in EMS defectiveness/shame, social isolation, and disconnection, can be alerted for possible elements of suicidal ideation using YSQ-S2, which may be useful in the clinical evaluation process.
REFERENCES
Almeida, S. A., Guedes, P. M. M., Nogueira, J. A., França, U. M., & Silva, A. C. O. (2009). Investigação de risco para tentativa de suicídio em hospital de João Pessoa - PB. Revista Eletrônica de Enfermagem, 11(2),383-389. [ Links ]
American Psychiatric Association (APA). (2014). Manual diagnóstico e estatístico de transtornos mentais: DSM-V (5. ed.). Porto Alegre: Artmed. [ Links ]
Barros, M. B. A., Oliveira, H. B., & Marín-León, L. (2004). Epidemiologia no Brasil. In B. G. Werlang, & N. J. Botega (Eds.), Comportamento suicida (pp. 45-57). Porto Alegre: Artmed. [ Links ]
Beck, A. T., Kovacs, M., & Weissman, A. (1975). Hopelessness and suicidal behavior: An overview. Journal of the American Medical Association, 234(11),1146-1149. DOI: http://dx.doi.org/10.1001/jama.1975.03260240050026 [ Links ]
Beck, A. T., Steer, R. A., Kovacs, M., & Garrison, B. (1985). Hopelessness and eventual suicide: A 10-year prospective study of patients hospitalized with suicidal ideation. The American Journal of Psychiatry, 142(5),559-563. DOI: http://dx.doi.org/10.1176/ajp.142.5.559 [ Links ]
Beck, J. S. (2013). Terapia cognitivo-comportamental: Teoria e prática (2. ed.). Porto Alegre: Artmed. [ Links ]
Bertolote, J. M., Mello-Santos, C., & Botega, N. J. (2010). Detecção do risco de suicídio nos serviços de emergência psiquiátrica. Revista Brasileira de Psiquiatria, 32(2),87-95. DOI: http://dx.doi.org/10.1590/S1516-44462010000600005 [ Links ]
Botega, N. J., Rapeli, C. B. & Casi, C. F. S. (2006). Comportamento suicida. In N. J. Botega (Ed.). Prática psiquiátrica no hospital geral: Interconsulta e emergência (pp. 430-481). Porto Alegre: Artmed. [ Links ]
Botega, N. J., & Werlang, B. S. G. (2004). Avaliação e manejo do paciente. In B. S. G., Werlang & N. J. Botega (Eds.), Comportamento suicida (pp. 123-139). Porto Alegre: Artmed. [ Links ]
Brasil. Ministério da Saúde. (2006). Prevenção do suicídio: Manual dirigido a profissionais das equipes de saúde mental. Brasília: Ministério da Saúde. Recuperado de http://www.cvv.org.br/downloads/manual_prevencao_suicidio_profissionais_saude.pdf [ Links ]
Cataldo Neto, A. N., Gauer, C. G. J., & Furtado, N. R. (2003). Psiquiatria para estudantes de medicina. Porto Alegre: EDIPUCRS. [ Links ]
Cazassa, M. J. (2007). Mapeamento de esquemas cognitivos: Validação da versão brasileira do Young Schema Questionnaire - Short Form (Dissertação de mestrado, Pontifícia Universidade Católica do Rio Grande do Sul). Recuperado de http://tede.pucrs.br/tde_arquivos/20/TDE-2007-10-25T175537Z-900/Publico/395990 [ Links ]
Cazassa, M. J., & Oliveira, M. S. (2012). Validação brasileira do questionário de esquemas de Young: Forma breve. Estudos de Psicologia (Campinas), 29(1),23-31. DOI: http://dx.doi.org/10.1590/S0103-166X2012000100003 [ Links ]
Chehil, S., & Kutcher, S. P. (2012). Suicide risk management: A manual for health professionals. Oxford: John Wiley & Sons. [ Links ]
Corrêa, H., & Barrero, S. P. (2006). Suicídio: Uma morte evitável. São Paulo: Atheneu. [ Links ]
Dale, R., Power, K., Kane, S., Stewart, A. M., & Murray, L. (2010). The role of parental bonding and early maladaptive schemas in the risk of suicidal behavior repetition. Archives of Suicide Research, 14(4),311-328. DOI: http://dx.doi.org/10.1080/13811118.2010.524066 [ Links ]
Dancey, C. P., & Reidy, J. (2013). Estatística sem matemática para psicologia (5. ed.). Porto Alegre: Penso. [ Links ]
Durkheim, E. (2000). O suicídio: Estudo de sociologia. São Paulo: Martins Fontes. [ Links ]
Ellis, T. E., & Ratliff, K. G. (1986). Cognitive characteristics of suicidal and nonsuicidal psychiatric inpatients. Cognitive Therapy and Research, 10(6),625-634. DOI: http://dx.doi.org/10.1007/BF01173750 [ Links ]
Ferreira, V. R. T., & Trichês, V. J. S. (2014). Epidemiological profile of suicide attempts and deaths in a southern Brazilian city. Psico, 45(2),219-227. [ Links ]
Fukumitsu, K. O. (2014). O psicoterapeuta diante do comportamento suicida. Psicologia USP, 25(3),270-275. DOI: http://dx.doi.org/10.1590/0103-6564D20140001 [ Links ]
Gvion, Y., & Apter, A. (2012). Suicide and suicidal behavior. Public Health Reviews, 34(2),1-20. Recuperado de: http://www.publichealthreviews.eu/upload/pdf_files/12/00_Gvion.pdf [ Links ]
Hawke, L. D., & Provencher, M. D. (2012). Early maladaptive schemas among patients diagnosed with bipolar disorder. Journal of Affective Disorders, 136(3),803-811. DOI: http://dx.doi.org/10.1016/j.jad.2011.09.036 [ Links ]
Large, M., Smith, G., Sharma, S., Nielssen, O., & Sing, S. P. (2011). Systematic review and meta-analysis of the clinical factors associated with the suicide of psychiatric in-patients. Acta Psychiatrica Scandinavica, 124(1),18-29. DOI: http://dx.doi.org/10.1111/j.1600-0447.2010.01672.x [ Links ]
Martin, R., & Young, J. E. (2010). Schema therapy. In K. S. Dobson (Ed.), Handbook of cognitive-behavioral therapies (pp. 317-346). London: The Guilford Press. [ Links ]
Macente, L. B., Santos, E. G., & Zandonade, E. (2009). Tentativas de suicídio e suicídio em município de cultura pomerana no interior do estado do Espírito Santo. Jornal Brasileiro de Psiquiatria, 58(4),238-244. DOI: http://dx.doi.org/10.1590/S0047-20852009000400004 [ Links ]
Meneghel, S. N., Victora, C. G., Faria, N. M. X., Carvalho, L. A., & Falk, J. W. (2004). Características epidemiológicas do suicídio no Rio Grande do Sul. Revista de Saúde Pública, 38(6),804-810. DOI: http://dx.doi.org/10.1590/S0034-89102004000600008 [ Links ]
Nock, M. K., Borges, G., Bromet, E. J., Alonso, J., Angermeyer, M., Beautrais, A., Williams, D. (2008). Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. The British Journal of Psychiatry, 192(2),98-105. DOI: http://dx.doi.org/10.1192/bjp.bp.107.040113 [ Links ]
Nock, M. K., Borges, G., Bromet, E. J., Cha, C. B., Kessler, R. C., & Lee, S. (2008). Suicide and suicidal behavior. Epidemiologic Reviews, 30(1),133-154. DOI: http://dx.doi.org/10.1093/epirev/mxn002 [ Links ]
Qin, P., Agerbo, E., & Mortensen, P. B. (2003). Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: A national register-based study of all suicides in Denmark, 1981-1997. The American Journal of Psychiatry, 160(4),765-772. DOI: http://dx.doi.org/10.1176/appi.ajp.160.4.765 [ Links ]
Rafaeli, E., Bernstein, D. P., & Young, J. (2011). Schema therapy: Distinctive features. New York: Routledge. [ Links ]
Sadock, B. J., & Sadock, V. A. (2007). Compêndio de psiquiatria (9. ed.). Porto Alegre: Artmed. [ Links ]
Souza, V. S., Alves, M. S., Silva, L. A., Lino, D. C. S. F., Nery, A. A., & Casotti, C. A. (2011). Tentativas de suicídio e mortalidade por suicídio em um município no interior da Bahia. Jornal Brasileiro de Psiquiatria, 60(4),294-300. [ Links ]
Toro, G.V. R., Nucci, N. A. G., Toledo, T. B. Oliveira, A. E. G., & Prebianchi, H. B. (2013). O desejo de partir: Um estudo a respeito da tentativa de suicídio. Psicologia em Revista, 19(3),407-421. [ Links ]
Värnik, A., Sisask, M., Värnik, P., Wu, J., Kõlves, K., Arensman, E., ...Hegerl, U. (2011). Drug suicide: A sex-equal cause of death in 16 European countries. BioMed Central Public Health, 11(1),61-68. DOI: http://dx.doi.org/10.1186/1471-2458-11-61 [ Links ]
Viana, G. N., Zenkner, F. M., Sakae, T. M., & Escobar, B. T. (2008). Prevalência de suicídio no Sul do Brasil, 2001-2005. Jornal Brasileiro de Psiquiatria, 57(1),38-43. DOI: http://dx.doi.org/10.1590/S0047-20852008000100008 [ Links ]
Wenzel, A., Brown, G. K., & Beck, A. T. (2010). Terapia cognitivo-comportamental para pacientes suicidas. Porto Alegre: Artmed. [ Links ]
Werlang, B. G., & Botega, N. J. (2004). Comportamento suicida. Porto Alegre: Artmed. [ Links ]
World Health Organization (WHO). (2014). Preventing suicide: A global imperative. Recuperado de http://www.who.int/mental_health/suicideprevention/exe_summary_english.pdf?ua=1 [ Links ]
Young, J. E. (2003). Terapia cognitiva para transtornos da personalidade: Uma abordagem focada em esquemas. Porto Alegre: Artmed. [ Links ]
Young, J. E., Klosko, J. S., & Weishaar, M. E. (2008). Terapia do esquema: Guia de técnicas cognitivo-comportamentais inovadoras. Porto Alegre: Artmed. [ Links ]
 Correspondência:
Correspondência:
Cristina Pilla Della Méa
Instituição: Faculdade Meridional - IMED
Rua Senador Pinheiro, 304 , Vila Rodrigues
Passo Fundo - RS. CEP: 99070-220
E-mail: cristina.mea@imed.edu.br
Este artigo foi submetido no SGP (Sistema de Gestão de Publicações) da RBTC em 26 de Dezembro de 2014. cod. 324.
Artigo aceito em 14 de junho de 2016.


{kind=link}
{kind=link}