










Services on Demand
article
 text in
text in  Portuguese (pdf)
Portuguese (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Share

 Permalink
PermalinkRevista Brasileira de Terapias Cognitivas
Print version ISSN 1808-5687On-line version ISSN 1982-3746
Rev. bras.ter. cogn. vol.17 no.2 Rio de Janeiro July/Dec. 2021
http://dx.doi.org/10.5935/1808-5687.20210022
SYSTEMATIC REVIEW
Internet Cognitive Behavioral Therapy for Social Anxiety Disorder: a systematic review
Maria José Nunes GadelhaI; Lucas Rafael Medeiros da SilvaII; Anna Paola de OliveiraI; Natalie Aguiar CavalcanteII; Vanda Silva de AraújoI; Rodrigo Teixeira LopesIII; Neuciane Gomes da SilvaII
IUniversidade Federal do Rio Grande do Norte, Faculdade de Ciências da Saúde do Trairi - Santa Cruz - Rio Grande do Norte - Brasil
IIUniversidade Federal do Rio Grande do Norte, Departamento de Psicologia - Natal - Rio Grande do Norte - Brasil
IIIUniversity of Bern, Department of Clinical Psychology and Psychotherapy - Berna - Cantão de Berna - Suíça
ABSTRACT
Internet-based Cognitive-behavioral Therapy (iCBT) has been used to treat several mental disorders, among them Social Anxiety Disorder (SAD). The present study aimed to investigate empirical studies involving internet-based cognitive-behavioral interventions for the treatment of SAD, provided they were conducted partially or entirely in synchronous format. A systematic review was conducted between May and June 2021 in PubMed, PsycINFO, and Web of Science. The combination of keywords used were (1) "internet-based" OR "internet-delivered" OR "online" OR "telepsychology" AND "cognitive behavioral therapy" OR "cognitive therapy" AND "social phobia" OR "social anxiety disorder"; and (2) "iCBT" AND "social phobia" OR "social anxiety disorder". Four papers were selected. These studies presented synchronous interventions by videoconference and aimed to test its efficacy for treating SAD over the Internet. Results show that psychoeducation and exposure techniques are well suited in the online format. There is evidence that treatment of individuals with SAD is effective and feasible, resulting in symptom reduction or remission and improved quality of life. Still, further research is needed to consolidate the evidence of synchronous Internet-based treatment for SAD.
HEADINGS: Videoconferencing. Cognitive Behavioral Therapy. Telepsychology. Phobia, Social. Systematic Review
INTRODUCTION
The format of psychotherapy through information and communication technologies has been the subject of research in recent years, having received different denominations over time, such as telepsychology (McCord et al., 2020; Pierce et al., 2020), internet-based therapy (Alaoui et al., 2015), internet-delivered treatment (Andrews et al., 2014), online therapy (Bittencourt et al., 2020; Westerhof et al., 2019), videoconference psychotherapy (Cheli et al., 2020; Cipolletta & Mocellin, 2017), among others. Overall, these models can be classified as synchronous online psychotherapies and asynchronous online psychotherapies. In the first model, interventions are usually performed by videoconference, in real-time, when the patient and the therapist maintain verbal or nonverbal communication, either by audio, video, or data, simulating face-to- face care. In turn, asynchronous or self-guided interventions are performed through prescriptive online programs, hosted on websites, and consumed by people who want mental health-related assistance (Lopes et al., 2020).
The pandemic of COVID-19 gave even more importance to the format of synchronous psychotherapy since it drove public and private institutions and private practices to adapt their practices, causing therapies previously performed in the face-to- face format to be performed remotely through videoconferencing, thus favoring isolation. In this sense, although under the imposition of the pandemic, this necessary adaptation also predicts positive impacts in the post-pandemic period, such as the popularization of online psychological treatments and the facilitation of their access by populations previously unreached (Raony et al., 2020; Warnock-Parkes et al., 2020; Simpson et al., 2020).Of the population presenting with Social Anxiety Disorder (SAD), only half seek appropriate treatment. Randomized clinical trials show that Internet-based Cognitive- Behavioral Therapy (iCBT) interventions can be effective in treating SAD compared to not using some treatment (Berger et al., 2014; Thew et al., 2019). The primary psychological interventions used technology-assisted for SAD include guided or self- guided iCBT, virtual reality exposure, and cognitive bias modification (Kampmann et al., 2016).
Research about predominantly asynchronous SAD treatments, with therapist support via forums or email or even no contact beyond the program, is more frequent than interventions researchs that combine iCBT programs with real-time therapeutic support, or even than 100% synchronous treatments (e.g., Alaoui et al., 2015; Ivanova et al., 2016; Niles et al., 2021; Nordgreen et al., 2018; Schulz et al., 2016). Warnock-Parkes et al. (2020) propose an adaptation of Clark and Wells' (1995) protocol, used in face-to-face SAD treatment, to a 100% synchronous format with 14 sessions and a duration of three to four months. However, although Warnock-Parkes et al. (2020) do not present empirical data on the effectiveness of online SAD treatment, the authors make suggestions and recommendations to adapt the face-to-face model. The use of videoconferences prevails as an indication in this proposal, highlighting the use of programs that favor the client's connection, the choice of a place where there are no interruptions or distractions, and, finally, the request for regular feedbacks.
In meta-analysis studies, Acarturk et al. (2009) and Hofmann et al. (2008) concluded that CBT psychological treatments for SAD are effective in adults but may be less effective in more severe cases. In a recent review, Guo et al. (2020) analyzed the efficacy of CBT for SAD in an asynchronous format and found that it can significantly reduce the symptoms of the disorder, showing long-term efficacy, and that its effect, when used alone, was similar to the effect observed when combined with other therapies.
The review by Guo et al. (2020) included in its research only articles in which the treatment under study was based on computer programs, mobile phone applications, or discussion forums, and in which the therapist's feedback was provided via email, not specifying attendance protocols in a synchronous format, based on the internet, in which therapist and patient could have more direct contact. Thus, the objective of this review was to investigate empirical studies involving internet-based cognitive-behavioral interventions, individual or group, for the treatment of SAD, provided that at least one activity by videoconference was adopted, considering the publication period from 2011 to 2021.
METHOD
This systematic review was based on the Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA) model. The search was conducted online between May and June 2021 in the PubMed, PsycINFO, and Web of Science databases. The choice of databases is justified by their recognition and use in systematic literature reviews in health and psychology. The search key combinations used included: 1) "internet-based" OR "internet-delivered" OR "online" OR "telepsychology" AND "cognitive behavioral therapy" OR "cognitive therapy" AND "social phobia" OR "social anxiety disorder"; and "iCBT" AND "social phobia" OR "social anxiety disorder." The articles were selected directly from the databases or located from the references of these sources and could also be written in any language.
For the inclusion of the articles in the review, the following criteria were used: a) to be empirical studies; b) to involve cognitive-behavioral therapies; c) the subjects of the sample should have a primary diagnosis of SAD, with or without diagnosed comorbid disorders; d) at least one of the treatments used should be over the internet; e) to be a study with a group or individual intervention; f) to have at least one synchronous activity via the internet, and g) to have been published between the years 2011 and 2021.
The exclusion criteria for review articles were: a) being a review study (meta- analysis, integrative, systematic, or narrative review); b) being a theoretical essay; c) being a validation or adaptation study of a psychological instrument; d) the research subjects being children or elderly; e) the treatment being asynchronous only; f) contact with the therapist being restricted to feedback by email or text messages; and g) articles that did not evidence synchronous contact between therapist and participant.
RESULTS
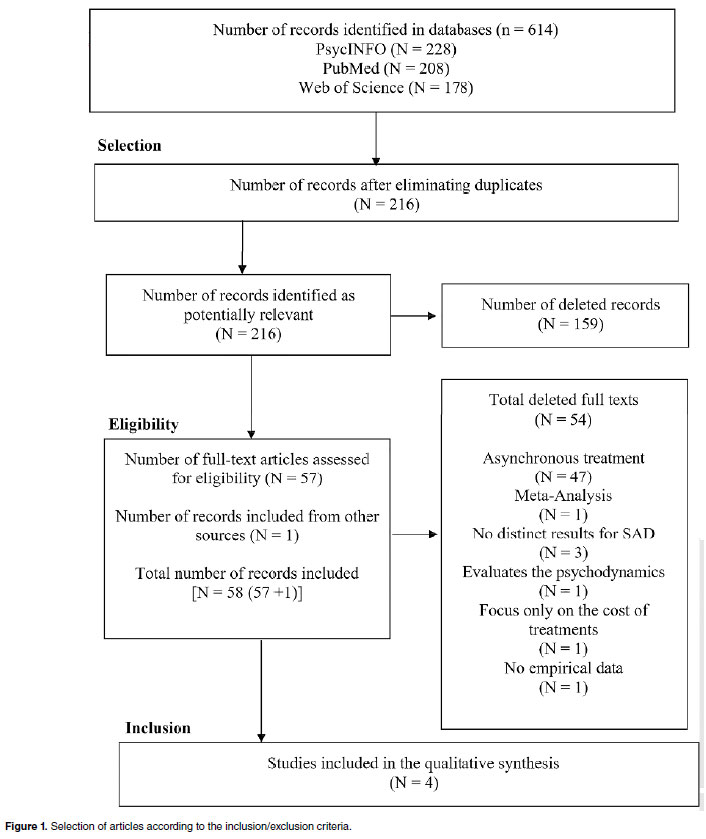
Six hundred fourteen articles were collected: 228 in PsycINFO, 208 in PubMed, and 178 in Web of Science. Subsequently, duplicate articles were excluded, leaving, in the end, 216 works. The entire procedure of analysis of the articles included in this review, from the identification phase to the final product, is shown in Figure 1.
In the identification phase, database search was performed with the previously mentioned combinations, applied to the titles and abstracts and the body of the texts. Then, in the selection phase, three of the authors of this review independently analyzed the titles and abstracts of each article, applying the exclusion and inclusion criteria. In the selection phase, 159 articles were excluded because they met the exclusion criteria, i.e., they were systematic reviews, theoretical essays, involved validation and adaptation of theoretical instruments, did not evaluate some approaches of the iCBT in a synchronous format, the subjects were children, adolescents or elderly or did not have a primary diagnosis of SAD. Thus, 57 full-text studies were selected for the eligibility phase, and one record from another source was found from the article by Matsumoto et al. (2018), which was also included in this phase, totaling 58 selected records. These were analyzed using the study selection criteria through the PRISMA statement method, and cases of doubts or divergences were discussed together.
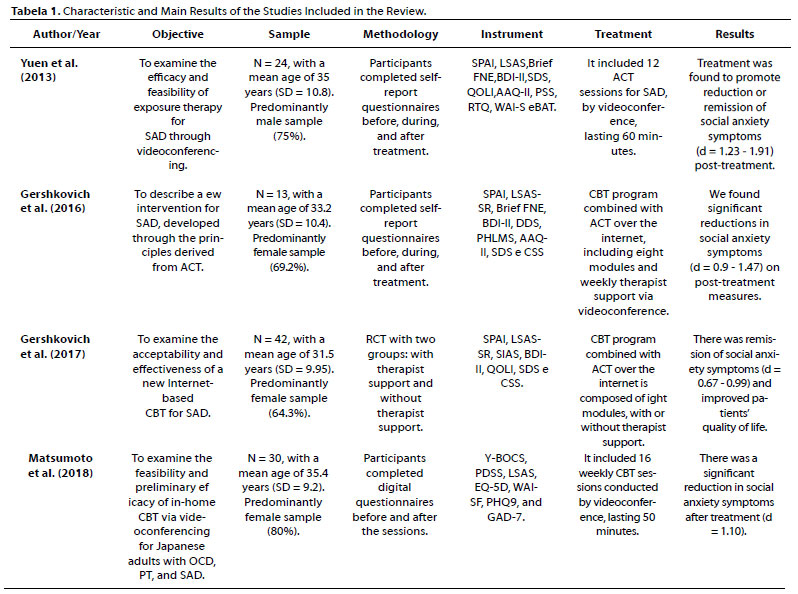
As for the justification for the exclusion of the articles, 47 papers were excluded because the contact with the therapist was established only in the asynchronous modality, and seven others were excluded for different reasons: three did not show results of the intervention in participants with SAD, one used asynchronous treatment, one was a meta- analysis, one evaluated a psychodynamic approach treatment, and another described a protocol and focused on the comparison of financial costs, neglecting the effectiveness of the treatment. In the fourth phase, four articles were included, which met all the inclusion criteria. Table 1 brings some critical data about each of them, such as the study's objective listed by the authors, the sample, the methodology applied, the instruments used, the characteristics of the treatment, and the main results of such research.
By observing Table 1, it is possible to identify the convergent and divergent points of the articles analyzed along the topics presented. The four studies had the main objective of assessing the effectiveness of the proposed interventions, with the addition of some particular aspects, such as their feasibility (Matsumoto et al., 2018; Gershkovich et al., 2016; Yuen et al., 2013) and acceptability by participants with SAD (Gershkovich et al., 2017).
In total, 109 subjects were evaluated in the four studies, with the one by Gershkovich et al. (2016) presenting the lowest number of participants (N = 13), and the one by Gershkovich et al. (2017), the highest number of participants (N = 42), both published by the same group of collaborators. Female participation was notable in three studies (Gershkovich et al., 2016; Gershkovich et al., 2017; Matsumoto et al., 2018), with the percentage ranging from 64.3% to 80%. Mean ages ranged from 31.5 to 35.4 years. Participants of two different nationalities were targeted in the intervention, Gershkovich et al. (2016), Gershkovich et al. (2017), and Yuen et al. (2013) analyzed American subjects, with Caucasians being the prevalent ethnicity (respectively, 69.2%, 66.7% and 75% of the sample). In contrast, Matsumoto et al. (2018) relied on a complete sample of Japanese.
The methodologies used involved the Randomized Clinical Trial (RCT) conducted by Gershkovich et al. (2017) and the analysis of clinical aspects of SAD before, during, and after the intervention (Gershkovich et al., 2016; Matsumoto et al., 2018; Yuen et al., 2013). The theoretical perspectives and treatments used presented an intersection between the classical and the innovative. Thus, in addition to an intervention based on traditional Cognitive-Behavioral Therapy (CBT) (Matsumoto et al., 2018), resources from third-wave cognitive-behavioral therapies are present in the experiments of Yuen et al. (2013), Gershkovich et al. (2016), and Gershkovich et al. (2017), which used elements of Acceptance and Commitment Therapy (ACT) and also mindfulness.
As for the treatment format, two studies delivered fully synchronous interventions, and two other studies delivered a combination of synchronous and asynchronous interventions. In the first two cases, videoconferencing and real-time communication between the therapist and the patient throughout the session were the variables in evidence (Matsumoto et al., 2018; Yuen et al., 2013). In the last two studies (Gershkovich et al., 2016; Gershkovich et al., 2017), the authors adapted a face-to-face ACT protocol to an electronic interface located on a website, emphasizing the role of narrated audios, video clips, reading materials, and restricting contact with the therapist to 15-20 minutes (Gershkovich et al., 2016) or 10-15 minutes (Gershkovich et al., 2017).
In this context, in the first study analyzed in this review, Yuen et al. (2013) sought to verify the effectiveness and feasibility of ACT for subjects who met the primary diagnosis of SAD, according to the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM - IV). In this sense, the intervention consisted of 12 psychotherapy sessions, lasting one hour, via skype, counting on the conduct of doctoral students in clinical psychology. Patients should perform homework assignments to continue what had been worked in each session, involving real-life social situations, and complete monitoring forms at the sessions' beginning, middle, and end (Yuen et al., 2013).
Yuen et al. (2013) showed that a fully synchronous intervention model has many advantages, confirmed from the analysis of the results, which found large effect sizes (Cohen's d from 1.2 to 1.91) between pre-treatment and post-treatment social anxiety measures, showing lower anxiety ratings at post-treatment. Regarding treatment acceptability and feasibility, 95% of the subjects reported satisfaction with the intervention, 91% reported fear attenuation, and 95% confirmed a decrease in social skipping behaviors (Yuen et al., 2013).
The second study, by Gershkovich et al. (2016), aimed to describe a treatment intervention protocol for SAD, in which they also used elements of acceptance derived from the principles of ACT, combined with conventional exposure techniques. In this sense, the researchers selected 13 participants who had the primary diagnosis of SAD according to DSM-IV. The treatment was available through a website with individual login and password for each participant who completed the eight module intervention protocol (Gershkovich et al., 2016).
Along with the intervention of the modules belonging to the program, participants were also entitled to one synchronous online videoconference session per week, lasting 15 to 20 minutes. This type of service aimed to perform a kind of check-in, in which empathic listening was offered and a review of homework assignments and the concepts of the week's module was conducted, in addition to assistance in exposure situations. Therefore, it should be noted that this was not a regular psychotherapy session (Gershkovich et al., 2016).
The treatment evaluation was applied before, during (after the completion of four modules), and after treatment (after the completion of the eight modules and three months after the whole treatment), through measures of social anxiety, depression, and satisfaction. The results showed that the intervention was related to reducing SAD symptoms and contributed to the attenuation of fears in social situations and their avoidance (Gershkovich et al., 2016).
Following this same perspective, in the third study described in this review, Gershkovich et al. (2017) proposed to verify the effectiveness and acceptability of the same intervention, which is composed of modules that combine ACT strategies with classical exposure (Gershkovich et al., 2016). In addition, to better evaluate the effectiveness of the intervention, the authors also sought to verify whether the support of therapists associated with the program modules is vital. To this end, an RCT consisted of two groups: 1) participants who completed the modules with therapist support via videoconference once a week; 2) participants who only completed the program without therapist support (Gershkovich et al., 2017). Forty-two volunteers were selected whose mean age was 31.5 years and whom 64.3% were female.
In addition, those participants in the group that received support from the therapist were provided with the same videoconference session protocol presented in Gershkovich et al. (2016) with a short duration. Again the research subjects were assessed before, during, and post-treatment from self-report measures of social anxiety, depression, and treatment satisfaction (Gershkovich et al., 2017). No significant changes were found between the group receiving videoconference support and the group without support, even though more significant remission of SAD symptoms was found in the group receiving synchronous support.
Unlike the previous research regarding the theoretical perspective, Matsumoto et al. (2018), the last study analyzed in this review, used traditional CBT in its protocol. However, like Yuen et al. (2013), it employed a fully synchronous intervention. The research aimed to examine the feasibility and efficacy of CBT delivered by videoconferencing in treating Obsessive-compulsive disorder (OCD), panic disorder (PT), and SAD. Thirty Japanese adults participated in the research; of these, nine had a principal diagnosis of SAD, which is the main focus of analysis in this review. The treatment consisted of weekly individual sessions, lasting 50 minutes, held in an online videoconference room, whose access link was sent by email by the therapist for 16 weeks.
Topics such as psychoeducation, exposure exercises, behavioral experiments, and homework assignments were addressed (Matsumoto et al., 2018).
The evaluations measured SAD symptoms, quality of life, the bond between therapist and participant, depressive symptoms, and satisfaction with CBT via videoconference. For this, before sessions number 1, 8, and 16, the participants answered the questionnaires on a tablet lent by the researchers and sent the answers to their therapists' email. The therapists checked the data and evaluated the symptoms with the participant's collaboration (Matsumoto et al., 2018).
Matsumoto et al. (2018) showed a significant reduction in social anxiety symptoms, with a large effect size (Cohen's d = 1.10), calculated between pre- and post- treatment. The authors pointed out that this type of intervention could be widely implemented in Japan, considering the effectiveness of the intervention and the satisfaction of 86% of the participants.
DISCUSSION
In the analyses performed from the results of the studies included in this review, it was found that, although internet psychotherapy has been widely disseminated and used for the treatment of SAD (Acarturk et al., 2009; Andrews et al., 2018; Hofmann & Smits, 2008; Kampmann et al., 2016), few studies have included synchronous interventions in their clinical protocol (Gershkovich et al., 2016; Gershkovich et al., 2017; Matsumoto et al., 2018; Yuen et al., 2013). This type of real-time care, besides being similar to face-to- face care in terms of technical procedures, has been reported as a very viable alternative for people with SAD who have accessibility difficulties regarding geographical location or even the characteristics of the disorder itself, such as emotional discomfort during the commute in public transportation or social contact during the journey to the therapist (Bittencourt et al., 2020).
Only the studies by Yuen et al. (2013) and Matsumoto et al. (2018) applied fully synchronous protocols to treat SAD. The results of these two studies were similar to those reported in Loerinc et al.'s (2015) review of face-to-face CBT in terms of acceptability and feasibility of treatment, satisfaction with the intervention, alleviation of fear, and decrease in socially eschewing behaviors. Hietanen et al. (2020) corroborate this idea by stating that it is possible to obtain the same effects in the therapeutic relationship through physical eye contact or video call. The same study compared the psychophysiological responses between groups with eye contact in a live interaction and a video call. They found that direct gaze provoked positive affective facial reactions of autonomic arousal, measured through skin conductance responses and facial reactions with electromyography. Thus, the results suggest that the physical presence or proximity of the other person is not necessary for positive psychophysiological responses to eye contact.
Gershkovich et al. (2016) combined asynchronous treatment with synchronous treatment, conducting a pilot study that included weekly synchronous sessions lasting 15- 20 minutes. This protocol was improved by Gershkovich et al. (2017) through a more robust study since, in addition to assessing aspects not addressed in the 2016 study, it used an RCT, a method considered relevant, with strict and reliable interventional and sample control criteria in the evaluation of health treatments (Reis et al., 2008).
The absence of significant differences between the social anxiety measures of the SAD group that participated in the asynchronous protocol with support and the SAD group that did not receive support, as pointed out by Gershkovich et al. (2017), reveals that the iCBT programs also have their contribution in the treatment of SAD. Thus, the authors affirm the usefulness of this treatment modality for subjects who have limitations regarding access to face-to-face appointments, as well as for individuals who are afraid to put themselves in social contexts, or even for those who prefer to participate anonymously and have schedule restrictions (Gershkovich et al., 2017). In this same direction, Hedman et al. (2011) state that asynchronous protocols can have the same effectiveness as face-to-face style CBT protocols. In turn, Berger et al. (2014) also point out that asynchronous self-guided internet treatments showed moderate to high effects compared to control groups in subjects with SAD, with long-lasting effects, found five years after treatment completion.
These data highlight efficacy results for the treatment of SAD for both fully synchronous (Yuen et al., 2013; Matsumoto et al., 2018) and mixed models (Gershkovich et al., 2017). However, a direct comparison between the studies cannot be performed since they used different methodologies and theoretical perspectives. It is possible that both third-wave theoretical models and the traditional model of CBT may be suitable for fully synchronous treatments. However, even if the theoretical perspectives and treatments used show an intersection between the classical and the innovative, a trend that is being drawn not only in the treatment of SAD but in several diagnostic categories, no studies with mixed protocols (asynchronous with synchronous support) using traditional CBT as a theoretical perspective were found.
Other differences can still be identified. For example, the four studies analyzed chose to assess symptoms and other secondary parameters before, during, and after the last session/module of the intervention, but only Gershkovich et al. (2016) and Yuen et al. (2013) added a follow-up procedure in their design. In Gershkovich et al.'s (2016) research, the maintenance of significant gains was observed after three months of the intervention. In contrast, the same type of evidence is not present in the RCT conducted one year later by the same North American researchers nor in the Japanese study, which would have the potential to confer greater validity to their findings of the effectiveness of iCBT (Gershkovich et al., 2017; Matsumoto et al., 2018).
From this perspective, given the analysis performed, it is suggested that the asynchronous modality combined with a weekly synchronous moment by videoconference (Gershkovich et al., 2016; Gershkovich et al., 2017) or simply the fully synchronous treatment by video (Matsumoto et al., 2018; Yuen et al., 2013) are more effective in the remission of SAD symptoms than synchronous treatment through other means of communication. Thus, videoconferencing is considered a more efficient tool than phone calls and text messages, as it allows verbal and nonverbal communication, enhancing the interaction between therapist and patient (Gershkovich et al., 2017; Yuen et al., 2013), as well as promoting the strengthening of the therapeutic relationship (Cipolletta et al., 2018; Matsumoto et al., 2018).
In agreement with this, Gershkovich et al. (2017) reported that patients considered video conferencing superior to text messages in terms of usefulness. In this same perspective, the majority of participants (n = 24) in Matsumoto et al.'s (2018) research preferred the videoconference synchronous care modality, while the rest of the volunteers remained neutral (n = 3) or preferred the face-to-face format (n = 2). Yuen et al. (2013) also state that 95% of those involved in the research reported easy access to skype for videoconferences. Overall, these data suggest that the treatment for SAD can be adapted to the online format, without dismissing essential techniques for the therapeutic process, such as cognitive defusion, exposure, and classical psychoeducation, and that the iCBT format of care, with at least one synchronous activity, seems to be effective for both Western and Eastern cultures.
However, even having found results that point to the effectiveness for the treatment of SAD in interventions that include synchronous meetings, the international literature still lacks scientific articles with research focused on the evaluation of the effectiveness and viability of the treatment through the psychotherapeutic process by videoconference. In this way, considering the advantages already presented by totally synchronous treatments, through videoconferencing, the need to develop clinical trials and other types of research with a large sample, which are concerned with applying this type of model for the treatment of the disorder in question, thus contributing to the consolidation and dissemination of this format of psychotherapy, is pointed out.
FINAL CONSIDERATIONS
This review aimed to estimate empirical studies involving individual or group cognitive-behavioral interventions for treating SAD synchronously over the internet. Internet psychotherapy has been studied worldwide in recent years and with greater emphasis due to the COVID-19 pandemic. From this perspective, treatment of anxiety disorders over the internet has been developed and studied because it is more accessible to the population compared to face-to-face psychotherapy, since the latter may entail more significant barriers to its implementation, whether geographical (displacement), monetary (high cost), logistical (long waiting list), or psychological (fear or shame of meeting face- to-face with a stranger, in the case of people with social anxiety).
Thus, it was possible to observe that even though the synchronous modality is still susceptible to some technical limitations, such as connection failures, this type of intervention has proven effective in treating SAD and may present efficacy similar to that of face-to-face psychotherapy. Moreover, this model has a vast implementation potential since it has been adapted not only for Western cultures but also in Eastern countries.
Regarding the limitations, this research did not include children as the target audience studied, in addition to having a small sample of articles analyzed and heterogeneity regarding the types of interventions used in the research, including both mixed-type studies, with synchronous, asynchronous interventions and synchronous interventions. These last two limitations can be explained, in large part, by the scarcity of studies related to the 100% synchronous treatment of SAD.
The high number of productions found on asynchronous treatment can be explained by the increased use or development of new technologies (computer programs and mobile phone applications). However, further research is needed to understand the real effectiveness of asynchronous programs or if the profile of socially anxious people demands treatments with fewer face-to-face meetings to detail such explanation and account for the most used treatments in this public.
REFERENCES
Acarturk, C., Cuijpers, P., van Straten, A., & de Graaf, R. (2009). Psychological treatment of social anxiety disorder: A meta-analysis. Psychological Medicine, 39(2),241-254. https://doi.org/10.1017/S0033291708003590 [ Links ]
Alaoui, S.E., Hedman, E., Kaldo, V., Hesser, H., Kraepelien, M., Andersson, Rück, C., Andersson, G., Ljótsson, B., & Lindefors, N. (2015). Effectiveness of Internet-based cognitive-behavior therapy for social anxiety disorder in clinical psychiatry. Journal of Consulting and Clinical Psychology, 83(5),902-914. https://doi.org/10.1037/a0039198 [ Links ]
Andrews, G., Newby, J.M. & Williams, A. D. (2014). Internet-Delivered Cognitive Behavior Therapy for Anxiety Disorders Is Here to Stay. Current Psychiatry Reports, 17(1),1- 5. http://doi.org/10.1007/s11920-014-0533-1 [ Links ]
Andrews, G., Basu, A., Cuijpers, P., Craske, M. G., McEvoy, P., English, C. L., & Newby, J. M. (2018). Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: An updated meta-analysis. Journal of Anxiety Disorders, 55,70-78. https://doi.org/10.1016/j.janxdis.2018.01.001 [ Links ]
Berger, T., Boettcher, J., & Caspar, F. (2014). Internet-Based Guided Self-Help for Several Anxiety Disorders: A Randomized Controlled Trial Comparing a Tailored With a Standardized Disorder-Specific Approach. Psychotherapy, 51(2),207-219. https://doi.org/10.1037/a0032527 [ Links ]
Bittencourt, H. B., Rodrigues, C. C., Santos, G. L., Silva, J. B., Quadros, L. G., Mallmann, L. S. Bratkowski, P. S., & Fedrizzi, R. I. (2020). Psicoterapia on-line: uma revisão de literatura. Diaphora, 9(1),41-46. https://doi.org/10.29327/217869.9.2-6 [ Links ]
Cheli, S., Cavalletti, V., & Petrocchi, N. (2020). An online compassion-focused crisis intervention during COVID-19 lockdown: a cases series on patients at high risk for psychosis. Psychosis, 12(4)1-4. https://doi.org/10.1080/17522439.2020.1786148 [ Links ]
Cipolletta, S., Frassoni, E., & Faccio, E. (2018). Construing a therapeutic relationship online: An analysis of videoconference sessions. Clinical Psychologist, 22(2),220-229. http://doi.org/10.1111/cp.12117/ [ Links ]
Cipolletta, S., & Mocellin, D. (2017). Online counseling: An exploratory survey of Italian psychologists' attitudes towards new ways of interaction, Psychotherapy Research, 28(6),1-16. https://doi.org/10.1080/10503307.2016.1259533 [ Links ]
Clark, D. M., & Wells, A. (1995). Cognitive model of social phobia. Em R. G. Heimberg, M.R. Liebowitz, D. A. Hope & F. R. Schneider. Social phobia: Diagnosis, assessment and treatment. (pp. 69-93). Guilford. [ Links ]
Gershkovich, M., Herbert, J.D, Forman, E, M, & Glassman, L. (2016). Guided Internet-Based Self-Help Intervention for Social Anxiety Disorder With Videoconferenced Therapist Support. Cognitive and Behavioral Practice, 23(2),239-255. https://doi.org/10.1016/j.cbpra.2015.08.005 [ Links ]
Gershkovich, M., Herbert, J. D., Forman, E. M., Schumacher, L. M., & Fischer, L. E. (2017). Internet-Delivered Acceptance-Based Cognitive-Behavioral Intervention for Social Anxiety Disorder With and Without Therapist Support: A Randomized Trial. Behavior Modification, 41(5),583-608. https://doi.org/10.1177/0145445517694457 [ Links ]
Guo, S., Deng, W., Wang, H., Liu, J., Liu1, X., Yang, X., He, C., Zhang, Q., Liu, B., Dong, X., Yang, Z., Li, Z., & Xiaoming, L. (2020). The efficacy of internet-based cognitive behavioral therapy for social anxiety disorder: A systematic review and meta-analysis. Clinical Psychology & Psychotherapy, 28(3),656-668. https://doi.org/10.1002/cpp.2528 [ Links ]
Hedman, E., Andersson, G., Ljótsson, B., Andersson, E., Rück, C., Mörtberg, E., & Lindefors, N. (2011). Internet-based cognitive behavior therapy vs. cognitive behavioral group therapy for social anxiety disorder: a randomized controlled non- inferiority trial. Plos One, 6(3),1-10. https://doi.org/10.1371/journal.pone.0018001 [ Links ]
Hietanen, J. O., Peltola, M. K., & Hietanen, J. K. (2020). Psychophysiological responses to eye contact in a live interaction and in video call. Psychophysiology, 57, 1-12. https://doi.org/10.1111/psyp.13587 [ Links ]
Hofmann, S. G., & Smits, J. A. J. (2008). Cognitive-behavioral therapy for adult anxiety disorders: A meta-analysis of randomized placebo-controlled trials. The Journal of Clinical Psychiatry, 69(4),621-632. https://doi.org/10.4088/jcp.v69n0415 [ Links ]
Ivanova, E., Lindner, P., Ly, K.H., Dahlin, M., Vernmark, K., Andersson, G., & Carlbring, P. (2016). Guided and unguided Acceptance and Commitment Therapy for social anxiety disorder and/or panic disorder provided via the Internet and a smartphone application: A randomized controlled trial. Journal of Anxiety Disorders, 44,27-35. https://doi.org/10.1016/j.janxdis.2016.09.012 [ Links ]
Kampmann, s. L., Emmelkamp, P. M.G., & Morina, N. (2016). Meta-analysis of technology- assisted interventions for social anxiety disorder. Journal of Anxiety Disorders, 42,71- 84. https://doi.org/10.1016/j.janxdis.2016.06.007 [ Links ]
Loerinc, A. G., Meuret, A. E., Twohig, M. P., Rosenfield, D., Bluett, E. J., & Craske, M. G. (2015). Response rates for CBT for anxiety disorders: Need for standardized criteria. Clinical psychology review, 42,72-82. https://doi.org/10.1016/j.cpr.2015.08.004 [ Links ]
Lopes, R.T., Svacina, M.A., & Sartes, L.A. (2020). Terapia cognitivo-comportamental mediada pela internet. Em: Federação Brasileira de Terapias Cognitivas, C. B. Neufeld, E.M. Falcone & B.P. Rangé (Orgs.), Procognitiva. Programa de Atualização em Terapia Cognitivo-Comportamental: Ciclo 7 (pp 9-55), volume 3. Artmed Panamericana (Sistema de Educação Continuada a Distância). [ Links ]
Matsumoto, K., Sutoh, C., Asano, K., Seki, Y., Urao, Y., Yokoo, M., Takanashi, R., Yoshida, T., Tanaka, M., Noguchi, R., Nagata, S., Oshiro, K., Numata, N., Hirose, M., Yoshimura, K., Nagai, K., Sato, Y., Kishimoto T, Nagawa, A., & Shimizu, E. (2018). Internet-Based Cognitive Behavioral Therapy With Real-Time Therapist Support via Videoconference for Patients With Obsessive-Compulsive Disorder, Panic Disorder, and Social Anxiety Disorder: Pilot Single-Arm Trial. Journal of medical Internet research, 20(12),1-17. https://doi.org/10.2196/12091 [ Links ]
McCord, C., Bernhard, P., Walsh, M., Rosner, C., & Console, K. (2020). A consolidated model for telepsychology practice. Journal Clinic Psychology, 76, 1060-1082. https://doi.org/10.1002/jclp.22954 [ Links ]
Niles, A.N., Axelsson, E., Andersson, E., Hedman-Lagerlöf, E., Carlbring, P., Andersson, G., Johansson, R., Widén, S., Driessen, J., Santoft, F., & Ljótsson, B. (2021). Internet- based cognitive behavior therapy for depression, social anxiety disorder, and panic disorder: Effectiveness and predictors of response in a teaching clinic. Behaviour Research and Therapy, 136, 2-12. https://doi.org/10.1016/j.brat.2020.103767 [ Links ]
Nordgreen, T., Gjestad R., Andersson, G., Carlbring, P., & Havik, O.E. (2018). The effectiveness of guided internet-based cognitive behavioral therapy for social anxiety disorder in a routine care setting. Internet Interventions, 13,24-29. https://doi.org/10.1016/j.invent.2018.05.003 [ Links ]
Pierce, B. S., Perrin, P. B. & McDonald, S. D. (2020). Demographic, Organizational, and Clinical Practice Predictors of U.S. Psychologists' Use of Telepsychology.Professional Psychology: Research and Practice, 51(2),184-193. https://doi.org/10.1037/pro0000267 [ Links ]
Raony, I., Figueiredo, C.S., Pandolfo, P., Giestal-De-Araujo, E., Bomfim, P.O., & Savino, W. (2020). Psycho-Neuroendocrine-Immune Interactions in COVID-19: Potential Impacts on Mental Health. Frontiers In Immunology, 11(1170),1-15. https://doi.org/10.3389/fimmu.2020.01170 [ Links ]
Reis, F.B., Lopes, A.D., Faloppa, L., & Ciconelli, R.M. (2008). A importância da qualidade dos estudos para a busca da melhor evidência. Revista Brasileira de Ortopedia, 43(6),210-216. https://doi.org/10.1590/S0102-36162008000600001 [ Links ]
Schulz, A., Stolz, T., Vincent, A., Krieger, T., Andersson, G. & Berger, T. (2016). A sorrow shared is a sorrow halved? A three-arm randomized controlled trial comparing internet-based clinician-guided individual versus group treatment for social anxiety disorder. Behavior Research and Therapy, 84,15-26. https://doi.org/10.1016/j.brat.2016.07.001 [ Links ]
Simpson, S., Richardson, L., Pietrabissa, G., Castelnuovo, G., & Reid, C. (2020). Videotherapy and therapeutic alliance in the age of COVID-19. Clinical Psychology & Psychotherapy, 28(2),409-421. https://doi.org/10.1002/cpp.2521 [ Links ]
Thew, G. R., Powell, C. L., Kwok, A. P., Chan, M. H. L., Wild, J., Warnock-Parkes, E., Leung, P.W.L., & Clark, D.M. (2019). Internet-Based Cognitive Therapy for Social Anxiety Disorder in Hong Kong: Therapist Training and Dissemination Case Series. Jmir Formative Research, 3(2),1-14. https://doi.org/10.2196/13446 [ Links ]
Warnock-Parkes, E., Wild, J., Thew, G. R., Kerr, A., Grey, N., Stott, R., Ehlers, A., & Clark,D.M. (2020). Treating social anxiety disorder remotely with cognitive therapy. The Cognitive Behaviour Therapist, 13(30),1-20. https://doi.org/10.1017/S1754470X2000032X [ Links ]
Westerhof, G. B., Lamers, S. M. A., Postel, M. G., & Bohlmeijer, E. T. (2019). Online Therapy for Depressive Symptoms: An Evaluation of Counselor-Led and Peer- Supported Life Review Therapy. The Gerontologist, 59 (1). 135-146. https://doi.org/10.1093/geront/gnx140 [ Links ]
Yuen, E.K., Herbert, J.D., Forman, E.M., Goetter, E.M., Juarascio, A.S., Rabin, S., Goodwin, C., & Bouchard, S. (2013). Acceptance based behavior therapy for social anxiety disorder through videoconferencing. Journal of Anxiety Disorders, 27(4),389-397. https://doi.org/10.1016/j.janxdis.2013.03.002 [ Links ]
 Correspondence:
Correspondence:
Maria José Nunes Gadelha
E-mail: maria.gadelha@ufrn.br
Este artigo foi submetido no SGP (Sistema de Gestão de Publicações) da RBTC em 23 de Agosto de 2021. cod. 250
Artigo aceito em 08 de Outubro de 2021


{kind=link}
{kind=link}