










Serviços Personalizados
artigo
 texto em
texto em  Português (pdf)
Português (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkRevista Brasileira de Terapias Cognitivas
versão impressa ISSN 1808-5687versão On-line ISSN 1982-3746
Rev. bras.ter. cogn. vol.17 no.2 Rio de Janeiro jul./dez. 2021
http://dx.doi.org/10.5935/1808-5687.20210027
THEORETICAL REVIEW
Online group intervention: online G10 experience report
Tânia Moraes Ramos Andrade; Karen Priscila Del Rio Szupzynski; Rodrigo Casagrande de Lima Paganella; Margareth Da Silva Oliveira; Paulo Knapp
PUCRS, Programa de Pós-graduação em Psicologia - Porto Alegre - RS - Brasil
ABSTRACT
The COVID-19 pandemic negatively impacted the mental health of the population, causing increased levels of stress, anxiety and depression. Isolation and social distancing demand the use of digital media as an essential tool to enable psychological interventions focused on treatment, prevention and promotion of mental health. The aim of this study was to describe an experience report on the adaptation and feasibility of applying the G10 program online, during the period of social distancing from COVID-19. The sample consisted of 14 participants who underwent the evaluation of the DASS-21 scale, pre and post-intervention. The results identified a statistically significant difference in the Stress dimension (p=0.005), in which a reduction in symptoms was identified after the intervention. Equally significant results were observed in the dimensions of Anxiety (p=0.032) and Depression (p=0.028). The qualitative data obtained suggest the development, at the group level, of cohesion among group members around common purposes and feelings of belonging; and, on a personal level, coping strategies to deal with stressful situations and self-knowledge about values ??and character strengths.
Keywords: Groups; Internet-based intervention; Behavioral and cognitive therapies; Third wave; Covid-19.
INTRODUCTION
Technological development in health has progressively increased and gained more space, and the use of technologies to improve the supply of health services is called eHealth (Rocha et al., 2016). Additionally, mobile devices are increasingly widespread, giving health workers and patients the possibility to access health services anywhere, anytime.
The exponential growth of technologies was driven by the COVID-19 pandemic that started in December 2019. According to the Brazilian Ministry of Health (2020), the first COVID-19 case was diagnosed in Brazil at the end of January 2020. The disease spread rapidly across the country, leading to the collapse of the health care system in some states. On June 16th, 2020, Brazil surpassed 934,000 confirmed cases, with more than 45,000 deaths caused by COVID-19. The situation worldwide indicated urgent measures were needed to mitigate the collapse of the health system. These measures included social isolation and social distancing, among other important recommendations. The impact of the pandemic goes beyond the effects directly related to the virus and disease, considering that society is experiencing increasing uncertainty that leads to symptoms such as stress, anxiety, and depression. Guidelines to support mental health guidance and psychosocial care were developed in accordance to the "Recomendações e orientações em saúde mental e atenção psicossocial na COVID-19." [Recommendations and guidelines concerning mental health and psychosocial care within the COVID-19 context] published by the Oswaldo Cruz Foundation (Noal et al., 2020).
Many face-to-face services were interrupted by the widespread adoption of social isolation measures, and technology emerged as a powerful resource. As a result, all human relations started being mediated by some device connected to the Internet (Noal et al., 2020). As a result, online psychological interventions were considered a resource that could directly benefit all those involved and the collective, developing greater empathy and concern with society.
Group interventions are a "fertile ground" to reinforce positive competencies. Every whole human being can provide some knowledge in a given context that can benefit the collective (Rodriguez et al., 2017). In this sense, valuing collective intelligence involves finding a context in which an individual's knowledge is valuable and essential for developing a specific group (Bembem & Santos, 2013). Collective intelligence is defined by Lévy (2015) as the result of the effective mobilization of human competencies, that is, intelligence distributed everywhere, incessantly valued, and coordinated in real-time. It is, therefore, necessary to understand that each individual has knowledge based on experiences obtained throughout life that can be shared. Hence, collective intelligence would be a structure for human relations, and a sense of belonging to a place or ideology would no longer bring people together but rather the ability to share individual knowledge (Bembem & Santos, 2013).
Emotional dysregulation is associated with the concept of collective intelligence and is related to high levels of negative responses such as fear, sorrow, anger, and the inability to recognize and name emotions. Emotional psychoeducation enables people to understand their emotions and triggers and adapt to a given context (e.g., communicating their feelings assertively). When psychoeducation is provided to groups, people tend to acknowledge that emotional difficulties are common to other people, which leads to a sense of shared humanity, from which social skills related to emotional, cognitive, and behavioral events can be explored. Hence, social skills are also vital to construct collective intelligence because they refer to behaviors that are efficiently and adequately expressed in interpersonal relations to communicate feelings, attitudes, opinions, or rights in a situational and cultural context (Caballo, 2003; Pureza et al., 2013). Social skills constitute protective factors in human development (Cecconello & Koller, 2000), denoting the importance of interventions to teach these skills to different groups and contexts. Cognitive-behavioral techniques are predominantly employed in social skills training (Murta, 2005). These techniques include providing instructions, promoting behavioral rehearsal, modeling, giving verbal feedback, and video feedback, home assignments, promoting cognitive restructuring, problem-solving, and relaxation (Caballo, 2003; Del Prette & Del Prette, 1999); experiential techniques are also used in group interventions (Del Prette & Del Prette, 2001a, 2001b). These techniques are intended to modify behavioral (behavioral rehearsal), cognitive (cognitive restructuring), and physiological (relaxing) components, typical in social skill deficits (Herbert et al., 2005; Murta, 2005).
Group cohesion must be developed and constantly reinforced for a group to share emotional deficits or a lack of social skills. Strengthening interpersonal bonds involves high levels of empathy and the need to be emotionally and psychologically available to others (Falcone, 1999). Empathy is considered essential for human experience and social cognition. Empathy is the ability to sense other people's feelings (affective component) and understanding someone else's experience and perspective (cognitive component) (Melloni, Lopez & Ibanez, 2014).
Additionally, another important foundation to construct collective intelligence is character strengths and virtues; to the extent, these suggest the identification and development of human potentialities (Seibel, DeSousa & Koller, 2015). The classification of character strengths was proposed by the first comprehensive and systematic studies in psychology intending to classify essential human values (Peterson & Seligman, 2004; Rashid & Seligman, 2019). Character strengths can be conceptualized as positive traits of people that reflect thoughts, feelings, and behaviors (Park, Peterson & Seligman, 2004) and can be assigned to an individual's self (Rashid & Seligman, 2019).
Mindfulness is also associated with the conception of collective intelligence. Kabat-Zinn (2003) defines mindfulness as awareness that emerges when we purposefully pay attention to the present moment, as a given experience unfolds, nonjudgement. From another perspective, Langer (1989) states that the opposite of mindfulness is being on the "autopilot" or mindlessness, which is characterized by mental distraction, when an individual operates without paying attention to the task at hand, stuck to previously established categories or ingrained habits, or yet, seeing the world from a single perspective (Vandenberghe & Assunção, 2009; Langer, 2014). Studies addressing clinical interventions based on mindfulness have presented various techniques in cognitive-behavioral therapy (Wenzel, 2018; Germer, Siegal & Fulton, 2016; Hayes, Follette & Linehan, 2004). For example, Beck (2013) notes that mindfulness helps individuals observe and accept their inner experiences nonjudgement or assessing or trying to change these experiences. Hayes and Wilson (2003) add that mindfulness is a method or set of techniques that direct acceptance processes, cognitive defusion, and exposure.
Note that different types of impacts may be generated by the intense and abrupt changes caused by the pandemic. Helgeson, Reynolds, and Tomich (2006) described that positive changes associated with bad events are differently classified, namely: posttraumatic growth, stress-related growth, and benefit finding when facing trauma. However, perhaps the best term is "posttraumatic growth" because it highlights potential evolution/maturity compared to an individual's previous level of functioning. Additionally, the term "traumatic" underlines that growth comes after a significant event, and progress did not come from minor stressors nor was a natural part of a personal development process (Valverde, Baylos, & Torres, 2009; Zoellner & Maercker, 2006).
Barros and collaborators (2020) addressed 45,161 Brazilian individuals and verified that approximately 40% of the sample felt sad or depressed during the COVID-19 pandemic; 52.6% reported more anxiety or nervousness; 43.5% reported the onset of sleep problems, and 48.0% reported that preexisting sleep problems worsened. Related symptoms were most frequent among young or adult women and individuals with a previous history of depression. The high prevalence of symptoms of anxiety, stress, and depression reinforces the need to ensure the provision of mental health care adapted to the pandemic context.
In another study addressing 1,775 people, Barbosa and collaborators (2021) analyzed the frequency of anxiety, depression, and stress symptoms during the COVID-19 pandemic. The results revealed significantly higher means of the three symptoms assessed by the Depression, Anxiety and Stress Scale (DASS-21), more prevalent among unemployed single women and those who already presented some previous mental health symptoms.
Wang and collaborators (2020) conducted a study with 1,210 individuals residing in 194 cities in China and verified the prevalence of moderate to severe anxiety, depression, and stress symptoms during the COVID-19 pandemic. The results show that 28.8% of the participants presented significant levels of anxiety, 16.5% presented depression symptoms, and 8.1% showed important stress levels. A total of 75.2% of the sample reported fear that their families would be infected with the disease. Being a woman, a student, and having physical symptoms from COVID-19 or prior health problems were significantly associated with higher anxiety, depression, and stress levels.
According to Schmidt, Crepaldi, and Bolze (2020), psychology can support coping with the consequences of the COVID-19, and psychological interventions implemented during the pandemic can decrease emotional difficulties caused by social isolation and promote mental health. Additionally, it is important to evaluate interventions that can be used after the pandemic period, in order to assist in the rehabilitation process, elaboration of losses and other possible changes caused by the disease.
Given the previous discussion, this study's objective is to provide an experience report concerning the online modality of a group intervention (G10), intended to awaken collective intelligence, human relationships grounded on the mobilization of competencies, and valorization of multiple human skills during the COVID-19 pandemic. The G10 program's proposition is to help individuals broaden the way they look to themselves and their communities, identify and strengthen each participant's psychological power and the group as a whole, supporting them to be more effective in their projects to contribute to society.
Therefore, the G10 can contribute with measures that encourage people to look at the collective, developing greater empathy and consideration toward others, especially in a time of extreme social vulnerability caused by the COVID-19 pandemic.
METHOD
This experience report concerns the adaptation of the G10 interpersonal development program to the online modality after social distancing measures were imposed to restrain the dissemination of COVID-19.
Groups' participants
Online meetings were held with three groups, composed of 6 to 7 participants each. There were a total of 22 participants; most were women aged between 21 and 61. As for the participants' occupations, there were self-employed professionals (n=8), teachers (n=10), and students (n=4). Only 14 participants completed the instrument in the posttest.
Instruments
The following instruments were used to assess the participants:
• Sociodemographic questionnaire to collect data such as sex, age, education, marital status, occupation, among others;
• Depression Anxiety and Stress Scale (DASS-21) (Lovibond & Lovibond, 1995) - Short Form. DASS-21 was adapted and validated for the Brazilian context by Vignola and Tucci (2014). It is divided into three four-point Likert scales, with a total of 21 questions. Each subscale is composed of seven items designed to assess depression, anxiety, and stress. The final score is obtained by summing the scores obtained in the seven items of each of the three subscales. In the end, the scale provides three scores, one for each subscale, with a minimum of "0" and a maximum score of "21". DASS-21 was used to test and re-test the participants and monitor their anxiety, stress, and depression levels and the intervention's effects on these symptoms.
Intervention
The online G10 program is part of the Programa de Desenvolvimento Interpessoal G10 [G10 Interpersonal Development Program] of the Research Group "Avaliação e Atendimento em Psicoterapia Cognitiva e Comportamental" (GAAPCC) [Assessment and Care in Cognitive and Behavioral Psychotherapy], from the Graduate Program in Psychology at PUCRS.
The G10 program is intended to promote personal and social development, encouraging the participants to broaden the way they look at themselves and their communities, strengthening each participant's psychological power and the group as a whole. Cognitive-behavioral techniques (e.g., identification of automatic thoughts) are adopted during meetings to promote the participants' intrapersonal and interpersonal development and expand repertoires, coping strategies, training skills, and techniques to promote empathy, assertiveness, and mindfulness. The cognitive model was also a fundamental part of the meetings. The way people feel emotionally and behave can be mediated by cognitive processing influencing how they perceive or interpret events (Beck, 2013). Dysfunctional thoughts, cognitive distortions, and underlying beliefs are directly associated with psychological distress and psychopathology (Knapp and Beck, 2008). Hence, the G10 program follows the assumptions of cognitive-behavioral therapy to provide the participants with a better understanding of human functioning. The urgent need to support the population in general due to the COVID-19 pandemic determined that the program initially idealized for ten face-to-face meetings (Table 1) was condensed into five online meetings (Table 2). This change enabled forming leaderships, so the collective was maintained in a time so important for life in society. Due to the COVID-19 pandemic, the G10's remote modality acquired new relevance and significance, considering the ability of the program to gather different people in collective action. The online modality facilitated access, and more people adhered to the intervention.
The original G10 program is composed of ten meetings that last 1 hour and 30 minutes on average. However, adaptation to the online modality demanded that the most relevant topics were revised to meet the needs that emerged in the pandemic context. Hence, the adapted program was composed of five remote meetings, each lasting 1 hour and 30 minutes, held via Google Meet. The complete adapted program is presented in Table 2.
The structure of the meetings was the same in all the groups. All the meetings included common strategies: welcome, mindfulness techniques, agenda for the day, and weekly assignments.
Data Collection Procedures
The program was publicized during the pandemic on social networks and the research group and G10 program's website. The post provided information on the G10 program, reporting its objectives, number and duration of meetings, starting date, the fact it is free of charge, registration link, asking for personal information, and DASS-21 scale.
Ethical Considerations
Ethical guidelines, provided by Resolution 510/16, Brazilian Council of Health (CNS), were complied with in all the study's stages, and the project was submitted to the Scientific Committee at the Escola de Ciências da Saúde e da Vida. The project was approved by the Institutional Review Board at the Pontifícia Universidade Católica do Rio Grande do Sul (CAAE 79241717.0.0000.5336).
Statistical Analysis
This study's central objective is an experience report; however, some quantitative data are presented to illustrate how the intervention was applied. Data were statistically treated using the Statistical Package for Social Sciences version 25.0. The statistical significance level was set at 5%. Descriptive statistics were used to present the results using absolute and relative frequencies (n - %), measures of central tendency (mean and median), and variability (standard deviation and interquartile range). The Shapiro-Wilk test analyzed the symmetry of the distributions. The Wilcoxon rank test was used to compare the scores based on the participants' measurements at two points in time (pre- and post-intervention). To identify the magnitude of the differences between pre- and post-intervention scores, the Cohen effect size was calculated with correction by Hedges and Olkin (1985). The Cohen cutoff points (Cohen, 1992) are classified as: negligible (d < 0.20); small (d > 0.20 and < 0.50); moderate (d > 0.50 and < 0.80), or large (d > 0.80).
RESULTS
This study refers to an experience report, and quantitative data are presented to illustrate and reinforce the importance of studies addressing online interventions intended to mobilize competencies and value multiple human skills. The intervention's purpose was to prevent anxiety, stress, and depression symptoms from aggravating by strengthening concepts such as collective intelligence, mindfulness, and resilience.
First, the G10 Program's face-to-face version was adapted to the online version. Then, due to a need to offer more mental health care alternatives to cope with the crisis caused by the COVID-19 pandemic, the G10 team held regular meetings online to proceed with and adapt the project. Tables 1 and 2 present the adaptation process and the final structure of the program's online version.
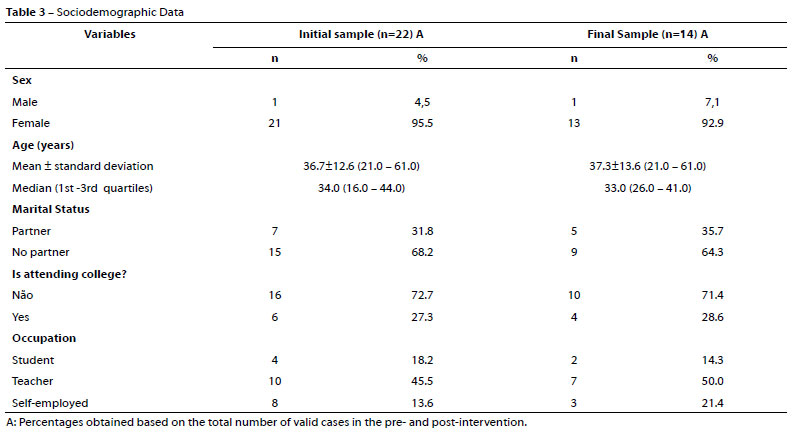
The initial database was composed of 22 participants, predominantly women, 95.5% (n=21) aged between 21 and 61; 36.7 years old on average (SD=12.6). Regarding marital status, 68.2% (n=15) of the participants reported having no partner. As for educational level, 27.3% (n=6) reported undergraduate studies, and regarding occupation, 45.5% (n=10) reported being a teacher. At the end of the intervention, there were 36.4% (n=8) of missing cases, so 14 participants (63.6%) remained. The characteristics of this group are presented in Table 3.
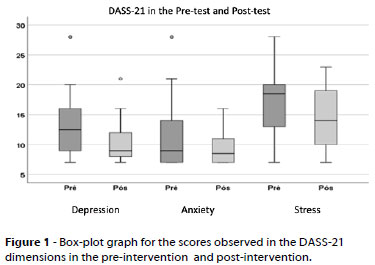
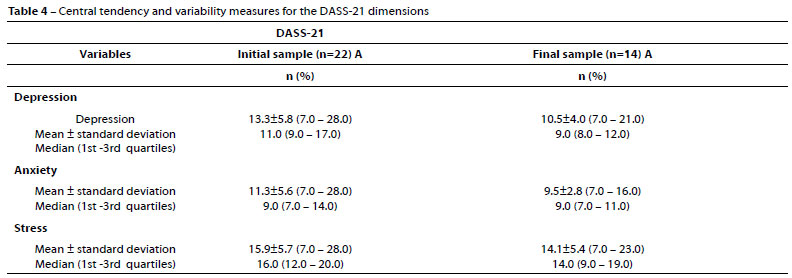
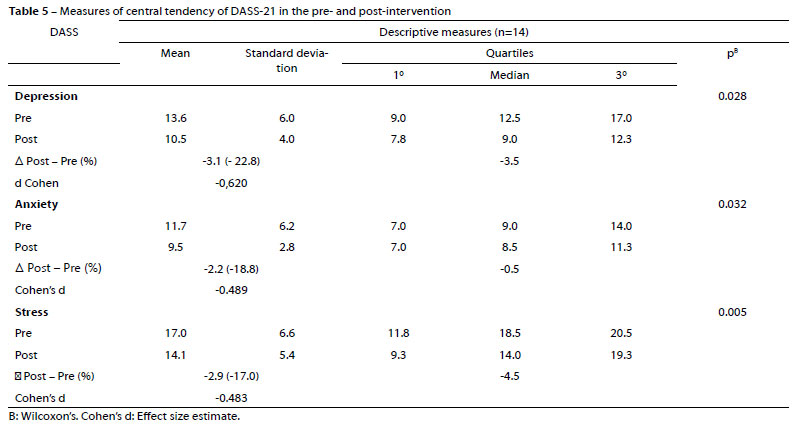
The pre- and post-test scores obtained by the 14 participants who completed the study were compared in the DASS-21 dimensions. As the results presented in Table 4 show, Wilcoxon's test detected a statistical significance in the Stress dimension (p=0.005); that is, symptomatology decreased after the intervention. Equally significant results were found in the Anxiety (p=0.032) and Depression (p=0.028) dimensions.
The means obtained in the depression, anxiety, and stress dimensions were assessed before the intervention, and the following was obtained for depression 13.6 (SD=6.0), anxiety 11.7 (SD=6.2), and stress 17.0 (SD=6.6). The means changed after the intervention: 10.5 (SD=4.0) for depression, 19.5 (SD=2.8) for anxiety, and 14.1 (SD=5.4) for stress. The estimated "effect size" can be considered to verify the program's effect, and the intervention's highest impact was on the Depression dimension, which presented a moderate effect size (Cohen's d = -0.620) [i.e., a "moderate" decrease in magnitude was found at the end of the intervention]. Regarding the Anxiety (Cohen's d = -0.489) and Stress (Cohen's d = -0.483) dimensions, the impact of the intervention was classified as a small magnitude.
Figure 1 presents the differences between the means obtained before and after the intervention. Therefore, even though it is an experience report, data indicate higher representativeness of the results obtained for depression symptoms.
DISCUSSION AND FINAL ONSIDERATIONS
This study's objective was to report the experience of adapting the G10 interpersonal development program to the online modality. The results show the importance of adequately adapting an intervention protocol, assessing the feasibility of its application. Adapting the program to fewer and shorter sessions enabled more participants to adhere to the program's online version. Additionally, the program in this modality was feasible and could be offered in other circumstances, and its effectiveness could be tested. Another relevant fact concerning this adaptation was the structure proposed for the sessions. The fact that all the sessions were initiated by welcoming the participants, a time when the therapist would allow the participants to talk about themselves or asked about their families, was reported by most participants as being very positive. Feedback also showed that the participants valued being welcomed, as one of the participants reported: "I felt cared for by the group. It strengthened me, and I knew that I'd be with kind people who had the same purpose as I did, which was thinking about the collective" (T.A., 43 years old).
Even though this paper's objective was not to discuss results concerning effectiveness, note that the quantitative data were very satisfactory. According to comparisons between the test and retest, the results concerning anxiety (p=0.032), depression (p=0.028), and stress (p=0.005) showed statistically significant differences after the intervention. Note that the decreased stress levels suggest that the participants needed an opportunity to express their anxieties and improve their coping strategies to deal with the challenging experience presented by the pandemic (Barros et al., 2020; Wang et al., 2020). These promising results corroborate with those reported in the literature (Barbosa et al., 2021).
Most participants reported difficulties with social distancing because they missed social interaction, leaving home for work, studying, running errands, and all activities they performed before the pandemic. Hence, some members used the group to share their anxieties and also exchange positive experiences. This need became even more apparent, considering that institutions, such as schools, companies, and churches were closed, triggering feelings of loneliness and vulnerability. These results are associated with the findings presented by Schmidt and collaborators (2020), who highlight the importance of interventions to strengthen connections with social support networks, even if remotely.
According to the participants' reports, the meetings favored a feeling of well being and improved the relationship with their families. Various participants reported less anxiety, more empathy, and more tolerance toward themselves and others, especially when working in the home office. In addition, many participants started using breathing and relaxing techniques in their daily lives to control stress.
It is worth noting the participants' attendance and punctuality. Many reported that the fact that G10 was available online facilitated adherence to the meetings. This fact corroborates the literature that reports the differentials of online interventions, considering their benefits such as easier access, low cost, and reach (Rocha et al., 2016), as some participants report:
"a friend of mine had attended the face-to-face version, but I couldn't because of my work and the fact it was far away from home. But it is online now, which facilitated my participation." (M, Z., 34 years old)
"This was one good thing about the pandemic, I was open to new things... and G10 was great." (E. O., 31 years old)
"I wouldn't have the chance to attend it otherwise because I live outside Poa" (I.H., 57 years old)
"I live by myself, so I'm always excited for the G10 meeting; I even wear lipstick" (N.S., 56 years old)
Strong group cohesion was developed via the online G10 program with the constant presence of empathy. The participants were concerned with everyone's physical and emotional health and expressed their concern, always recommending each other to "take care." The participants also showed concern with each other's family members being infected, hospitalized, or losing family members and friends. One of the groups remained in contact after the meetings ceased, keeping solid interpersonal relationships and being supportive in situations such as the loss of family members or one of the participants becoming infected with COVID-19. This group still meets monthly and supports each other in the face of adversities. Hence, the intervention showed strong potential to encourage empathy and reinforce the importance of personal relations, especially in the current pandemic situation (Melloni, Lopez & Ibanez, 2014; Falcone, 1999).
Another satisfactory result, which reinforces the idea of future studies addressing the effectiveness of interventions, was the reports related to the topics addressed in the meetings. Many participants reported that knowledge of psychological and emotional aspects encouraged them to: "think about the collective, values and purposes, learn about how to deal with stressful situations, to control stressful situations and emotions." It is clear that contexts in which psychoeducation is provided and teach these concepts benefit the participants and encourage collective actions, expanding collective intelligence and/or personal agency (Bembem & Santos, 2013; Rodriguéz et al., 2017).
One of the G10's central objectives is to develop collective intelligence and produce actions within communities. The meetings had the objective to develop personal characteristics to promote collective intelligence, with relationships grounded on the valorization of multiple human skills. The participants' reports revealed that some already worked with social projects while others desired to participate in these projects; however, they were not sufficiently engaged. The following excerpt illustrates the extent to which this characteristic was encouraged and reinforced among the participants: "I've been working in a project with homeless people for many years, and talking about the collective made all the difference, you even contributed with food for donation when I asked." (A.S., 56 years old)
The previous discussion shows that the G10 intervention adapted to the online modality has the potential to develop critical characteristics in situations such as the novel coronavirus pandemic. In addition, the exponential growth of health technologies driven by social isolation and social distancing measures requires studies providing more mental health care alternatives (Noal, Passos & Freitas, 2020). In Brazil, few studies address online interventions, reinforcing this study's innovative nature.
It is also important to highlight some of this study's limitations. First, this is an experience report, which restricts the generalization of the results. Additionally, this study's sample is considered small as it concerned a pilot study in which the G10 Program was implemented online. Another limitation concerns the loss of participants between test and retest. The authors considered it probably happened due to some participants' difficulty accessing the Internet and difficulties applying the questionnaires after the intervention.
Furthermore, the pandemic represented a challenge surrounded by uncertainty, which may have influenced how the sessions were conducted, hindering the appropriate reproduction of the stages in each session. It was difficult keeping the meetings' focus and structure because the participants presented diverse demands. Nevertheless, satisfactory results were achieved, suggesting that future studies should address the effectiveness of interventions and reinforce the need to expand mental health services in the online modality in Brazil.
REFERENCES
Barbosa, L. N. F., Melo, M. C. B. D., Cunha, M. C. V. C., Albuquerque, J. M., Costa, J. M., & Silva, E. F. F. S. (2021). Frequência de sintomas de ansiedade, depressão e estresse em brasileiros na pandemia COVID-19. Revista Brasileira de Saúde Materno Infantil, 21(Suppl 2),413-419. https://doi.org/10.1590/1806-9304202100S200005 [ Links ]
Barros, M. B. D. A., Lima, M. G., Malta, D. C., Szwarcwald, C. L., Azevedo, R. C. S. D., Romero, D., ... Gracie, R. (2020). Relato de tristeza/depressão, nervosismo/ansiedade e problemas de sono na população adulta brasileira durante a pandemia de COVID-19. Epidemiologia e Serviços de Saúde, 29(4),e2020427. https://doi.org/10.1590/S1679-49742020000400018 [ Links ]
Beck, J. S. (2013). Terapia cognitivo-comportamental. Artmed. [ Links ]
Bembem, A. H. C., & Santos, P. L. V. (2013). Inteligência coletiva: Um olhar sobre a produção de Pierre Lévy. Perspectivas em ciência da informação, 18(4),139-151. https://doi.org/10.1590/S1413-99362013000400010 [ Links ]
Brasil. Ministério da Saúde (MS). (2020). COVID-19: Painel Interativo. https://qsprod.saude.gov.br/extensions/covid-19_html/covid-19_html.html [ Links ]
Caballo, V. E. (2003). Manual de avaliação e treinamento das habilidades sociais. Santos. [ Links ]
Cecconello, A. M., & Koller, S. H. (2000). Competência social e empatia: Um estudo sobre resiliência com crianças em situação de pobreza. Estudos de Psicologia (Natal), 5(1),71-93. https://doi.org/10.1590/S1413-294X2000000100005 [ Links ]
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1),155-159. https://doi.org/10.1037/0033-2909.112.1.155 [ Links ]
Da Conceição, I. K., Andrade, T. M. R., Knapp, P., Oliveira, M. da S., Argimon, I. I. de L. (2015). Ensinando Terapeutas a Desenvolver Empoderamento [Apresentação de Pôster]. XII Congresso Brasileiro de Terapias Cognitivas. Ribeirão Preto. [ Links ]
Del Prette, Z. A. P., & Del Prette, A. (1999). Psicologia das Habilidades Sociais: Terapia e educação. Vozes. [ Links ]
Del Prette, Z. A. P., & Del Prette, A. (2001a). Inventário de habilidades sociais (IHS-Del-Prette): Manual de apuração e interpretação. Casa do Psicólogo. [ Links ]
Del Prette, Z. A. P., & Del Prette, A. (2001b). O uso de vivências no treinamento de habilidades sociais. In M. L. Marinho, & V. E. Caballo (Orgs.), Psicologia clínica e da saúde (pp. 117-135). UEL. [ Links ]
Falcone, E. (1999). Avaliação de um programa de treinamento da empatia com universitários. Revista Brasileira de TerapiaComportamental e Cognitiva, 1(1),23-32. https://doi.org/10.31505/rbtcc.v1i1.267 [ Links ]
Germer, C. K., Siegel, R. D., & Fulton, P. R. (2016). Mindfulness e psicoterapia. Artmed. [ Links ]
Hayes, S. C., & Wilson, K. G. (2003). Mindfulness: method Method and process. Clinical Psychology: Science and Practice, 10(2),161-165. https://doi.org/10.1093/clipsy.bpg018 [ Links ]
Hayes, S. C., Follette, V. M., & Linehan, M. (Eds.). (2004). Mindfulness and acceptance: Expanding the cognitive-behavioral tradition. Guilford Press. [ Links ]
Hedges, L. V., & Olkin, I. (1985). Statistical Methods for MetaAnalysis. Academic Press. [ Links ]
Helgeson, V. S., Reynolds, K. A., & Tomich, P. L. (2006). A meta-analytic review of benefit finding and growth. Journal of Consulting and Clinical Psychology, 74(5),797-816. https://doi.org/10.1037/0022-006X.74.5.797 [ Links ]
Herbert, J. D., Gaudiano, B. A., Rheingold, A. A., Myers, V. H., Dalrymple, K., & Nolan, E. M. (2005). Social skills training augments the effectiveness of cognitive behavioral group therapy for Social Anxiety Disorder. Behavior Therapy, 36(2),125-138. https://doi.org/10.1016/S0005-7894(05)80061-9 [ Links ]
Kabat-Zinn, Jon (2003): Mindfulness-Based Interventions in Context. Past, Present, and Future. Clinical Psychology: Science and Practice, 10(2),144-156. https://doi.org/10.1093/clipsy.bpg016 [ Links ]
Knapp, P., Argimon, I. I. de L., Machado, S. da S. (2019). G10 - Programa de desenvolvimento interpessoal: Uma interlocução entre inteligência coletiva e terapia cognitiva [Mesa Redonda]. XII Congresso Brasileiro de Terapias Cognitivas & XI Congresso Latino-Americano de Terapias Cognitivas e Comportamentais, Fortaleza, Ceará, Brasil. [ Links ]
Knapp, P., & Beck, A. T. (2008). Fundamentos, modelos conceituais, aplicações e pesquisa da terapia cognitiva. Brazilian Journal of Psychiatry, 30(Suppl 2),S54-S64. https://doi.org/10.1590/S1516-44462008000600002 [ Links ]
Langer, E. J. (1989). Minding matters: The consequences of mindlessness-mindfulness. Advances in Experimental Social Psychology, 22, 137-173. Academic Press. https://doi.org/10.1016/S0065-2601(08)60307-X [ Links ]
Langer, E. J. (2014). Mindfulness, 25th anniversary edition (2nd ed., pp. 3-43). Da Capo Press. [ Links ]
Lévy, Pierre. (2015). A inteligência coletiva: Por uma antropologia do ciberespaço. Edições Loyola. [ Links ]
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the Depression Anxiety & Stress Scales (DASS-21) (2nd ed.). Psychology Foundation. [ Links ]
Melloni, M., Lopez, V., & Ibanez, A. (2014). Empathy and contextual social cognition. Cognitive, Affective, & Behavioral Neuroscience, 14(1),407-425. https://doi.org/10.3758/s13415-013-0205-3 [ Links ]
Murta, S. G. (2005). Aplicações do treinamento em habilidades sociais: Análise da produção nacional. Psicologia:Reflexão e crítica, 18(2),283-291. https://doi.org/10.1590/S0102-79722005000200017 [ Links ]
Noal, D. da S., Passos, M. F. D., & Freitas, C. M. de (Orgs.). (2020). Recomendações e orientações em saúde mental e atenção psicossocial na COVID-19. Fundação Oswaldo Cruz. https://www.arca.fiocruz.br/handle/icict/44264 [ Links ]
Park, N., Peterson, C., & Seligman, M. E. (2004). Strengths of character and well-being. Journal of social and Clinical Psychology, 23(5),603-619. https://doi.org/10.1521/jscp.23.5.603.50748 [ Links ]
Peterson, C., & Seligman, M. E. (2004). Character strengths and virtues: A handbook and classification (Vol. 1). Oxford University Press. [ Links ]
Pureza, J., Rusch, S., Wagner, M. F., & Oliveira, M. da S. (2012). Treinamento de habilidades sociais em universitários: Uma proposta de intervenção. Revista Brasileira de Terapias Cognitivas, 8(1),2-9. doi: 10.5935/1808-5687.20120002 [ Links ]
Rashid, T., & Seligman, M. (2019). Psicoterapia positiva: Manual do terapeuta. Artmed. [ Links ]
Resolução CNS nº 510, de 07 de abril de 2016. O Plenário do Conselho Nacional de Saúde em sua Quinquagésima Nona Reunião Extraordinária, realizada nos dias 06 e 07 de abril de 2016, no uso de suas competências regimentais e atribuições conferidas pela Lei n o 8.080, de 19 de setembro de 1990, pela Lei n o 8.142, de 28 de dezembro de 1990, pelo Decreto n o 5.839, de 11 de julho de 2006, e. https://bvsms.saude.gov.br/bvs/saudelegis/cns/2016/res0510_07_04_2016.html [ Links ]
Rocha, T. A. H., Fachini, L. A., Thumé, E., Silva, N. C. D., Barbosa, A. C. Q., Carmo, M. D., & Rodrigues, J. M. (2016). Saúde Móvel: Novas perspectivas para a oferta de serviços em saúde. Epidemiologia e Serviços de Saúde, 25(1),159-170. https://doi.org/10.5123/S1679-49742016000100016 [ Links ]
Rodríguez, G., Givaduan Moreno, M. E., Ramírez Hernández, M., Valdez Arellano, E. I., & Pick Steiner, S. (2017). El cuidado de la salud como semilla para el desarrollo: experiencia de un programa basado en habilidades para la vida y reducción de barreras psicosociales. Acta de investigación psicológica, 7(2),2647-2657. https://doi.org/10.1016/j.aipprr.2017.06.002 [ Links ]
Schmidt, B., Crepaldi, M. A., Bolze, S. D. A., Neiva-Silva, L., & Demenech, L. M. (2020). Saúde mental e intervenções psicológicas diante da pandemia do novo coronavírus (COVID-19). Estudos de Psicologia (Campinas), 37. [ Links ]
Seibel, B. L., DeSousa, D., & Koller, S. H. (2015). Adaptação brasileira e estrutura fatorial da escala 240-item VIA Inventory of Strengths. Psico-USF, 20(3),371-383. https://doi.org/10.1590/1413-82712015200301 [ Links ]
Valverde, C. V., Baylos, C. C., & Torres, G. H. (2009). Reacciones frente al trauma: vulnerabilidad, resistencia y crecimiento. Emociones Positivas, 375-392. [ Links ]
Vandenberghe, L., & Assunção, A. B. (2009). Concepções de mindfulness em Langer e Kabat-Zinn: um encontro da ciência Ocidental com a espiritualidade Oriental. Contextos Clínicos, 2(2),124-135. https://doi.org/10.4013/4921 [ Links ]
Vignola, R. C., & Tucci, A. M. (2014). Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. Journal of Affective Disorders,28,104-109. https://doi.org/10.1016/j.jad.2013.10.031 [ Links ]
Wang, C., R., Wan, X., Tan, Y., Xu, L., Ho, C. S., & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal Environmental Research and Public Health, 17(5),1729. https://doi.org/10.3390/ijerph17051729 [ Links ]
Wenzel, A. (2018). Inovações em Terapia Cognitivo-Comportamental: Intervenções estratégicas para uma prática criativa. Artmed. [ Links ]
Zoellner, T., & Maercker, A. (2006). Posttraumatic growth in clinical psychology-A critical review and introduction of a two component model. Clinical Psychology Review, 26(5),626-653. https://doi.org/10.1016/j.cpr.2006.01.008 [ Links ]
 Correspondence:
Correspondence:
Karen Priscila Del Rio Szupzynski
E-mail: karenszu@yahoo.com.br
Este artigo foi submetido no SGP (Sistema de Gestão de Publicações) da RBTC em 25 de Mês de 2021. cod. 255
Artigo aceito em 15 de Outubro de 2021


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}