










Serviços Personalizados
artigo
 texto em
texto em  Português (pdf)
Português (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkRevista Brasileira de Terapias Cognitivas
versão impressa ISSN 1808-5687versão On-line ISSN 1982-3746
Rev. bras.ter. cogn. vol.18 no.1 Rio de Janeiro jan./jun. 2022
http://dx.doi.org/10.5935/1808-5687.20220009
10.5935/1808-5687.20220009 THEORETICAL REVIEW
Cognitive-behavioral therapy and emotional regulation to chronic pain management in randomized clinical trials: a scoping review
Lucas Geremia La PortaI; Prisla Ücker CalvettiII
IFederal University of Health Sciences of Porto Alegre/UFCSPA, Department of Psychology - Porto Alegre - RS - Brazil
IIFederal University of Health Sciences of Porto Alegre/UFCSPA, Postgraduate Program in Health Sciences - Porto Alegre - RS - Brazil
ABSTRACT
Chronic pain affects 20% of the world population, causing significant economic and biopsychosocial impact. Cognitive behavioral therapies have presented evidence for treating chronic pain.
OBJECTIVE: to investigate the scientific production of randomized clinical trials involving cognitive-behavioral intervention and emotional regulation in the treatment of patients with chronic pain in digital and face-to-face mode.
METHOD: scoping review of the PubMed, Scopus, Web of Science, PsycInfo, and Cochrane Central databases, conducted between May 2019 and February 2020, following PRISMA guidelines.
RESULTS: 24 studies were found, 6 of which are included in this review. The most frequent outcomes were catastrophizing, pain management, depressive symptoms, affection, and coping. Most cognitive-behavioral interventions combined integrative approaches, especially mindfulness, in internet-based and face-to-face modes and included follow-up. The outcomes related to pain and affective- emotional aspects showed improvement.
CONCLUSION: Internet-based and face-to-face Cognitive and behavior therapies showed evidence of clinically significant contributions to affective and emotional aspects of the treatment of chronic pain.
Keywords: cognitive behavioral therapy; emotional regulation; chronic pain; randomized controlled trial.
INTRODUCTION
Chronic pain is defined as pain that lasts or occurs repeatedly for a period of over three months; it affects 20% of the world population, which makes it a relevant source of pain and economic distress. It is generally accompanied by demoralization, anguish, and functional impairment. The classification of chronic pain prepared by the IASP - International Association for the Study of Pain - is based on current scientific evidence and on the biopsychosocial model (Barke, 2019).
Pain is classified into three categories according to how long it lasts: acute, recurring, and chronic. Acute pain is identified as a burn, fracture, or muscle fatigue. In terms of intensity, pain may be continuous, moderate or acute. Pain impacts the quality of life, increases an individual's vulnerability to other diseases, particularly in the domain of mental health; causes functional difficulties such as anxiety and depression, and impairs aspects of professional (medical leave, absenteeism, retirement) or school and work. Even if pain presents an adaptive function for the organism, it is characterized as chronic when its duration exceeds three months, and it modifies the person's physiology, cognition, emotions, and behavior (Calvetti & Segabinazzi, 2019).
The affective-emotional aspect of pain refers to the relation between pain and humor, among the emotional and behavioral reactions caused by the pain process.
Research psychologist Ronald Melzack has proposed the Neuromatrix Theory of Pain, a biopsychosocial perspective model stating that the experience of pain is defined by neuronal stimuli arising from genetic and sensorial influences, and also by cognitive processes, and physical and psychological stress that affect the muscles, which, in turn, generates acute and chronic pain. Therefore, there is a complex relationship between psychological stress and symptoms of chronic pain (Santos et al., 2018).
The definition of pain categories varies according to the perceived location, etiology, or the main anatomic system affected. The new category in the ICD-11 - the International Classification of Diseases (WHO, 2022) - for "chronic pain" includes the most usual relevant clinical ailments and is divided into seven groups: (a) primary chronic pain; (b) cancer chronic pain; (c) post-traumatic or post-surgical chronic pain; (d) chronic neuropathy pain; (e) chronic orofacial and head pain; (f) visceral chronic pain; and (g) chronic musculoskeletal pain (Treede et al., 2015).
Treatment of chronic pain includes the prescription of long-term interventions, which must offer a good cost-benefit ratio, and be objective and feasible, so the patient can adhere to the treatment. Assessment of pain must be systematic and consider its sensorial and emotional aspects. Therefore, the patient must be continuously re-evaluated, since the treatment may be changed, doses readjusted, and the analgesics reduced and eventually discontinued, based on the results of those evaluations (Thorn, 2017).
Among the interdisciplinary programs for managing pain, cognitive-behavioral therapy (CBT) has revealed itself the psychosocial treatment of choice for chronic pain treatment. Its main goals include identifying and substituting poorly adaptive cognitions, emotions, and behavior for others that are more adaptive (Gatchel, McGeary, McGeary & Lippe, 2014). CBT does not present the risks associated with chronic pain medicine, surgery, and intervention procedures, even if the average effect extent on pain outcomes is small to moderate. Integrating CBT into medical environments, especially in primary care, shows significant perspectives for the evolution of outcomes (Ehde, Dillworth & Turner, 2014).
Emotional regulation can encompass any coping strategy, adaptive or not, used by the person when facing undesired emotional intensity. Whatever the style of coping, emotional regulation depends on the context and the situation (Aldao & Plate, 2020).
In various segments of applied Psychology, emotional regulation has gained relevance, especially for therapeutic reasons, and mainly in the field of Behavioral and Cognitive Therapies (Gutiérrez & Munoz-Martinez, 2013). Therefore, like a homeostatic thermostat, emotional regulation is capable of regulating emotions and keeping them at a "manageable level" so they can be dealt with (Leahy, 2013).
All emotions have a regulating role to perform; they are complex sets of chemical and neuronal reactions that form a pattern. The manner in which emotions are regulated is a process that requires different strategies to allow the organism to maintain homeostasis. Notably, emotions are regulated by interacting with other individuals (Crispim, 2015).
This study shows the relevance of conducting a scoping review in the field of evidence-based practice of cognitive-behavioral therapy (Dobson & Dobson, 2018) in randomized clinical trials and specially about internet-based CBT (Anderson, 2020) and face-to-face before pandemic period. Therefore, this study aims at analyzing scientific production regarding contributions of internet-based and face-to-face cognitive- behavioral therapy and emotional regulation process to chronic pain management in randomized clinical trials.
METHOD
This is a scoping review study. A search was conducted between May 2019 and February 2020, on the PubMed, PsycInfo, Web of Science, Scopus databases and on the Cochrane Central database, using the following descriptors: "cognitive behavioral therapy" AND ("emotional regulation" OR "emotional self regulation") AND ("clinical trial" OR "randomized") AND "chronic pain", according table 1. The descriptors were used in English in order to extend the reach of the search, since most publications on the subject are in English, and there are a limited number of relevant studies published in Portuguese. This study followed the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews andMeta-Analyses) (Moher et. al, 2015).
The following inclusion criteria were used to select items for analysis: (a) studies published until February 2020; (b) studies published in English, Spanish, or Portuguese; (c) studies that presented final results. The criteria for exclusion were: (a) duplicate publications; (b) studies published in other languages; (c) theoretical articles, monographs, dissertations, thesis, books, book chapters, and congress annals; (d) studies with results analysis still underway; (e) studies that do not match the defined descriptors.
The analysis of the studies retrieved was conducted by two independent evaluators, namely, the authors of this study, one a senior-year Psychology student, the other a psychologist and research professor. An initial analysis was performed based on the title, abstract, and keywords of each article retrieved, with the goal of applying the inclusion criteria described above.
The evaluators of this study examined the number and trustworthiness of the evidence presented in the articles included in this systematic review by applying the GRADE - Grades of Recommendation, Assessment, Development and Evaluation
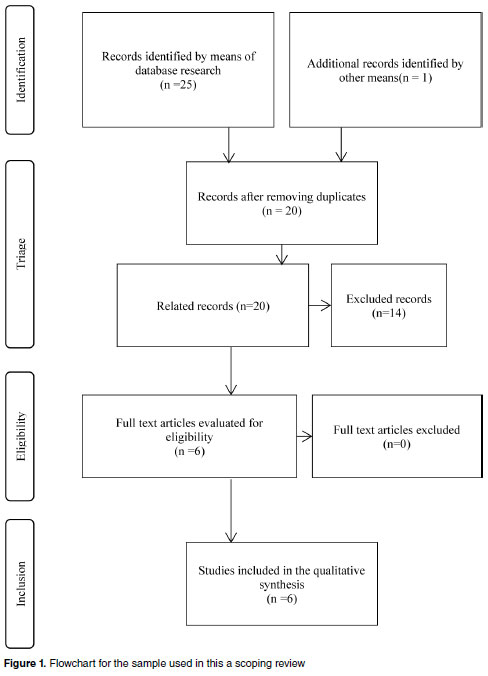
(Health Ministry, 2014). The following flowchart illustrates (figure 1) the process of selecting studies for inclusion in a scoping review.
RESULTS
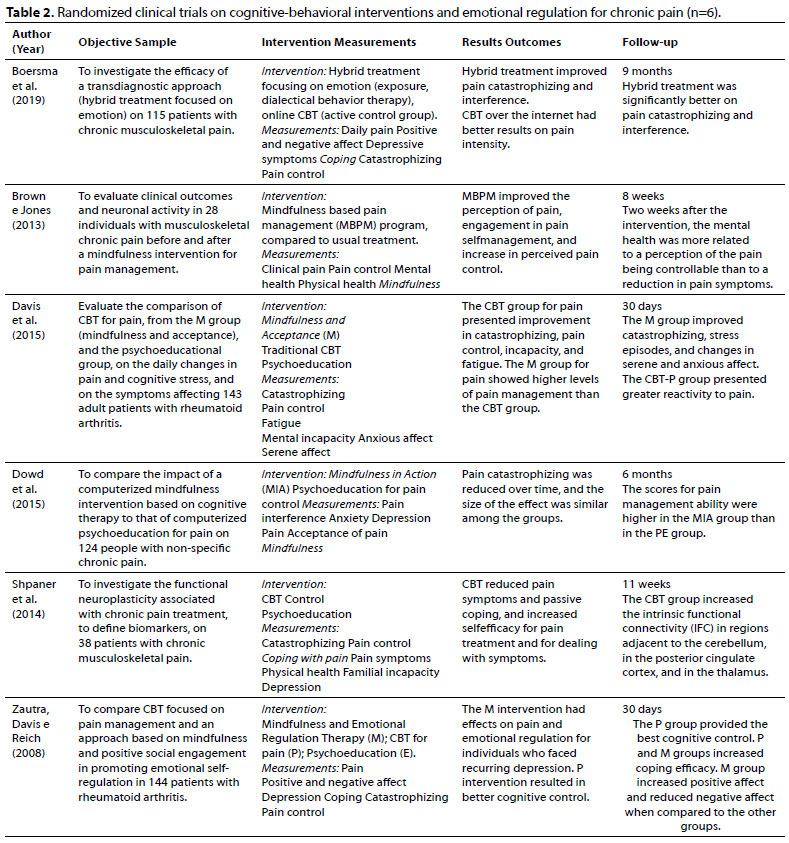
Table 2 presents the retrieved articles broaching interventions of cognitive- behavioral perspective on emotional regulation in chronic pain management in randomized clinical trials (n=6).
The articles' contents were analyzed considering their objectives, sample, measurements, internet-based and/or face-to-face interventions, and main results and follow-up based on the criterion of frequency and relevance to the objectives of this review.
DISCUSSION
Among the articles included, Shpaner et al. (2014) aimed at a better understanding of functional neuroplasticity related to management of chronic pain, and at defining biomarkers for recovery, in eleven cognitive-behavioral group therapy sessions with 38 patients presenting chronic musculoskeletal pain. Brown and Jones (2013) investigated the effects of mindfulness-based intervention, through a pain management program, on clinical outcomes and neural activity linked to cognitive control and emotional regulation on 28 individuals with chronic musculoskeletal pain.
Zautra, Davis and Reich (2008) examined the efficacy of an approach based on cognitive-behavioral methods that focused on pain management, and of another approach, based on mindfulness meditation and positive social engagement, to promote emotional regulation in the treatment of 144 patients with rheumatoid arthritis. They collected data about positive and negative affect, as well as depressive symptoms, on 30 journals.
As to the sample of studies included in this review, the most frequent types of chronic pain were chronic musculoskeletal pain (Shpaner et al., 2014; Brown & Jones, 2013; Boersma et al., 2019), and chronic rheumatoid arthritis pain (Zautra, Davis & Reich, 2008, Davis et al., 2015). Non-specific chronic pain was also found (Dowd et al., 2015).
As for the mode of intervention, two were done in an individual basis (Brown & Jones, 2013; Dowd et al., 2015), while the rest were in group. Two interventions were internet-based CBT (Boersma et al., 2019; Dowd et al., 2015). Two interventions focused directly on emotional regulation: mindfulness meditation and emotion regulation therapy (Zautra, Davis & Reich, 2008) and The Mia Intervention (Dowd et al., 2015).
Intervention M (Mindful Awareness and Acceptance Treatment) had the goal of studying the regulation and disadaptation of emotions related to chronic pain (Zautra, Davis & Reich, 2008). This same intervention, when used in Davis et al. (2015) focused on developing two skill sets: one for lessening the negative effect of pain episodes and stress on mood, symptoms, and functioning; another for enhancing positive affect involvement. In Dowd et al. (2015), The Mia Intervention is comprised of an emotional regulation program and by mindfulness meditation (MBSR), based on stress reducing factors and cognitive therapy.
The hybrid treatment focusing on emotion is grounded on principles of exposure to pain and preventive behaviors related to emotion, and uses Dialectical Behavior Therapy to address difficulties in emotional regulation and skill shortcomings (Boersna et al., 2019). The Mindfulness-Based Pain Management Program (MBPM) teaches the practice of mindfulness to reduce the reactive cycle that leads to physical and emotional stress. MBPM teaches not to try to do anything about the underlying unpleasant sensation of pain, but to train in mindfulness to lessen the reactive cycle that leads to physical and emotional stress (Brown & Jones, 2013)
The CBT treatment for pain was specifically focused on increasing pain management abilities, aiming to enhance cognitive coping and functional health, as well as restrict the fatigue symptoms of pain (Davis et al., 2015). In Zautra, Davis and Reich (2008), this same treatment includes adding pain management abilities.
CBT as used in Shpaner et al. (2014) had the main goal of altering cognition, reducing disadaptive coping, and improving the ability to use attention-diversion strategies. The CBT program given online contains modules with some specific topics, including: dealing with pain through gradual exercises, information on mindfulness, stress, pain, sleep, setbacks and maintenance planning (Boersma et al., 2019).
Another research used a psychoeducation program (Dowd et al., 2015) based on elements of pain management programs and the biopsychosocial model. This intervention contains information about activating rhythm, encouraging activity, applying cognitive behavioral skills to solve problems, and the role of useless thoughts.
One of the studies took an educational approach involving pain physiology, the vicious cycle of chronic pain, the relevance of managing stress and depression, physical activity, sleep hygiene, and healthy eating. However, this approach did not include cognitive and behavioral aspects about coping strategies (Shpaner et al., 2014).
The educational group protocol in Zautra, Davis, and Reigh (2008) had no information on coping strategies, and rather presented general information on health and medicine. In Davis et al. (2005), the educational control group provided information about pain management and stress, without employing skills to cope with the pain or with emotional difficulties.
Pain outcomes were found in every study, the most frequent being catastrophizing and pain management, followed by depressive symptoms, affection, and coping. In this review, the analysis of the results, as well as the discussion, will focus on the most frequent outcomes.
Regarding improvements related to pain, one of the studies reported a decrease in the effective classification of clinical pain, resulting from mindfulness training treatment (Brown & Jones, 2013). The average intensity of pain was lowered below the posttreatment baseline in both groups (the Mia Intervention and the Psychoeducation for pain management), but this reduction was not observed during follow-up. Interference on total pain, as well as pain acceptance and catastrophizing, improved for both groups in the pre- and post-treatment periods, and these improvements remained present during follow-up, with moderate to high variations (Dowd et al., 2015).
In Boersma et al. (2019), pain interference improved over time, and the amplitude of variation was similar for both groups (emotion-focused hybrid treatment, and internetbased CBT given online). The comparison of pre-treatment and post-treatment scores of the "outcome" variable reveals statistically significant differences between the interventions. That is, for pain intensity and catastrophizing, the hybrid treatment was favored over CBT provided online. The standardized average difference of the effects was low to moderate.
The evaluations of pain catastrophizing decreased over time, both groups showing similar decreases. Post hoc analysis showed that catastrophizing dropped between T1 (before the intervention) and T2 (after the intervention), and remained stable between T2 and T3 (6 months after the intervention). Levels of catastrophizing in T3 were expressively lower than those in T1 (Dowd et al., 2015).
The MBPM group (mindfulness-based pain management) reported a less expressive increase between pre- and post-treatment periods in catastrophizing related to a daily pain episode (Time x A Pain t = -2.91, p <0.004). In the pre- and post-treatment periods, the strength of the association between daily pain and catastrophizing decreased over time (Brown & Jones, 2013).
As for general levels of catastrophizing, the MBPM group showed an improvement in the pre- and post-treatment periods (Time t = -2.54, p <0.02) (Brown & Jones, 2013). The CBT group for pain showed improvement in general levels of catastrophizing (Time t = -3.85, p <0.0003). The E group (usual treatment) showed a worsening in general levels of catastrophizing (Time t = 2.49, p <0.02) (Davis et al., 2015).
However, there were improvements in psychological results, such as the perceived management of pain, associated with increased anticipatory processing in dorsolateral pre-frontal cortex (DLPFC), and in the somatosensory cortex. Also, alterations in neuronal activity were found, the mindfulness treatment reduced the heightened activation in the brain's central regions (especially the bilateral DLPFC) during the anticipation of acute pain, without affecting regions usually correlated with pain intensity (cingulate gyrus and posterior insula) (Brown & Jones, 2013).
In regards to pain management, the M group (Mindfulness Awareness and Acceptance Treatment) presented higher overall levels of pain management than the CBT group for pain (t (97) = 3.01, p <0.01) and the E group t (89) = 2.40, p <0.02). The CBT group for pain presented lower reductions in management of perceived pain during days of heightened pain (Time x A Pain t = 2.89, p <0.004). The CBT group for pain showed improvement in general levels of pain management (Time t = -3.85, p <0.0003). The arthritis educational control group showed an improvement in the general levels of perceived pain management (Time t = 2.47, p <0.02) (Davis et al., 2015).
In the same study as Davis et al. (2105), the M group showed improvement in the pre- and post-treatment relation between stress episodes and changes in serene affect (Time x A Stress t = 2.18, p <0.03) and anxious affect (Time x A Stress t = -2.17, p <0.03). In the overall level of serene affect, the M group showed improvement in the pre- and post-treatment periods (Time t = -5.48, p <0.0001).
The intervention based on mindfulness stands out as a solid strategy for emotions in people with signs and symptoms of recurring depression, as is evidenced by increased positive affect and decreased negative affect, when compared to CBT for pain and educational control. The mindfulness-based strategy improves emotional regulation (Zautra, Davis & Reich, 2008). The mindfulness group in Davis et al. (2015) showed improved pre- and post-treatment relations, including episodes of stress and changes in serene affect and in anxious affect.
The Mindfulness in Action (MIA) intervention showed a baseline change posttreatment in regards to the ability to manage emotions, deal with stress, and enjoy pleasant events. This effect remained throughout the six-month follow-up period of the perceptions of stress and emotion management. The Patient Impression of Change (PGIC) evaluation for the ability to manage emotions was higher in the MIA group than in the PE group in T2 (post-intervention), and this difference remained throughout T3 (6 months after the intervention) (Dowd et al., 2015).
In comparison to the educational group (usual treatment), participants in the CBT showed reduced connectivity between the DMN (default mode network) and the amigdala, the PAG (periaqueductal gray region), and the left lateral region of the occipital cortex. Stronger connectivity was seen between the basal ganglia and the right S2 (secondary right somatosensorial cortex) between pre- and post-treatment. This increased connectivity from pre- to post- treatment was correlated to a drop, in the same period, of pain symptoms and passive coping, and an increase in self-efficacy for treating pain and dealing with symptoms (Shpaner et al., 2014).
Pain management classifications are strongly infused with cognitive language, supporting types of interventions made available by CBT, as well as education programs about pain. In that sense, CBT interventions on pain have provided better cognitive control. On the other hand, meditation and mindfulness methods do not stimulate control, but awareness (Zautra, Davis & Reich, 2008). In the study by Davis et al. (2015), the CBT group showed improvement in pain management and catastrophizing, and in Zautra, Davis and Reich (2008) there was also pain control.
In the randomized clinical trial by Ganji, Pakniat, Armat, Tabatabaeichehr, and Mortazavi (2018), it was concluded that the intervention (Self-Management Group Education) conducted in six educational sessions decreased pain in elderly people with osteoarthritis. Therefore, self-management education can promote behavioral changes in pain control.
Regarding the educational control groups included in this review, one of the inperson groups showed worsened general levels of catastrophizing, but improved general levels of incapacity (Davis et al., 2015). Two others showed inferior results when compared to the respective intervention groups (Zautra, Davis & Reich, 2008; Shpaner et al., 2014). Computerized psychoeducation did not indicate significant differences in various pain measurements when compared to the intervention group (Dowd et al., 2015). The core clinical implication of the study by Dowd et al. (2015) is that it supports the viability of computerized interventions as an additional option for management of chronic pain.
In the study by Vowles, Fink, and Cohen (2014), an interdisciplinary program of rehabilitation based on Acceptance and Commitment Therapy was used, and the level of incapacity, among other clinical outcomes, was assessed. Of the patients who reported decreased effort through pain management and increased engagement in activities they value personally, over the period of the intervention (4 weeks), 80% showed a reliable drop in incapacity during the three-month follow-up.
In the study by Davis et al. (2015), the data suggest that treatment M (Mindful Awareness and Acceptance Treatment) focused on emotion regulation produces broader benefits in pain management and daily stress than those reported by the CBT group for pain, or by the educational group for arthritis. Furthermore, the M treatment showed higher general levels of pain control in relation to the CBT for pain group.
As for reduction of pain levels, the Brown and Jones (2013) study reported a drop in the scores on the Pain Catastrophizing Scale (PCS) from the baseline to the end of the treatment. This positive result reportedly remained or was further improved in the followup period for five of the six participants, having decreased for only one of them.
The study by Linton and Fruzzetti (2014) evaluated the effects of a hybrid approach that combines a treatment based on DBT (Dialectical Behavior Therapy), focused on emotions, with a control that is exposure-based. The result was the reduction in negative affect indicated by the catastrophic thought. The findings of this study support the notion that negative emotions play a relevant role in chronic pain and its treatment, as well as the idea that the goal context is important.
The results indicated an average reduction of 51% in pain intensity from pre to follow-up (Linton & Fruzzetti, 2014). In the opposite direction, the study by Dowd et al.
(2015) did not show an expressive change in average pain intensity classification. In Brown and Jones (2013), acute experimental pain classifications were not lessened by MBPM (mindfulness-based pain management) treatment, but there was a small reduction in the effective classification of clinical pain as a result of treatment.
In the study by Osborne, Jimenez-Torres, Landa, Mahoney, and Madan (2017), the pain psychotherapy group integrated aspects from acceptance and commitment therapy, cognitive-behavioral therapy, and mindfulness-based stress reduction based on mindfulness. There was a reduction in depression, anxiety, and somatic symptoms over the course of the treatment. On average, participants were admitted with high scores in the depressive symptomatology scale, but had lower scores when they were discharged. Differently from the Dowd et al. (2015) study, psychological suffering showed no change over time, and the magnitude of change did not vary per group (MIA and computerized psychoeducation).
The controlled experimental study by Zeinaly and Pourhosein (2016), evaluated the efficacy of a treatment based on emotion regulation in patients with chronic pain, and concluded that treatment strategies that have emotion regulation as a core component can reduce the level of anxiety and stress and be efficient in managing pain. In other study Osborne et al. (2017), the results demonstrated that group psychotherapy improved emotion regulation and reduced pain. Subjects also showed improved capacity of engaging in goal-driven behaviors, as well as managing impulsive responses, even if they still experienced negative emotions. The mindfulness intervention promoted emotional regulation and reduction of recurring depression (Zautra, Davis & Reich, 2008).
The randomized study by Hearn and Finlay (2018) about the computerized version of mindfulness for patients with medullary lesion demonstrated a reduction in depression and chronic pain. The online mindfulness training, compared to psychoeducation, allowed for more significant improvement in the symptoms of depression and anxiety, catastrophic thought, and specific elements of mindfulness (describing, acting with awareness, non-reactivity to inner experience, and total scores) by the end of the intervention. At follow-up, the most pronounced effect was improvement in symptoms of depression, pointing to a strong relationship between engagement in mindfulness training and improvement in this outcome.
The study by Seminowicz et al. (2013), investigated associations in the brain's gray matter after cognitive-behavioral therapy sessions in patients with chronic pain. Eleven sessions resulted in an increase in gray matter in the pre-frontal and somatosensorial regions, as well as an increase in pre-frontal dorsolateral volume, related to the reduction in pain catastrophizing. These results suggest that the gray matter can change after eleven weeks of CBT, in parallel with clinical improvements in general mental health and in coping with pain.
In that same line, the study by Shpaner et al. (2014), demonstrated that CBT, in comparison with active educational control, is linked to relevant changes in functional connectivity in a restful state, in patients with chronic pain. It was further observed that, in a CBT intervention, learning new strategies for pain management produces measurable changes in intrinsic functional connectivity (IFC) within and between networks previously involved in chronic pain.
Changes related to CBT were observed in the functional connectivity of basal ganglia (BG), and in the amplitude of intrinsic fluctuations in the cerebellum. The findings of this study suggest that CBT treatment can alter the cortico-limbic connectivity by improving cognitive and behavioral aspects. CBT intervention produced clinical improvements in anxiety, depression and chronic pain (Shpaner et al., 2014).
Conclusions reached in the study by Zautra, Davis and Reich (2008) suggest that therapists and researchers should consider including the emotional regulation process in treatment evaluation and planning. Also, emphasize the fact that therapies based on emotional regulation process can further develop the potential for increasing positive affective experience and reducing negative responses, especially for individuals with a history of depression.
CONCLUSION
The prevalent forms of chronic pain observed in this study were musculoskeletal pain and rheumatoid arthritis pain. Non-specific chronic pain, also found in the sample of this review, is now denominated musculoskeletal chronic pain, described in the primary chronic pain category according to ICD-11.
The cognitive-behavioral interventions analyzed in the studies retrieved for this review presented improvements in various chronic pain outcomes, especially catastrophizing and pain control, as well as acceptance, management, and coping. These effects were associated with improved outcomes in mental health.
Effects of CBT and mindfulness were found in neurologic structures linked to clinical variables of mental health, correlated to pain and to emotional regulation (the latter through mindfulness control). It was observed that the clinical history of recurring depression has a relevant influence in the beneficial effects (greater pain reduction), mainly through mindfulness. Additionally, half of the studies assessed strategies for coping with pain.
All studies had control groups, and a follow-up period varying from one to nine months. For control conditions, the studies used educational methods, one used regular clinical treatment, and another used online CBT as active control. Few instruments were used specifically for evaluating emotional regulation, which was verified through elements linked to the affective-emotional component of pain, such as negative and positive affect. In that sense, observed few interventions that dealt directly with emotional regulations, but rather interventions that use emotional regulation as a strategy in cognitive and behavioral approaches, such as traditional Cognitive Therapy, and in mindfulness approaches, such as Dialectical Behavioral Therapy and Acceptance Therapy, thus comprising an integrative model that focuses on the affective-emotional component of pain.
As for limitations of the studies, care should be taken not only in their interpretation, but also in applying their findings, seeing as confusing factors may be present - such as patients who were taking medication. Some authors suggest that replication of the studies may increase the reliability of the findings.
For future studies, can be suggest that follow-up periods be used to understand the potential long-term effects that internet-based mindfulness training and CBT vs. face-to- face related to cognitive control and emotional regulation. Also, in others intervention studies, the relationship between changes in process mindfulness, acceptance, and pain catastrophizing should be examined. Finally, the main effective components of internetbased CBT vs. in-person CBT must be identified to preserve the engagement of patients in treatment programs.
REFERENCES
Aldão, A. & Plate, A. (2020). Enfrentamento e regulação emocional. In: S. C. Hayes & S. G. Hofmann (Eds.). Terapia Cognitivo-comportamental baseada em processos: ciência e competências clínicas. (pp. 205-214) Porto Alegre: Artmed. [ Links ]
Andersson, G. (2020). A tecnologia da informação e o papel dinâmico da prática. In: S. C. Hayes & S. G. Hofmann (Eds.). Terapia Cognitivo-comportamental baseada em processos: ciência e competências clínicas. (pp. 53-65). Porto Alegre: Artmed. [ Links ]
Barke, A. (2019). Chronic Pain has arrived in the ICD-11. International Association for the Study of Pain. Recuperado de https://www.iasp-pain.org/PublicationsNews/NewsDetail.aspx?ItemNumber=8340&navItemNumber=643. [ Links ]
Boersma, K., Sodermark, M., Hesser, H., Flink, I. K., Gerdle, B., & Linton, S. J. (2019). Efficacy of a transdiagnostic emotion-focused exposure treatment for chronic pain patients with comorbid anxiety and depression: a randomized controlled trial. Pain, 160,1708-1718. doi: 10.1097.0000000000001575. [ Links ]
Brown, C.A, & Jones, A. K. P. (2013). Psychobiological correlates of improved mental health in patients with musculoskeletal pain after a mindfulness-based pain management program. The Clinical Journal of Pain, 29(3),233-244. doi: 10.1097/AJP.0b013e31824c5d9f. [ Links ]
Calvetti, P. U., & Segabinazzi, J. D. (2019). Avaliação psicológica da dor em pessoas adoecidas. In: Hutz, C. S. et al. (Eds.) Avaliação psicológica nos contextos de saúde e hospitalar (pp. 103-114). Porto Alegre: Artmed. [ Links ]
Crispim, I. V. R. (2015). Estilos de vinculação, regulação emocional e partilha social das emoções em estudantes universitários. Dissertação de Mestrado, Universidade Lusófona de Humanidades e Tecnologias, Lisboa. [ Links ]
Davis, M. C., Zautra, A. J., Wolf, L. D., Tennen, H., & Yeung, E. W. (2015). Mindfulness and cognitive behavioral interventions for chronic pain: differential effects on daily pain reactivity and stress reactivity. Journal of Consulting Clinical Psychology, 53(1),24-35. doi: 10.1037/a0038200. [ Links ]
Dobson, D. & Dobson, K. (2018). Evidence-based practice of cognitive-behavioral therapy. New York: The Guilford Press. [ Links ]
Dowd, H., Hogan, M. J., McGuire, B. E., Sarma, K. M., & Fish, R. A. (2015). Comparison of online mindfulness-based cognitive therapy intervention with online pain management psychoeducation: a randomized controlled pilot study. Clinical Journal of Pain, 31(6), 517-527. doi: 10.1097/AJP.0000000000000201. [ Links ]
Ehde, D. M., Dillworth, T. M., Turner, J. A. (2014). Cognitive-Behavioral Therapy for Individuals with Chronic Pain: Efficacy, Innovations and Directions for Research. American Psychologist Journal, 69(2), 153-166. doi: 10.1037/a0035747. [ Links ]
Ganji, R., Pakniat, A., Armat, M. R., Tabatabaeichehr, M., & Mortazavi, H. (2018). The effect of self-management educational program on pain intensity in elderly patients with knee osteoarthritis: a randomized clinical trial. Journal of Medical Sciences, 6(6): 1062-1066. doi: 10.3889/oamjms.2018.225. [ Links ]
Gatchel, R. J., McGeary, D. D., McGeary, C. A., Lippe, B. (2014). Interdisciplinary chronic pain management: past, presente, and future. American Psychological Association, 69(2),119-130. doi: 10.1037/a0035514. [ Links ]
Gutiérrez, R. M. V., & Munoz-Martínez, A. M. (2013). La regulación emocional: Precisiones y avances conceptuales desde la perspectiva conductual. Psicologia USP, 24(2),225-240. doi: 10.1590/S0103-65642013000200003. [ Links ]
Hearn, J. H., & Finlay, K. A. (2018). Internet-delivered mindfulness for people with depression and chronic pain following spinal cord injury: a randomized, controlled feasibility trial. Spinal Cord, 56(8),750-761. doi: 10.1038/s41393-018-0090-2. [ Links ]
Leahy, R. L. (2013). Regulação emocional em psicoterapia: um guia para o terapeuta cognitivo-comportamental. Porto Alegre: Artmed. [ Links ]
Linton, S. J., & Fruzzetti, A. E. (2014). A hybrid emotion-focused exposure treatment for chronic pain: a feasibility study. Scandinavian Journal of Pain, 5,151-158. doi: 10.1016/j.sjpain.2014.05.005. [ Links ]
Ministério da Saúde. (2014). Diretrizes metodológicas: Sistema GRADE: Manual de graduação da qualidade da evidência e força de recomendação para tomada de decisão em saúde. Brasília: Ministério da Saúde. Recuperado de https://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_metodologicas_sistema_gra de.pdf [ Links ]
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., Shekelle, P., & Stewart, L. A. (2015). Preferred reporting items for systematic review and metaanalysis protocols (PRISMA-P) 2015 statement. Systematic Reviews, 4(1). doi: 10.1186/2046-4053-4-1. [ Links ]
Osborne, P. J., Jimenez-Torres, G. J., Landa, Y., Mahoney, J., & Madan, A. (2017). Chronic pain management group psychotherapy for psychiatric inpatients: a pilot study. Bulletin of the Menninger Clinic, 81(2), 123-149. doi: 10.1521/bumc.2017.81.2.123. [ Links ]
Seminovicz, D. A., Shpaner, M., Keaser, M. L., Krauthamer, G. M., Mantegna, J., Dumas, J. A., Newhouse, P. A., Filippi, C., Keefe, F.J., Naylor, M. R. (2013). Cognitive behavioral therapy increases prefontal cortex gray matter in patients with chronic pain. Pain, 14(12). doi:10.1016/j.jpain.2013.07.020. [ Links ]
Shpaner, M., Kelly, C., Lieberman, G., Parelman, H., Davis, M., Keefe, F. J., & Naylor, M. R. (2014). Unlearning chronic pain: a randomized controlled trial to investigate changes in intrinsic brain connectivity following Cognitive Behavioral Therapy. Neuroimage Clinical, 5,365-376. doi: 10.1016/j.nicl.2014.07.008. [ Links ]
Santos, V., Zortea, M., Alves, R. L., Naziazeno, C., Saldanha, J. S., Carvalho, S., Leite, A., Torres, I., Souza, A., Calvetti, P. U., Fregni, F., & Caumo, W. (2018). Cognitive effects of transcranial direct current stimulation combined with working memory training in fibromyalgia: a randomized clinical trial. Scientific reports, S(1),12477. https://doi.org/10.1038/s41598-018-30127-z [ Links ]
Thorn, B. E. (2017). Cognitive therapy for chronic pain: a step-by-step guide. New York: The Guilford Press. [ Links ]
Treede, R. F., Rief, W., Barke, A., Aziz, Q., Bennett, M. I., Benoliel, R., Cohen, M., Evers, S., Finnerup, N. B., First, M. B., Giamberardino, M. A., Kaasa, S., Kosek, E., Lavand'homme, P., Nicholas, M., Perrot, S., Scholz, J., Schug, S., Smith, B. H., Svensson, P., Vlaeyen, J. W. S., Wang, S. J. (2015). A classification of chronic pain for ICD-11. The Journal of the International Association for the Study of Pain, 156(6). 1003-1007. https://doi.org/10.1097/_j.pain.0000000000000160 [ Links ]
Vowles, K. E., Fink, B. C. & Cohen, L. L. (2014). Acceptance and commitment therapy for chronic pain: a diary study of treatment process in relation to reliable change in disability. Journal of Contextual Behavioral Science, 3(2): 74-80. doi:10.1016/j. jcbs.2014.04.003. [ Links ]
World Health Organization (2022). International Classification of Diseases (ICD) 11th Revision. Recuperado de https://www.who.int/standards/classifications/classification-of-diseases# [ Links ]
Zautra, A. J., Davis, M. C., & Reich, J. W. (2008). Comparison of Cognitive Behavioral and Mindfulness meditation interventions on adaptation to rheumatoid arthrits for patients with and without history of recurrent depression. Journal of Consulting and Clinical Psychology, 76(3),408-421. doi: 10.1037/0022-006X.76.3.408. [ Links ]
Zeinali, F. & Pourhosein, R. (2016). Effectiveness of treatment base on emotional regulation in reducing chronic pain of patients who suffer from chronic pain. Online International Journal, 6 (S2),315-321. [ Links ]
Este artigo foi submetido no SGP (Sistema de Gestão de Publicações) da RBTC em 19 de Agosto de 2021. cod. 243 Correspondence:
Correspondence:
Prisla Ücker Calvetti
E-mail: prisla.calvetti@gmail.com
Artigo aceito em 10 de Janeiro de 2022


{kind=link}
{kind=link}
{kind=link}