










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Compartir

 Permalink
PermalinkArquivos Brasileiros de Psicologia
versión On-line ISSN 1809-5267
Arq. bras. psicol. vol.73 no.2 Rio de Janeiro mayo/ago. 2021
http://dx.doi.org/10.36482/1809-5267.ARBP2021v73i2p.112-127
ARTIGOS
Construction and Validation of Social Anxiety Disorder Exposure and Evaluation Scale - SADEE
Construcción y validación del Social Anxiety Disorder Exposure and Evaluation Scale - SADEE
Construção e validação da Social Anxiety Disorder Exposure and Evaluation Scale - SADEE
Cybele Perciano CyprianoI; Irismar Reis de OliveiraII
IMestranda. Programa de Pós-Graduação em Processos Interativos dos Órgãos e Sistemas (PPGPIOS). Universidade Federal da Bahia (UFBA). Salvador. Estado da Bahia. Brasil. https://orcid.org/0000-0003-4997-8635
IIProfessor Titular. Programa de Pós-Graduação em Processos Interativos dos Órgãos e Sistemas (PPGPIOS). Universidade Federal da Bahia (UFBA). Salvador. Estado da Bahia. Brasil. https://orcid.org/0000-0002-9680-9247
ABSTRACT
In the cases of Social Anxiety Disorder (SAD), treatment dropout is a frequent problem, which demands the development of instruments that enable treatment compliance. The present paper deals with the construction and validation of the Social Anxiety Disorder Exposure and Evaluation Scale (SADEE). The number of participants in the study was N = 407 responders of both genders. The process of content validity first led to the modification of problematic items. The construct validity was investigated by both exploratory factor analysis and confirmatory factor analysis, with the objective of estimating a unidimensional measure. The final adjustment obtained was that CFI = .99; TLI = .98; RMSEA = .04; SRMR = .07; χ2 /gl = 1.70. SADEE presented high correlation with the Liebowitz Social Anxiety Scale and high reliability. The conclusion was that SADEE showed satisfactory evidence of construct and concurrent validity, internal consistency and test-retest reliability.
Keywords: Social Anxiety Disorder; Cognitive Behavioral Therapy; Psychometrics; Validity; Psychological Assessment.
RESUMEN
La evasión del tratamiento es un problema frecuente en los casos de Trastorno de Ansiedad Social, lo que demanda la construcción de instrumentos que faciliten la adhesión al tratamiento. El objetivo del presente artículo es la construcción y validación del Social Anxiety Disorder Exposure and Evaluation Scale (SADEE). Participaron de la investigación N = 407 respondientes de ambos sexos. El proceso de validez del contenido llevó a la modificación de ítems problemáticos. La validez del constructo fue investigada por procedimientos de análisis factorial exploratorio y confirmatorio, con el objetivo de estimar una medida unidimensional. El ajuste final obtenido fue de CFI = 0,99; TLI = 0,98; RMSEA = 0,04; SRMR = 0,07; χ2 /gl = 1.70. Se obtuvo alta correlación con la escala de fobia social de Liebowitz y alta fiabilidad. La SADEE presentó evidencias satisfactorias de validez de constructo, concurrente, consistencia interna y la prueba y re-evaluación.
Palabras clave: Trastorno de Ansiedad Social; Terapia Cognitivo-Comportamental; Psicometría; Validez; Evaluación Psicológica.
RESUMO
Nos casos de Transtorno de Ansiedade Social (TAS), o abandono do tratamento é um problema frequente, que exige o desenvolvimento de instrumentos que possibilitem a adesão ao tratamento. O objetivo do presente artigo é a construção e validação da Escala de Exposição e Avaliação de Transtornos de Ansiedade Social (SADEE). O número de participantes do estudo foi N = 407 respondentes de ambos os sexos. O processo de validade do conteúdo levou primeiro à modificação de itens problemáticos. A validade do construto foi investigada tanto pela análise fatorial exploratória quanto pela confirmatória, com o objetivo de estimar uma medida unidimensional. O ajuste final obtido foi aquele CFI = 0,99; TLI = 0,98; RMSEA = 0,04; SRMR = 0,07; χ2 / gl = 1,70. A SADEE apresentou alta correlação com a Escala de Ansiedade Social de Liebowitz e alta confiabilidade. A conclusão foi que a SADEE mostrou evidência satisfatória de validade construtiva e concorrente, consistência interna e confiabilidade teste-reteste.
Palavras-chave: Transtorno de Ansiedade Social; Terapia Cognitiva Comportamental; Psicometria; Validade; Avaliação Psicológica.
Introdução
Anxiety is a natural and useful reaction to protect the human being from and/or adapt to certain situations. Its purpose is to protect the survival of the species (Leahy, 2020). Anxiety is characterized as pathological when presented on a generalized and extreme level, causing a negative impact on the individual's quality of life. Its focus is on an emotion directed at the future, and therefore at something which has not yet happened, in a pessimistic and catastrophic perspective (Hofmann & DiBartolo, 2014).
Pathological anxiety is an emotional response that is broader and more subjective than fear; where fear evokes said anxiety and is perceived as highly aversive by the person who suffers from it, for he/she considers it unpredictable and uncontrollable. Anxiety is composed of cognitive, affective, physiological and behavioral responses, concomitant and complex, which contribute to great suffering, as well as to avoidance of behaviors that are used to cope with situations seen as risky (Clark, D. & Beck, A, 2011).
Social Anxiety Disorder (SAD) is described as intense, painful, and debilitating fear or anxiety of being condemned, rejected and humiliated in social interactions or activities, where the individual is exposed to situations that make him/her feel vulnerable to criticism, judgment and negative evaluation from others. Someone with SAD recognizes this attitude as irrational but feels incapable of effectively reacting to the situation (Caballo et al., 2011; Levitan et al., 2015a). SAD causes intense and generalized impairment in social environments, with adverse consequences in every segment of the individual's life, such as general well-being, leisure activities, school work, level of employability, productivity, socioeconomic level, interpersonal relationships, and building a family nucleus (Leahy, 2020).
The defense mechanism most adopted by individuals with SAD is avoidance behavior, thought to perpetuate the disorder. Exposure technique, which works at eliminating such behavior, is of utmost importance in clinical intervention (Turner & Beidel, 1989). Due to the difficulties in implementing this technique and the high rates of treatment dropout, existing opportunities were sought after that would enhance the classic treatment of SAD within the framework of Cognitive Behavioral Therapy (CBT). The purpose was to contribute toward an improvement in the treatment and handling of Social Phobia (SP).
SAD was recognized as a pathology from the 1980 publication of the DSM-3, where it was called Social Phobia. With the publication of the DSM-5 in 2013, it came to be known as Social Anxiety Disorder (SAD) (Liebowitz et al., 1985). This disorder has undergone the least research, besides being, for many years, the least understood (Herbert, J. D et al., 1992; Turner & Beidel, 1989). Until the mid-1980s, social phobia episodes were described in the field of psychology as pathological shyness, date/meeting anxiety and even insecurity (Margis et al., 2003). The scientific community delayed in recognizing the disorder due to several intervening factors that caused the postponement, such as the fact that SAD is many times considered secondary to the presence of comorbidities; the coping strategies that the individual with SAD employs may be confused with their lifestyle; their aversion of interacting with strangers, including the psychotherapist; the belief that no treatment exists; the universal character of the experiences entailing social anxiety, as well as the tendency of confusing SAD with shyness, which causes those suffering from SAD not to seek treatment. Unfortunately, some of these conditions still exist to this day (American Psychiatric Association, 2013; Caballo et al., 2011).
The symptoms of SAD may include extreme tension, paralysis, obsessive worry over social interactions, isolation and loneliness, besides the physiological symptoms such as blushing, shaking, tachycardia, dizziness, tingling, nausea, etc. (Barlow, 2014). SAD causes generalized and quite intense impairment in the person's social coexistence, with adverse consequences in all the segments of his/her life, like their general well-being, leisure activities, education, level of employability, productivity, socioeconomic level, interpersonal relationships and building a family nucleus (Heimberg et al., 1995; Levitan et al., 2015b; Rapee & Spence, 2004). The most common social situations that trigger symptoms and that were considered in the development of the SADEE are: going to social events; speaking in public; setting dates or meetings; initiating and sustaining verbal communication; voicing an opinion; speaking on the phone; exercising authority; using public restrooms; returning purchased products; being observed; making visual contact with strangers; eating in public; giving and receiving compliments; participating in any event with many people involved; and being the center of attention (American Psychiatric Association, 2013).
SAD is considered the most common among the anxiety disorders and the third most prevalent among all the mental disorders. The prevalence is of 7.9% in the previous 12 months and 13.3% over the lifetime (Clark, D. & Beck, A, 2011). Without adequate treatment, the disorder may intensify over time (Levitan et al., 2015b). Between 10% and 15% of affected children have a history of expressing irritation as babies, and, hypothetically, because of this, they can later show behavioral inhibition, growing more careful and quieter, besides being introverted, during the school years (Leahy, 2020). Studies suggest that the parents of individuals with avoidance behavior are more recriminating and intolerant and/or overprotective, abusive, controlling, very overly critical and somewhat discouraging, which might contribute to the development of SAD (Oliva, 2015). Also, there is evidence that the increase of sensitivity to scrutiny and criticism are transmitted from generation to generation, thus causing the individual to be predisposed to having SAD. In addition, there are signs that family members of inhibited children have high rates of social anxiety; as well as signs that parents who have the disorder, and other family members with other types of anxiety, all contribute to the development of the pathology. In the same way, studies show that low levels of extroversion and high levels of emotional instability are also indicators of genetic risk for social anxiety (Clark, D. & Beck, A, 2011; Rapee & Spence, 2004; Santos, 2012).
The evaluation of SAD must be structured, highlighting the cognitive, behavioral and physiological symptoms, as well as the reactions to them, besides determining the degree to which such symptoms interfere in the subject's daily life. It is also important to establish the factors that maintain them, which are generally cognitions and safety behaviors, mainly represented by avoidance behavior. In addition, it is fundamental that the individual become aware of subtle safety behaviors that are used but not consciously perceived (Levitan, M. et al., 2015b). Several authors suggest that different assessment instruments of SAD be used, such as semi-structured interviews, self-information instruments, self-report tools, behavior measures, as well as the use of instruments to practice social abilities (Caballo, V et al., 2011). Within this context, the Liebowitz Social Anxiety Scale (LSAS) is considered the gold standard to evaluate SAD; there are 24 items that evaluate emotional symptoms of fear or anxiety, in addition to symptoms of avoidance behaviors (Liebowitz et al., 1985).
The cognitive behavioral treatment of SAD is made up of strategies of psycho-education, practicing progressive muscle relaxation, practicing social abilities, imaginary and actual exposure to anxiety-inducing situations, bio-feedback and cognitive restructuring. The exposure technique, one of the focal points of this study, has the goal of differentiating facts from cognitive distortions, as well as developing the sense of security, self-confidence, and motivation, which are all necessary for healthy social interactions (Levitan et al., 2015b). Treatment abandonment of SAD is significant due to the fear of socially exposing oneself caused by insecurity and distrust regarding the possibility of suffering at the time of applying such technique, stemming from the fear that his/her threshold of suffering will not be respected. Cognitive distortions are mistakes in interpreting reality, to the detriment of the facts (Burato et al., 2009).
As far as the disorder's pharmacological treatment, studies show evidence that some individuals who suffer from SAD have a deficient serotonergic system, where serotonin plays an important role in mediating stress and in managing aversive situations. There are also signs that levels of dopamine, the neurotransmitter associated with motivation and seeking gratification, are reduced in some patients. Therefore, there is likely a biochemical substrate in social anxiety, with the most important one being the hyperfunctioning of the amygdala, the area of the brain responsible for the conditioning of fear. Experiencing social situations and simultaneously suffering some type of embarrassment entails awareness of fear to which some people are more predisposed than others. This pairing has to do with the origin of SAD, post-traumatic stress and other kinds of anxiety. Medications such as antidepressants and anxiolytics may be necessary to control the excess of emotional reactivity and anxiety (Levitan, M. et al., 2015b; Nardi et al., 2013).
Trial-based Cognitive Therapy (TBCT), for which the "list of items for exposure" was developed in treating SAD, and which gave origin to the SADEE, is considered a third wave therapy of Cognitive Therapy and was inspired by Franz Kafka's novel "The Trial." It is based on the presupposition that self-accusations correspond to one's core beliefs. TBCT has a seven-step structured approach, where the therapist uses a worksheet with seven columns to guide the patient during the role-playing of a courtroom trial. In this trial, the patient plays the role of defendant, prosecutor, defense attorney and jurors in order to find evidence for and against his/her self-accusations. By means of the trial, initially an investigation is conducted where the patients become aware of their self-accusations. Afterward, the procedure promotes the cognitive restructuring in the 3 levels of conceptualization automatic thoughts, underlying beliefs and core beliefs. This model uses different cognitive-behavioral techniques, such as analyzing the evidence, downward arrow and empty chair (Oliveira, 2014). TBCT has demonstrated its efficacy in social anxiety as well as in a variety of psychiatric diagnoses.
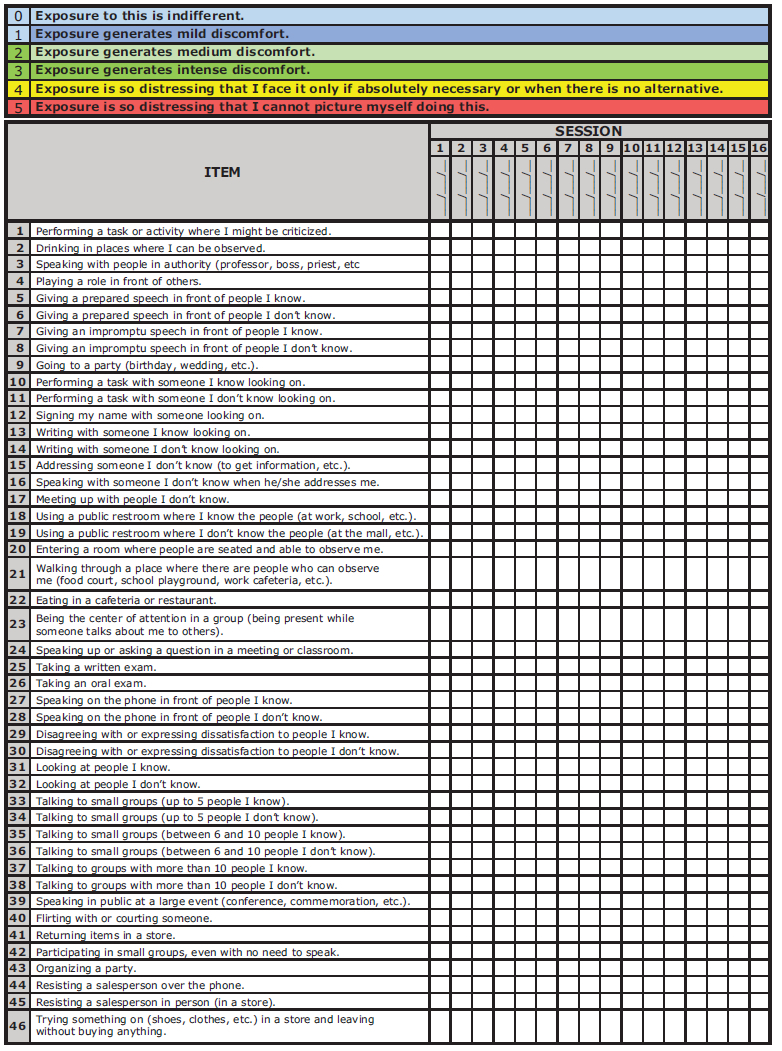
In search of other mechanisms that could improve the treatment of SAD and minimize the abandonment of the intervention, the creator of TBCT, before planning the exposure technique, proceeded to thoroughly investigate the relevant details of each theme, specifically for individual looking more precisely for the "what," "how," "when," "where," and "how intensely" each was affected in social situations. Subjectivity of individuals was brought to light. From the data collected in this procedure, a "list of items for exposure in social phobia" was created, which is part of the reatment protocol of Trial-Based Cognitive Therapy (TBCT); which was, in the present study, transformed into the SADEE (Appendix 1), in order to have its psychometric potential evaluated.
The aforementioned list of items for exposure in social phobia was based on existing scales to assess SAD (which will be cited in Methods. Starting with the need to verify the psychometric potential of such a list, the operational version of the SADEE was created (Appendix 1) with the intention of also incorporating differentials in order to enable greater treatment compliance: 1) response caption with six qualitative descriptions; 2) response caption in color; 3) more detailed item description; 4) global score results of all the items (vertically) of each evaluation; 5) score results by item (horizontally) of all the evaluations. With this framework in mind, the purpose of the current paper is to present the steps of creating SADEE.
The process of creation includes the problems with content validity, construct validity by way of factor proceedings, concurrent validity, and ultimately an analysis of internal consistency of the instrument after the elimination of items that were potentially problematic for the measure. The evidence is seen as a crucial initial step for the use of the scale in the clinical context, besides offering a basis for future studies to formulate normative tables.
Method
Participants
The first data collection (test) occurred between 01/15 and 03/30/2018 with a total n = 407 participants. The second data collection (retest) was carried out between 04/26 and 06/30/2018 with a total of n = 113. The sample comprised individuals between the ages of 18 and 60 years. There was significant difference on gender, with 83.04% of the responders being female; and, also, as to level of education, with 90.41% having college degrees. Furthermore, 75.5% of the participants are from the state of Bahia.
Instruments
In order to validate the content of the SADEE, a protocol was developed so that three raters, specialists in social phobia, would assess the clarity of the task instruction, the clarity of the wording of the items, as well as the need for examples in the SADEE items. Regarding the level of suitability, the evaluators could attribute a value of "0"- inadequate item to "2"- adequate item.
In order to investigate other psychometric features of the SADEE, the following instruments were administered during the study: (1) a sociodemographic questionnaire with information regarding gender, age, schooling, income, among other information from the participants, for sample characterization; (2) SADEE in the form of 60 items, with answers in Likert format of 6 points with describers that indicate the level of discomfort felt from the action or situation described by the item; (3) Liebowitz Social Anxiety Scale (LSAS), to facilitate the analysis of the concurrent criterion validity, as this scale is considered the gold standard to assess social anxiety.
Development of SADEE
The primary version of SADEE is composed of sixty items, inspired by the Social Phobia and Anxiety Inventory - SPAI, the Liebowitz Social Anxiety Scale - LSAS, the Fear of Negative Evaluation - FNE, and the Social Phobia Inventory - SPIN.
Due to the difficulty that an anxious individual usually feels when answering an anxiety scale, the main purpose in the item description of SADEE was to explain very thoroughly the different details and/or circumstances that cause discomfort provoked by each stimulus (item) of the scale. The response scale is the six-point Likert format, so that there are clearer and more specific options for the intensity of anxiety described in each item. Descriptors are used to indicate the level of discomfort or distress. The color identification aims to facilitate the relation of the item with the level of subjective intensity of each discomfort or distress in question.
Upon planning the use of the exposure technique, one expects the therapist to take into account the level of discomfort the responder feels in relation to the item contents (Levitan et al., 2015a). The two options on the scale classified as blue in the caption (points 0 and 1) should not be included in the exposure planning because they do not signal any social anxiety and are well tolerated by the individual. The options in green (points 2 and 3), indicating discomfort, are the ones to be considered when planning the initial exposure; although they cause avoidance behavior, they do not impede the individual from being exposed to them. The items classified as yellow and red (points 4 and 5), which generate distress, should be excluded from the initial planning until they drop in intensity and the patient considers them as green (discomfort), and then included in the therapy, with the assistance of the therapist. It is worth noting that TBCT has a technique called "consensual role-play," devised to facilitate exposure to items with a value of 4 and 5 (yellow and red) in the response scale, without causing the patient to feel pressured into doing it. In assessing the results, two types of outcomes are possible: the global score of the level of social anxiety and the score per item on the scale. Not utilizing factorial scores, produced by an estimate of the parameters, was chosen in order to simplify the use of the scale on paper. The global score of the responder may be obtained through the sum of the results of all the items in the same column, which refer to a certain evaluation.
Procedures
The study was administered on an electronic platform (SurveyMonkey), in order to reach participants from the general population in different states of Brazil, with the intent to widen the sample variability. Dissemination was conducted on social media platforms like Facebook, Instagram, LinkedIn and email. Different online invitations were sent for test and retest.
The responders spontaneously filled out the survey form after receiving the invitation with a link to the study questionnaire, sent by the researcher to potential participants, allegedly from the general population.
Data analysis
The data was analyzed under R v.3.5.1 (The R Foundation, 2018). Among the packages utilized for this study were psych (Revelle, 2011) and lavaan (Rosseel et al., 2017). Content validity coefficient (CVC) was estimated in order to verify the quality of the items. The criterion of coefficients higher than .80 was used to obtain content validity, according to recommendations from Filgueiras et al. (2015). Items with lower values were not eliminated but rather altered according to the raters' recommendations.
The Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) procedures were conducted according to Brown's (2015) recommendations. The EFA model was executed by the principal axis factoring extraction method, while the CFA was estimated by the DWLS method. The quality of factor loadings was evaluated considering 0.30 as the minimum value. From the viewpoint of structural adjustment indexes, the following indexes and criteria were employed: CFI (> .90); TLI (> .90); RMSEA (< .08); SRMR (< .08); and χ2/gl (< 5.00). In order to verify the concurrent validity between SADEE and LSAS, correlation coefficients were estimated between the scores produced by each measure.
Finally, reliability was analyzed via internal consistency method, using McDonald's omega coefficient to estimate the composite reliability. The recommended criteria of .70 was used for the desired consistency. To analyze temporal stability, or test-retest, Pearson correlation coefficient was estimated for the scores obtained at both times of administration - initial and posterior.
Ethical Considerations
Prior to its application, the current study was submitted for evaluation under the Ethics Committee for Research with Human Beings at the Institute of Health Sciences of the Federal University of Bahia, and was granted approval (CAAE - 73239317.2.0000.5662).
Results
Evidences of validity
To assess content validity, procedures were conducted by obtaining a coefficient of content validity (cvc), which is calculated as and through an agreement procedure on the quality of the scale items (Hernandez-Nieto, 2002). Individual item cvc was calculated as a reason of the average of the evaluations for the adequacy of the item over the maximum value that could be attributed (cvci), which produces a value range from 0-1. Coefficient was also estimated to every judge (cvcj), while the scale cvc was estimated by subtracting the standard error from the polarization of judges from the average of the cvcs provided by every judge (Pe) (cvc) - standard error is calculated as, given that Nj is the number of judges. Hernandez-Nieto (2002) indicates that cvc should be above .80 for the three scenarios. The content validity coefficient, as to item clarity, was .91, indicating good overall quality, but nine items included change recommendations within the comments. Item 4 was the only item that achieved a poor individual cvc of .50. The item was not removed, but modified for further use according to recommendations. Judges varied in cvc from the lowest value of .88 to .98. Overall, as values for judgements varied from 0-2, the cvcs also tended to vary little in terms of value. It was pointed out that five items needed examples. The items indicated by at least two raters as needing examples were considered a relevant necessity. Reformulations were administered according to the specific demands of the raters.
At the beginning of testing the sample's goodness of fit, the Kaiser-Meyer-Olkin (KMO) suitability factor was used, whose value should be above .70. For the data represented in this study, the results indicated that the sample is suitable for EFA, for KMO = .95. Bartlett's sphericity test, expected to be significant in large sample sizes, was conducted to check whether the correlation matrix is an identity matrix, where all the items are not correlated. A significant test indicates that the correlation matrix may be analyzed by the EFA procedure. The last assumption, indicating that the determinant of the data matrix should be different from zero, was also tested successfully. The results showed that the data are suitable for factor analysis procedures (Hair et al., 2018).
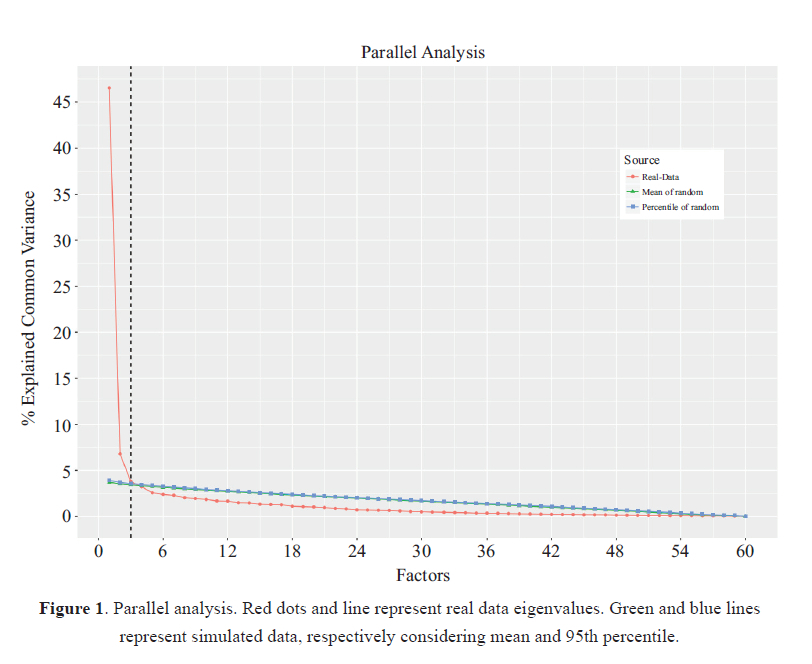
One of the preliminary steps for applying factor procedures goes through the number of factors that the data variance allows to retain. SADEE's dimensionality was studied by way of parallel analysis of its components. The option for parallel analysis involves a frequent position in the literature on how the criterion of eigenvalues higher than 1.00 comprises a strategy that may foster a suggestion of inflated retention. On the other hand, the parallel analysis allows for greater accuracy in the retention process, whereas a direct analysis of the screeplot's elbow was also employed (Figure 1). Thus, the parallel analysis, especially considering the simulations, points to the retention of three dimensions, but there is a sharp distinction between the first two factors, indicating sufficient retention only of the first factor through a graph analysis (Raiche et al., 2013).
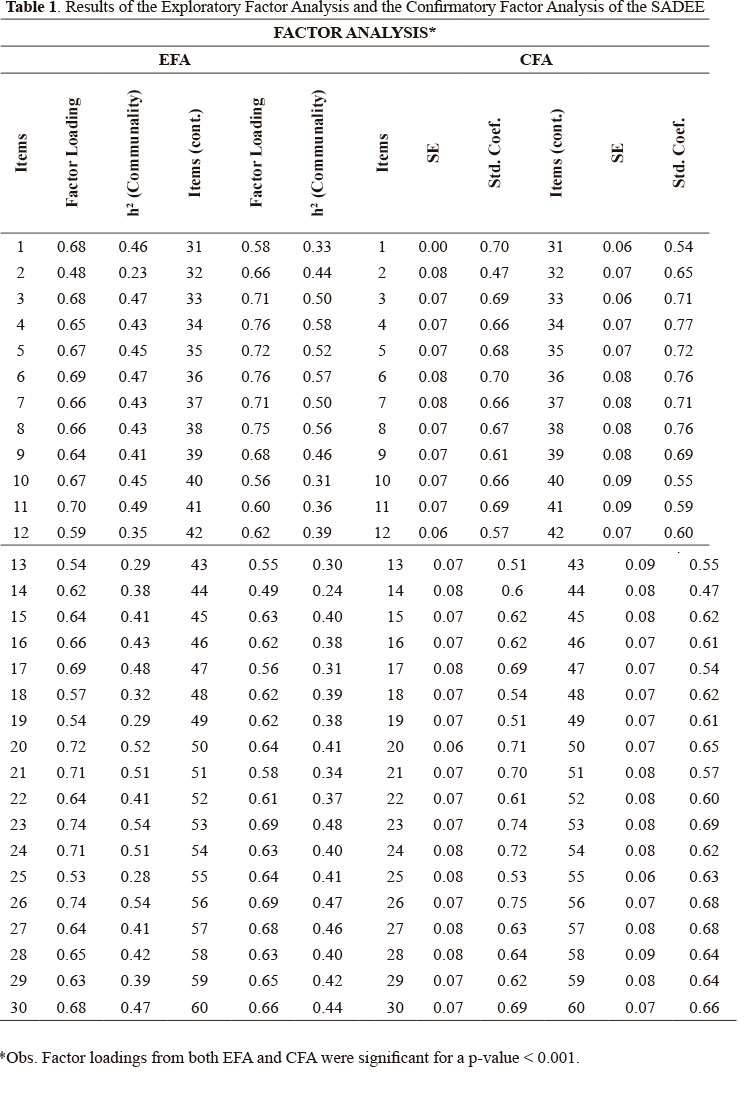
The explained variance ratio of SADEE was 46.55% for a unidimensional factor structure. The result of the EFA may be examined in Table 1. All the items showed item-total correlation of at least .47, higher than the criterion of .30 normally considered in the literature. Specifically considering the EFA, the commonalities (h2) presented five items with values lower than those recommended - items 2, 13, 19, 25 and 44. Despite the commonality (h2) problems, the same items presented factor loads greater than .30, indicating that despite the common variance, the items with low commonality still have a minimally satisfactory relation of representation with the factor. It is noteworthy that the items with greater factor load or capacity of representation were items 23, 26, 34, 36 and 38. Finally, one may affirm that the items presented indicators that support the evidence of good quality representation of the latent trait.
After the EFA, the confirmatory procedure was carried out with the objective of obtaining more information of adjustment of the instrument's structure. One important limitation is that cross-validation, by conducting both analysis with different samples, was not feasible due to the amount of items, but will be conducted in the future. The indexes used in the CFA and its respective results were: Comparative Fit Index (CFI) = .99; Tucker Lewis Index (TLI) = .98; Root Mean Square Error of Approximation (RMSEA) = .04; Standardized Root Mean Square Residual (SRMR) = .07; χ2 (Chi-Squared) = 2,900 and Degrees of Freedom = 1,710.
The obtained adjustment indexes support that the unidimensional structure offers a satisfactory approximation between the observed variance and the one estimated by the model. Still, one should point out that the Chi-Squared test was significant. However, the ratio with the degrees of freedom points to a satisfactory value of 1.70. Associative links were not employed between the item mistakes.
Concurrent Criterion Validity
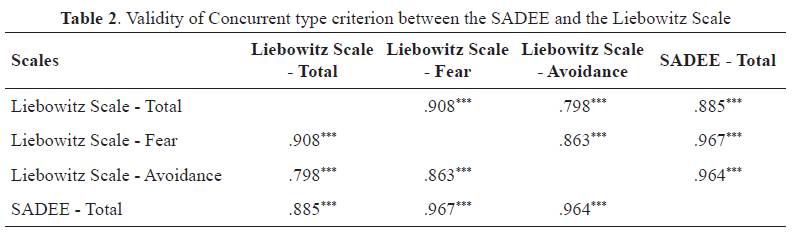
The results of the concurrent criterion validity between the SADEE and the Liebowitz Social Anxiety Scale may be found in Table 2. The matrix of correlations between the instruments and their respective dimensions showed positive results and of elevated magnitude. The lowest correlation of the SADEE with the Liebowitz scale was regarding the total score, presenting a value of .89.
Reliability
The result of the SADEE internal consistency was one omega = .97, with confidence interval of 95% that is between [.97, .98] for Cronbach's alpha coefficient. Besides the internal consistency, the result of the test-retest procedure shows a high correlation (.90) between the scores produced at both times of testing (p < .001/N = 113).
Discussion
The results indicated that the sample was adequate for the present study, despite showing a bias in the variable gender, which is of great importance on the incidence of SAD (MacKenzie & Fowler, 2013; Rodebaugh et al., 2012), as well as a bias in the income range and level of education. Such sample inconsistency may be circumvented by continuing studies regarding SADEE, which foresee recurrent data collection.
The development of a psychometric instrument capable of offering an assessment of social anxiety disorder is a crucial event, seeing the striking difficulty of diagnosing the disorder when one considers how hard it is to elaborate other objective indicators (e.g., imaging tests, biomarkers). Thus, it is essential to present psychometric data on characteristics such as validity, reliability, among others (Bilsker & Goldner, 2000). Furthermore, although the translation and adaptation of international instruments in the field of mental health for the Brazilian population is increasing and allows the benefits of transcultural comparisons, it is important that Brazilian instruments be developed for the assessment and clinical follow-up of mental disorders (Santos, 2012).
The results obtained for the content validity were favorable overall, despite leading to an elevated number of instrument corrections. When analyzing the need to show examples for the instrument's items, only five items indicated such a need. The obtained outcomes resulted in the modifications of the description of the SADEE items. Considering the construct validity, the first study of the dimensionality of the initial version of SADEE was carried out through the parallel analysis of its components. It was possible to observe from the results that up to two dimensions could be extracted through EFA. However, it is also noteworthy that a good part of the scale's variability is explained by a single factor. To guarantee the SADEE factors' interpretability in this initial phase of the instrument's analyses, unidimensionality of the scale was chosen. As one can see in the results, not one of the items presented factor load below the cut-off point of .30.
Confirmatory Factor Analysis was conducted to test the factor structure that was found. A model was specified considering the items as indicators and the factor as latent variables. In order to estimate the model parameters, the Diagonally Weighted Least Squares (DWLS) was used as the estimation method. This model was chosen because it is suitable for data that present slight asymmetry and are ordinal, as in the case of the data resulting from administering the SADEE. The results indicate that the unidimensional model conforms to the data. This aspect was also corroborated by the adjustment indexes, which showed that the solution is parsimonious and presents good adjustment to the empirical data. The ratio between Chi-squared and degrees of freedom is less than 2, indicating that there is little discrepancy between the model and the data (Schreiber et al., 2006). It is worth mentioning that according to the factor loads, items 23, 26, 34, 36 and 38 showed higher power of representation, most likely due to representing, clinically, the topics that most often act as triggers for social anxiety (Hofmann & DiBartolo, 2014).
To go beyond a valid internal structure, SADEE presented good criterion validity indexes concurrent with the Liebowitz Social Anxiety Scale, considered the gold standard in evaluating social anxiety (Santos, 2012). Regarding reliability, the internal consistency showed that it supports forming scores from the items of the scale; also, the test-retest denoted high correlation between the two times of application, which meets the theoretical expectations.
Some limitations were observed in the present study. First, the sample size was smaller than what is usually recommended - a ratio of 10 participants per item. On the other hand, a unidimensional structure presents a lower demand for investigating variance. The second limitation was the test-retest collection, which presented a technical bias because the responders did not identify themselves adequately. This generated a significant loss of the sample. Nonetheless, even with a small sample of n = 113, the correlation was elevated, showing high reliability. Future studies should also have a larger sample size, since, for this study, the participants can be characterized predominantly as females with higher levels of education.
Another final piece of information comprises the need for the scale assessment to consider a clinical sample for comparison, as well. The primary objective of the instrument is to serve as a facilitative tool for SAD patients undergoing treatment. Such an objective demands primarily that the SADEE be able to distinguish between responders with subclinical characteristics and those who have the disorder. Future studies should also include an investigation by way of the Receiver-Operating Characteristic (ROC) paradigm, with the aim of including cut-off points for using the scale.
References
American Psychiatric Association (Org.). (2013). Diagnostic and statistical manual of mental disorders: DSM-5. (5th ed). Washington, D.C. American Psychiatric Association. [ Links ]
Barlow, D. H. (Org.). (2014). Clinical Handbook of Psychological Disorders: A Step-By-Step Treatment Manual (5th ed.). New York. Guilford Publications. [ Links ]
Bilsker, D, & Goldner, E. (2000). Teaching Evidence-Based Practice in Mental Health. 10, 664-669. https://journals.sagepub.com/doi/abs/10.1177/104973150001000507 [ Links ]
Brown, T. A. (2015). Confirmatory Factor Analysis for Applied Research, Second Edition. New York. Guilford Publications. [ Links ]
Burato, K. R. da S., Crippa, J. A. de S., & Loureiro, S. R. (2009). Transtorno de ansiedade social e comportamentos de evitação e de segurança: Uma revisão sistemática. Estudos de Psicologia (Natal), 14, 167-174. https://doi.org/10.1590/S1413-294X2009000200010 [ Links ]
Caballo, V, Andrés, V, & Bas, F. (2011). Fobia Social. In Livro: Manual para o Tratamento Cognitivo-Comportamental dos Transtornos Psicológicos (p. 25-87). Curitiba. Editora Santos. [ Links ]
Clark, D., & Beck, A. (2011). Cognitive Therapy of Anxiety Disorders: Science and Practice. New York. Guilford Publications. [ Links ]
Filgueiras, A., Galvão, B. D. O., Pires, P., Fioravanti-Bastos, A. C. M., Hora, G. P. R., Santana, C. M. T., & Landeira-Fernandez, J. (2015). Translation and semantic adaptation of the Attentional Control Scale for the Brazilian context. Estudos de Psicologia (Campinas), 32(2), 173-185. https://doi.org/10.1590/0103-166X2015000200003 [ Links ]
Hair, J., Babin, B., Anderson, R., & Black, W. (2018). Multivariate Data Analysis (8a). Andover, Hampshire. Intl Thomson Business Pre. [ Links ]
Heimberg, R. G., Liebowitz, M, Hope, D. A., & Schineier, F. (1995). Social Phobia: Diagnosis, Assessment, and Treatment. New York. Guilford Press. [ Links ]
Herbert, J. D, Hope, D. A., & Bellack, A. S. (1992). Validity of the distinction between generalized social phobia and avoidant personality disorder. - PsycNET. APA PsycNet DoiLanding Page. https://psycnet.apa.org/doiLanding?doi=10.1037%2F0021-843X.101.2.332 [ Links ]
Hernandez-Nieto, R. (2002). Contributions to Statistical Analysis: The Coefficients of Proportional Variance, Content Validity and Kappa. Charleston. CreateSpace Independent Publishing Platform. [ Links ]
Hofmann, S. G., & DiBartolo, P. M. (Orgs.). (2014). Social Anxiety: Clinical, Developmental, and Social Perspectives (3a). Cambridge. Academic Press. [ Links ]
Leahy, R. L. (2020). ANXIETY FREE: Unravel Your Fears Before They Unravel You. London. Mandecilla Press. [ Links ]
Levitan, M., Nardi, A., Silva, A., & Quevedo, J. (2015a). Transtorno de ansiedade social: Diagnóstico e diagnóstico diferencial. In PROPSIQ programa de atualização em psiquiatria. (Vol. 2). Porto Alegre. Artmed Panamericana. [ Links ]
Levitan, M., Nardi, A., Silva, A., & Quevedo, J. (2015b). Transtorno de ansiedade social: Tratamento. In PROPSIQ programa de atualização em psiquiatria. (Vol. 1). Porto Alegre. Artmed Panamericana. [ Links ]
Liebowitz, M. R., Gorman, J. M., Fyer, A. J., & Klein, D. F. (1985). Social Phobia: Review of a Neglected Anxiety Disorder. Archives of General Psychiatry, 42(7), 729-736. https://doi.org/10.1001/archpsyc.1985.01790300097013 [ Links ]
MacKenzie, M. B., & Fowler, K. F. (2013). Social Anxiety Disorder in the Canadian Population: Exploring Gender Differences in Sociodemographic Profile. Journal of Anxiety Disorders, 27(4), 427-434. https://doi.org/10.1016/j.janxdis.2013.05.006 [ Links ]
Margis, R., Picon, P., Cosner, A. F., & Silveira, R. de O. (2003). Relação Entre Estressores, Estresse e Ansiedade. Revista de Psiquiatria do Rio Grande do Sul, 25, 65-74. https://doi.org/10.1590/S0101-81082003000400008 [ Links ]
Nardi, A. E., Quevedo, J., & Silva, A. G. da. (2013). Transtorno de Ansiedade Social: Teoria e Clínica (1a edição). Porto Alegre. Artmed. [ Links ]
Oliva, A. D. (2015). Origens Evolutivas dos Transtornos Mentais e Terapia Cognitivo-Comportamental. In PROCOGNITIVA Programa de Atualização em Terapia Cognitivo-Comportamental. (Vol. 2). Porto Alegre. Artimed Panamericana. [ Links ]
Oliveira, I. R. de. (2014). Trial-Based Cognitive Therapy: A Manual for Clinicians. (B. A. Moore, Org.). Oxfordshire. Routledge. [ Links ]
Raiche, G., Walls, T. A., Riopel, M., & Blais, J. G. (2013). Non-graphical solutions for Cattell's scree test. Methodology. 23-29. https://doi.org/10.1027/1614-2241/a000051 [ Links ]
Rapee, R. M., & Spence, S. H. (2004). The etiology of social phobia: Empirical evidence and an initial model. Clinical Psychology Review, 24(7), 737-767. https://doi.org/10.1016/j.cpr.2004.06.004 [ Links ]
Revelle, W. (2011). An Overview of the Psych Package. (Department of Psychology Northwestern University). 3, 1-25. https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.190.7429&rep=rep1&type=pdf [ Links ]
Rodebaugh, T. L., Fernandez, K. C., & Levinson, C. A. (2012). Testing the Effects of Social Anxiety Disorder on Friendship Quality Across Gender and Ethnicity. Cognitive Behaviour Therapy, 41(2), 130-139. https://doi.org/10.1080/16506073.2012.661451 [ Links ]
Rosseel, Y., Oberski, D., Byrnes, J., Vanbrabant, L, Savalei, V, Merkle, E., & Chow, M. (2017). An overview of the psych package. Department of Psychology Northwestern University. https://lavaan.ugent.be [ Links ]
Santos, L. F. dos. (2012). Estudo da validade e fidedignidade da Escala de Ansiedade Social de Liebowitz-Versão auto-aplicada. São Paulo. Universidade de São Paulo. https://doi.org/10.11606/D.17.2012.tde-03112012-112449 [ Links ]
Schreiber, J. B., Nora, A., Stage, F. K., Barlow, E. A., & King, J. (2006). Reporting Structural Equation Modeling and Confirmatory Factor Analysis Results: A Review. The Journal of Educational Research, 99(6), 323-338. https://doi.org/10.3200/JOER.99.6.323-338 [ Links ]
The R Foundation. (2018). R: What is R? https://www.r-project.org/about.html [ Links ]
Turner, S. M., & Beidel, D. C. (1989). Social phobia: Clinical syndrome, diagnosis, and comorbidity. Clinical Psychology Review, 9(1), 3-18. https://doi.org/10.1016/0272-7358(89)90043-3 [ Links ]
 Correspondence:
Correspondence:
Cybele Perciano Cypriano
cybelecypriano@gmail.com
Irismar Reis de Oliveira
irismar.oliveira@me.com
Submetido em: 03/09/2019
Aceito em: 04/12/2020


{kind=link}
{kind=link}
{kind=link}