










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkPsicologia em Pesquisa
versão On-line ISSN 1982-1247
Psicol. pesq. vol.7 no.1 Juiz de Fora jun. 2013
http://dx.doi.org/10.5327/Z1982-1247201300010006
ARTICLES
DOI: 10.5327/Z1982-1247201300010006
Does the Acute Cerebellitis play a role in the neurocognitive profile of a child after its onset?
A Cerebelite Aguda desempenha um papel no perfil neurocognitivo de uma criança após o seu inicio?
Heloisa Martinez FurnielI; Flávia Heloísa SantosI; Jose Javier Berenguer-PinaII; Fernanda Maria Paes Milanese RodriguesIII
ILaboratório de Neuropsicologia, Universidade Estadual Paulista "Júlio de Mesquita Filho" (Assis), Brasil
IIServicio Murciano de Salud (Murcia), Espanha
IIIRegional Hospital of Assis Dr. Joelson Leal Lisboa", Departamento de Pediatria (Assis), Brasil
ABSTRACT
This study aimed to present the neuropsychological assessment of MC, a seven-year-old girl, who was diagnosed with acute viral cerebellitis. The protocol included cognitive tests, stress and mood scales, behavioral observation, and interviews with family and school. In the neuropsychological assessment, difficulties in crystallized skills, especially in language and numerical cognition domains, were observed. The results of the neuropsychological assessment were discussed to detail her neurocognitive profile and verify to what extent her impairment could be attributed to the acute viral cerebellitis.
Keywords: Language; arithmetic; acute cerebellitis; neuropsychology; learning.
RESUMO
O estudo teve como objetivo apresentar a avaliação neuropsicológica de MC, menina de sete anos, diagnosticada com cerebelite viral aguda. Foram utilizados testes cognitivos, escalas de humor e estresse, observação comportamental, além de entrevista familiar e escolar. Na avaliação neuropsicológica, foram observadas dificuldades nas habilidades cristalizadas, em especial nos domínios da linguagem e cognição numérica. Os resultados da avaliação neuropsicológica foram discutidos visando detalhar o seu perfil neurocognitivo e verificar em que medida seus prejuízos poderiam ser atribuídos à cerebelite viral aguda.
Palavras-chave: Linguagem; aritmética; cerebelite aguda; neuropsicologia; aprendizagem.
Acute cerebellitis (AC), also named as "encephalitis cerebella" is an inflammatory syndrome characterized by cerebellar dysfunction (Batten, 1905). This neurological disorder commonly occurs during childhood, mainly around six years of age (Connolly, Dodson, Prensky & Rust, 1994; Nussinovitch, 2003; Weiss, 1959), and its onset is during or after an infection or after an immunization (De Bruecker, 2004).
The first description of acute cerebellar ataxia was reported by Shepherd (1848); sometime later, Batten (1905) classified the three types of ataxia, namely congenital, progressive, and AC. Although acute cerebellar ataxia and AC probably represent the same disease processes, the term AC is selectively used for more severe cases, and less favorable long-term prognosis (Desai & Mitchell, 2012).
The main symptoms of AC include vomiting, headaches, tremors, abnormal eye movements, dysarthria, and disturbances of consciousness ranging from somnolence to coma. Occasionally, there are symptoms of fever and stiff neck also (Sawaishi & Takada, 2002; Barkovich, 2005). These symptoms tend to disappear spontaneously in weeks or months after the initiation of the treatment; nevertheless, in some cases certain symptoms persist or even might be fatal (Barkovich, 2005).
The incidence of AC is uncertain. The medical records of all children hospitalized at an Israeli clinic, throughout an 11-year period, collected 39 cases over a population of roughly 60,000 children (Nussinovitch, 2003). In Netherlands, the incidence was 0.75 cases of acute cerebellar ataxia per 100,000 individuals, under 15 years of age over a 24-month period; and 70% of these cases were treated as in-patients (Van Der Maas, Bondt, Melker, & Kemmeren, 2009). In the United States, the frequency of AC was estimated to be 0.4% of all the neurological diseases of the pediatric hospital, 73 consecutive cases were reported during a period of 23 years (Connolly, Dodson, Prensky, & Rust, 1994).
Its physiopathology is characterized by inflammation of the cerebellum and the AC has been reported in association with childhood diseases, such as varicella, Epstein-Barr virus, mycoplasma pneumonia, rotavirus, human herpes virus, coxsackievirus, mumps, influenza, pertussis, and non-specific viral infections (Barkovich, 2005). In some cases, an infectious agent is isolated from the cerebrospinal fluid and in many cases, the cause of AC remains unknown (Desai & Mitchell, 2012).
Motor functions, coordination of voluntary movement, gait, posture, and speech, are the functions that traditionally associate with cerebellum integrity. However, recent findings suggest that the cerebellum may also play a role in higher cognitive activities, such as executive function (Ghez & Fahn, 1985; Schatz, Hale & Myerson, 1998; for a review see Bugalho, Correa & Viana-Baptista, 2006). In fact, the cerebellum plays an essential role in the organization of higher cognitive functions during development (Riva & Giorgi, 2000), especially in language (Leiner, Leiner & Dow, 1993).
Single case studies have associated the AC with language disorders, such as mutism (a severe incoordination of the volitional motor aspects of speech), and this condition was transient, however, the language skills were not completely recovered (Chiaretti, Fantacci, Bersani, Valentini, Pierri, & Serranti, 2011; Dimova, Bojinova & Milanov, 2009).
Dimova et al. (2009) reported a single case study of a girl aged seven years and half, who suffered two weeks of mutism; she also presented an involuntary laughing. Her receptive language was not affected and she was able to understand and obey simple commands. After six months, she showed improvements in speech, but the expressive language still deficient.
Hennes et al. (2012) study was carried out in 11 children with AC, aged between 13 and 14 years. They found that 45% of the children presented cognitive deficits according to their parent's observation. The parents reported deficits mainly in visual-spatial skills, language, and attention. However, no neuropsychological assessment was accomplished in this study.
Over a 12-year period, Chiaretti et al. (2011), found 17 cases of speech disorders following an AC insult, in children aged from two to seven years old. These children presented improvements between three days to five months of conventional treatment; nevertheless, in any case the speech was perfect afterward; no other cognitive skills were investigated. In the same study, Chiaretti et al. (2011), reported a single case of six-year-old girl with AC, associated with Echovirus; she presented mutism for 13 days. After six months, the child was able to formulate sentences, but her performance was quite slow.
In the context of the present study, it is important to explain crystallized and fluid intelligences; the former is the accumulated knowledge of an individual across lifespan, whereas the latter, requires adaptative behavior to new situations, and also are mostly affected after brain injury (Cattell & Horn, 1978). Crystallized intelligence is associated to vocabulary, mathematical skills, and also scholar achievement, such as geography or history; while the fluid intelligence can be assessed by solving novel problems, and taps on executive functions and processing speed (Lee, Yeatman, Luna & Feldman, 2011; Primi, 2002; Schelini, 2006).
Taking it into account, we may assume that in most single case studies of AC, the expressive language was more affected than the receptive language (Chiaretti, et al., 2011; Hennes, Zotter, Dorninger, Hartmann, Häusler, Huppke, & Jacobs, 2012; Dimova, Bojinova, & Milanov, 2009), and the other functions mostly affected were attention (Hennes, Zotter, Dorninger, Hartmann, Häusler, Huppke, & Jacobs, 2012) and executive functions (Schatz, Hale & Myerson, 1998), which suggest that AC is more frequently associated with impairment of fluid skills.
Neuropsychological assessment is a useful tool to identify, quantify, and qualify the cognitive deficits (Lezak, 1995). Besides, it is an objective measure of cognitive skills, being an advantage in contrast with studies based exclusively on self-report, which is a subjective measure. Assuming that cerebellar infection can leave cognitive sequels, the objective of this study was to investigate the neurocognitive profile of a seven-year-old girl after an onset of AC. We hypothesized that the child might present cognitive deficits in language but not in other cognitive functions, in case her impairment is a direct consequence of the AC. We also supposed that the child will not present a severe emotional distress following an onset of AC, based on the lack of reports in this matter.
MC's Medical History
MC is a girl of 84 months without any abnormalities on medical history before the current insult. She became in-patient at the Santa Casa de Misericordia de Assis in São Paulo State (Brazil) because of vomiting and dehydration. She remained hospitalized for three days, and then was discharged.
However, a week later, she was admitted at the pediatric intensive care unit (ICU) of the Hospital Regional de Assis "Dr. Joelson Leal Lisbon" because of neck stiffness, pain in the lower limbs, and ataxia.
Differential diagnosis procedure was performed: The cerebrospinal fluid test and the computed tomography (CT) scans were inconclusive. The magnetic resonance imaging (MRI) was observed to be normal, suggesting a benign condition. Result for Rheumatoid factor was found to be negative. MC was diagnosed with viral AC, and over 20 days of hospitalization, she was treated with corticoid, antibiotics, anti-inflammatory, and vitamin B1 (dexamethasone, ampicillin, acyclovir, ibuprofen, and thiamine, respectively).
During the fifth day of hospitalization, the child showed some improvement of the symptoms. She was able to walk and fed well; however, on the day before, she barely could extend her legs due to intense pain. On the day 12, she presented plastic hypertonia of all four limbs, facial paresis, bilateral ptosis, partial occlusion of eyelids, worsening ataxia, difficulty in swallowing and chewing, and pain in the limbs.
MC became anxious, stressed, and irritated. On the 17th day, she got a psychiatric investigation and was diagnosed with separation anxiety disorder of childhood (ICD-10 F93.0) and the acute stress reaction (ICD-10 F43.0), with symptoms of enuresis; a dose of imipramine (25 mg) was prescribed for its treatment. According to the ICD-10 (OMS, 1995), acute reaction to stress tends to disappear a few days after the stressing insult.
On the discharge consult, she presented slight alteration on her march, and was recommended for follow-up in pediatric and physiotherapy outpatient services. The psychologist from the hospital referred her for neuropsychological assessment, and the assessment begun two weeks after the hospital discharge, which was approximately six weeks after the onset of the symptoms. She returned only once as an outpatient for neuropediatric and psychiatric reviews. MC remained under psychopharmacological treatment for at least three months after hospitalization.
Methodology
Ethical Aspects
Prior to testing, informed written consent was obtained from MC's mother for the neuropsychological assessment and for the dissemination of scientific results.
Procedures
MC was admitted at the Laboratory of Neuropsychology of UNESP, Universidade Estadual Paulista and her neuropsychological assessment took place at the university clinic, i.e., Center for Applied Research in Psychology, in Assis Campus. The assessment process took place in eight sessions, each session lasting around 75 minutes, with short intervals to avoid fatigue and emotional distress when necessary. Additionally, four meetings were arranged to interview the mother and the teacher, respectively prior to the neuropsychological assessment and after that to explain the results to members of family and school. Afterward, the child was also explained the main results.
Materials
The protocol included instruments for different cognitive domains, such as the intelligence, attention, executive functions, memory, language, calculation, learning, visuospatial processing, and praxias-gnosias. Additionally, a screening of depressive mood and emotional distress was also performed.
Anamnesis: It was performed by taking a complete interview with special focus on the family configuration, gestational period, delivery, psychomotor, emotional and cognitive developments, schooling achievement, sociability, and social behavior (Santos, 2002).
Criterion of economic classification, Brazil - CCEB, 2011 (Associação Brasileira de Empresas de Pesquisa): It includes the instrument of economic segmentation that uses the presence and amount of comfort items and schooling of the head of the family, to differentiate the population. The score ranges provide the economic classification: A1, A2, B1, B2, C1, C2, D, and E. The A score represents the highest class of income and E score represent the smallest income level.
Intelligence
The Columbia Mental Maturity Scale - CMMS (Burgemeister, Blum & Lorge, 1959): It is a non-verbal measure of general reasoning ability with minimal motor response, widely used for children from three years to nine years old. Normative data for Brazilian children were provided by Alves and Duarte (2001).
The Wechsler Intelligence Scales for Children - WISC-III (Wechsler, 1991): The battery assesses different areas of intellectual abilities. The scale provides three different intelligence quotient (IQ) scores: a Full Scale IQ, a Verbal IQ, and a Performance IQ. Scores of four indexes are calculated using various combinations of subtests: Verbal Comprehension, Perceptual Organization, Processing Speed, and Resistance to Distraction. Normative data for Brazilian children were provided by Figueiredo (2002).
Executive Function
Wisconsin Card Sorting Test - WCST (Grant & Berg, 1948): This test was developed by Berg and Grant (1948) to assess abstraction ability and the ability to shift cognitive strategies in response to changing environmental contingencies. Normative data for Brazilian children were provided by Cunha and co-workers (2005).
Attention
The Corsi Block-Tapping Task (Kessels, van Zandvoort, Postma, Kappelle & De Haan, 2000). The Forward Corsi Block-Tapping Task has been widely accepted as a measure of visuospatial short-term memory. Normative data for Brazilian children were provided by Santos et al. (2005).
The ADHD Assessment Scale (EDAH; Escala Para la Evaluación del Trastorno por Déficit de Atención con Hiperactividad; Farré & Narbona, 2003): This scale classifies the child according to the predominance of the following symptoms: hyperactivity, attention deficit, conduct disorder, and hyperactivity with attention deficit, or symptoms of attention deficit/hyperactivity disorder associated with global conduct disorder. Normative data for Brazilian children were also provided by Poeta & Neto (2004).
Working Memory
The Corsi Block-Tapping Task (Kessels, Van Zandvoort, Postma, Kappelle & De Haan, 2000): After completing the forward span, the backward span was administered. The child had to repeat the sequence tapping in the specific blocks in reverse order, which is a measure of visuospatial working memory. Normative data for Brazilian children were provided by Santos et al. (2005).
Brazilian Children's Test of Pseudoword Repetition (BCPR) (Santos & Bueno, 2003): Each child was told at the beginning of the test that he/she would hear some "funny made-up word," which he/she should try to repeat aloud. It is a measure of phonological short-term memory. Normative data for Brazilian children were provided by Santos and Bueno (2003).
Episodic Memory
Free Recall of Words: Four lists of nine words each (2- and 3-sylable words) were presented to a child individually by a 1 per second rate and the child must recall as many items as possible in any order. After 20 minutes, the delayed free recall was requested (Santos, 2002). Normative data for Brazilian children were provided by Santos (2002).
Rivermead Behavioural Memory Test - Story Immediate Recall and Delayed Recall (Wilson, Cockburn, Baddeley & Hiorns, 1989): The purpose of this test is to detect impairment of everyday memory functioning and monitor change over a period of time. A story is read to the examinee that must recall it immediately. After 25-30 minutes, the delayed story recall is requested. Normative data for Brazilian children were taken from the guidebook (Wilson, Cockburn, Baddeley & Hiorns, 1989).
Language
Semantic verbal fluency: The child must generate as many examples as possible from each of the three semantic categories (animals, fruits, and toys) in one minute. Normative data for Brazilian children were provided by Santos (2007).
Phonological verbal fluency (Lezak, 1995): This requires the generation of as many examples as possible from each letter, F, A, and S, in one minute (Lezak, 1995). Normative data for Brazilian children were provided by Santos (2007).
Phonological Awareness Instrument of Sequential Assessment (CONFIAS, Consciência Fonológica - Instrumento de Avaliação Sequencial; Moojen et al., 2003): The CONFIAS assesses phonological awareness comprehensively and sequentially, considering the developmental relationship between phonological skills and writing achievement. The instrument classifies reading and writing abilities in four categories: pre-syllabic, syllabic, syllabic-alphabetic, and alphabetic. Normative data for Brazilian children were provided by Moojen (2003).
Calculation
Neuropsychological Test Battery for Number Processing and Calculation in Children - Zareki-R (Von Aster & Dellatolas, 2006): This test assesses the number representation in children considering cognitive abilities that are prerequisites for the acquisition of arithmetic skills, such as counting dots, counting backwards, dictation of numbers, mental calculation, reading numbers, positioning numbers on an analog scale, memory of digits, oral comparison, perceptive estimation, contextual estimation, problem solving, and written comparison. Normative data for Brazilian children were provided by Santos et al. (2012).
Visuospatial Construction
Copy of the Complex Picture of the BEM 144 (Signoret, 1991): The child was presented to the BEM Complex Picture, and requested to copy the figure as best he/she could. The order in which each child copied every item was noted on his protocol sheet. After this, the copying sheet was removed. Normative data for Brazilian children were provided by Santos and co-workers (2005).
Recall of the Complex Picture of the BEM 144 (Signoret, 1991): Immediately after copying the figure, the child was asked to reproduce the figure, as faithfully as possible without the model. Both copying and production were carried without using an eraser rubber or a ruler. The two tasks of copying and reproduction, tap on different skills, i.e., constructive function and visual memory, respectively. Normative data for Brazilian children were provided by Santos et al. (2005).
Schooling
School Achievement Test - SAT (Stein, 1994): It consists of three subtests that assesses writing skills (writing the name, saying words), reading (word recognition out of context), and arithmetic skills (solving calculations, both orally and in writing). The SAT aims to evaluate the core knowledge expected in accordance to the 1st to 6th grades in each one of the subtests, and also provides a general score. Normative data for Brazilian children were provided by Stein (1994).
Affective Behavior
Children's Depression Inventory - CDI (Kovács, 1983): The CDI evaluates the presence and severity of specific depressive symptoms in children so that a targeted treatment plan can be developed. It consists of a questionnaire with 20 items, containing three response options, of which the child selects the one that best describes his/her feelings in the last two weeks. The total score indicates the correspondent level of depression. The cut-off score is 23 points with a standard deviation of 2 points (Coutinho, Carolino & Medeiros, 2008). Normative data for Brazilian children were provided by Coutinho et al. (2008).
Stress Inventory - ESI (Lipp & Lucarelli, 1999). It consists of 33 items that aims to determine whether the child has a stress symptomatology. The stress symptoms provide four factors: physical (malaise, nausea, and enuresis), psychological (worry, nervousness, and sadness), psychological depressive symptoms (apathy and aggressiveness), and psychophysiological components (shyness, heart palpitations, difficulty breathing, and constant illness). Results are indicative of emotional distress if the score is equal or greater than 27 points in any of the four factors or the total scale note is greater than 105 points, indicating significant signs of stress (Moure, 2007). Normative data for Brazilian children were provided by Lipp and Lucarelli (1999).
Results
Criteria for Classification of the Cognitive Scores
The results were considered in terms of quantitative and qualitative aspects. For this purpose, the scores for cognitive tasks were obtained from the guidebooks or articles with normative data, specified in section on Materials. These scores were classified as slight, moderate, or severe impairments respectively, if the mean score of MC was 1 standard deviation (SD), or 2 or 3 SD below the mean score expected for her age or schooling level. This approach corresponds to a clinical measure of the symptoms severity. For scores 1SD above the average it was classified as "above average," as for the intelligence instruments, the items were classified using terms described according to the guidebooks standards.
Taking into account that, the child could have impaired motor skills because of the AC, extra time was provided to accomplish the tasks, mainly the ones who demanded chronometer, but the scoring system followed the guidebook standards in all conditions. All instruments were administered alternating verbal and non-verbal skills, and also controlling the cognitive domain. Intervals were provided to MC always whenever she seemed or assumed herself tired. The neuropsychological assessment had a holistic perspective, in that, different measures, such as observation, interpersonal interaction, scales, cognitive tests, and interview with people who maintain a daily basis relationship with the child were integrated.
Anamnesis
MC's mother informed about a normal pregnancy, as well as labor and caesarean delivery; and that after the birth, the girl presented a typical neuropsychomotor development.
The child lives with her mother and her maternal grandparents, the family socioeconomic status was equivalent to C1 (CCEB, 2011), which corresponds to two minimum wages per month. MC usually spends the weekends with her father and her paternal grandmother. During the period of the AC illness, the paternal grandmother requested legal custody of the child, because of the conflictive familiar relationship, but the judge's decision was favorable to her mother. According to MC's mother, the girl knew about the custody dispute, but no discussions about it were made in her presence. The mother also reported that the child had good relationship with both sides of the family.
According to her mother, MC started to present learning difficulties from the beginning of the first grade, mainly in calculations and writing. Despite of it, MC's ability to read was assumed by her mother as good. These difficulties remained throughout the first semester of the second grade, from February to June; then, she had the AC during the winter holidays (July), and after that she began both, the second semester at school and the neuropsychological assessment. MC's marks at school in both grades were lower than the expected, and there was a concern about the risk of reprobation by the end of the second grade. Besides, the mother mentioned that MC's class suffered a constant exchange of teachers throughout the first and second grades, which may also have influenced her literacy process, and consequently, the acquisition of learning skills. She remained under anti-depressant treatment by the time of her neuropsychological assessment. Both, mother and teacher reported improvements on MC's behavior in regard toenuresis and hyperactivity, respectively.
Behavior
In the first meeting the child was a bit shy, but carried out the tasks in a collaborative way. Most of the time she showed good ability to follow appropriate guidelines, although on some occasions she was slightly distracted. In the subsequent sessions, she was more communicative, making questions and starting conversations about everyday matters (friends, school, etc.). She also showed good ability to follow rules and became more interested in the activities. During the evaluation, she was engaged on performing the tasks and presented good skill to deal with frustration. She seemed to be a creative, curious, and an active child; she was also interested in playing games suitable for her own age. Hence, MC pursued to create emotional bonds.
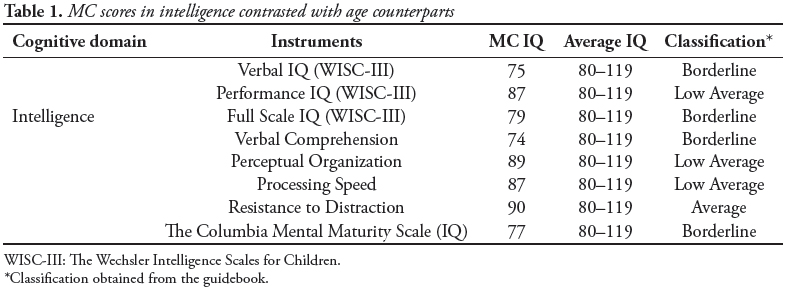
Intelligence (Table 1)
The analysis of the full IQ (WISC-III) indicated a cognitive performance below the expectancy level, classified as borderline. The Performance IQ was very near to average, whereas the Verbal IQ was framed as borderline. Following were the four indexes generated by the IQ (WISC-III): the Verbal Comprehension was lower than expected for her age and education levels; her Resistance to Distraction was about average, while, both Perceptual Organization and Processing Speed were rated as lower average, but very near to average scores (89 and 87 weighted points, respectively). Because she scored as borderline on WISC-III, a second instrument was used as confirmatory measure. The Columbia Mental Maturity Scale was chosen rather than Raven's Colored Progressive Matrices to avoid abstract reasoning demands. Nevertheless, her scores on Columbia Mental Maturity Scale were equivalent to her WISC-III IQ scores. According to this instrument, her maturity presented a delay equivalent to a child of five years old, which was not representative of her behavior on the entire neuropsychological assessment.
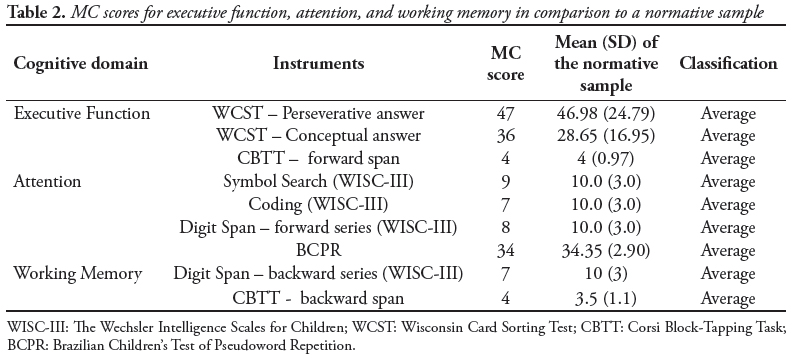
Executive Function (Table 2)
In Wisconsin Card Sorting Test, she demonstrated good capacity planning and reasoning abilities, therefore, suitable scores for her age.
Attention (Table 2)
The ADHD Assessment Scale was filled out by both mother and child's teacher. There were no indicative symptoms of attention deficit in the mother's questionnaire, but achieved a score indicative of hyperactivity and impulsivity. The same scale answered by the school teacher was not indicative for ADHD. During the neuropsychological assessment, there were no observation of attentional deficits across the instruments. Therefore, we suppose that the behaviors reported by mother might be associated to the family dynamics, but in more structured environments such as at school or on the clinical set, she was able to cope quite well. Considering her attention by the cognitive viewpoint, in timed activities, such as Coding and Symbol Search (WISC-III), MC performed as expected for her age, which suggest no damage in her attention span.
Working Memory (Table 2)
MC obtained results expected for her age in Digit Span backward order (WISC-III), and also in BCPR; these tasks in assembly indicate good phonological working memory capacity. Both the stages of the Corsi Block-Tapping Task (forward and backward), showed results within the average scores, which mean good visuospatial working memory as well.
Episodic Memory (Table 3)
In Immediate Recall and Delayed Recall of story (Rivermead Behavioural Memory Test), MC's scores were classified as expected for age, showing good ability to consolidate semantic information represented verbally. The exception was the immediate Free Recall of Words, but we supposed that the instruction of the task interfered on her achievement. The immediate word-list recall is an incidental measure of episodic memory, thus, she was not aware that she had to retrieve the items, as for the delayed recall the instruction was clear about keeping them in mind, and she succeeded in that condition. In reproductions Complex Picture of the BEM-144, the results were also within the average, but there was a better result in delayed recall, suggesting that she knows the benefits of time to organize information.
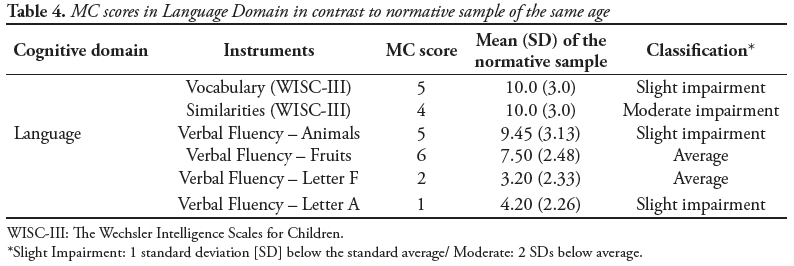
Language (Table 4)
The clinical observation, medical report, and performance on BCPR were not suggestive of articulatory deficits, such as dysarthria; but she presented lower scores in phonemic level of CONFIAS, and good ones for syllabic level. As for writing, her score on SAT was low average, due to orthographic errors and phonemic changes, like b/p or d/t. On SAT, her score in Reading was above average for both schooling and age; she used a lexical route and had difficulties only in irregular and less frequent words (exausto, durex, trouxe, repugnante, and advogado). However, in Vocabulary (WISC-III) and Similarities (WISC-III), she obtained substantial impairment, which respectively correspond to difficult in expressing her lexical knowledge, and limited ability to form concepts, in agreement with her deficits in Columbia's scale. She performed poorly in Semantic and Phonological Verbal Fluency, but not in all of items of these categories, which means that she understood the task, but had limited lexical knowledge to perform particular ones (for instance letter A and animals). This cannot be assumed as a speed processing limitation; because, if it was the case, she would have poor performance in all fluency items, besides, she would generate less exemplar in the first moments or her generation would be sparse across the time, but like most children, she also generated more exemplars by the first 30 seconds.
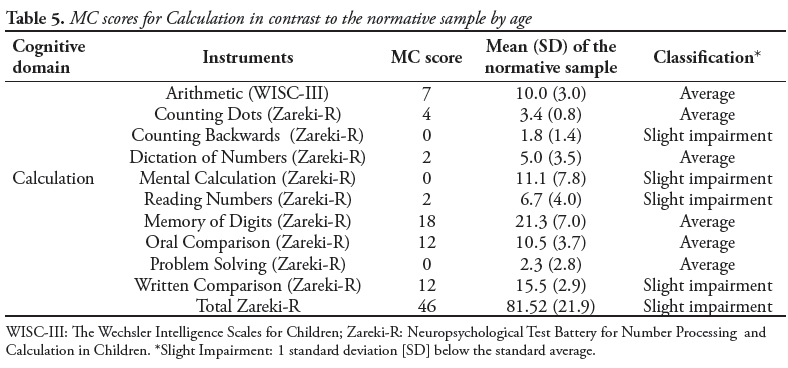
Calculation (Table 5)
In the calculation tasks, MC showed results ranging from average performance to slightly lower than expected. We observed a good performance in tasks that required counting, naming, and memorization of numbers; visual recognition of numbers and quantities; and writing numbers. However, she presented great difficulties to perform simple calculations (addition/subtraction units), without using pencil and paper. She also presented difficulties in performing additions and subtractions that already contained decimal system, even with the support of concrete materials. According to Silva & Santos (2011), a slight impairment on Zareki-R, even that present in different subtests, is not indicative of Developmental Dyscalculia.
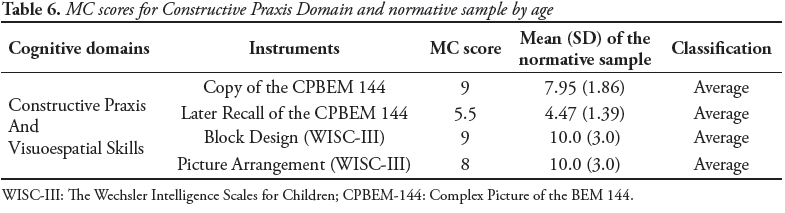
Visuospatial construction (Table 6)
MC displayed the capacity for orientation in space, perceptual organization, and planning of content, appropriate to her age group. Despite of the AC, her performance was satisfactory in all activities involving visuomotor coordination ("Block Design" and "Picture Arrangement," subtests of the WISC-III; and Complex Picture of the BEM 144).
Schooling (Table 7)
The total score on the Schooling Achievement Test (SAT) was classified as low average. The child got better results in reading and slight impairment, for arithmetic and writing, however her difficulties in learning were not severe enough to be classified as Learning Disabilities. Her difficulties in numerical cognition were confirmed and detailed by the Zareki-R.
Affective Behavior
According to the self-report of the child on the Stress Inventory and Children's Depression Inventory, there are no signs of stress or depression. Also, non-signals were observed during the interaction with the child.
Discussion
The present study aimed to determine whether there were cognitive impairments after the occurrence of AC in a seven-year-old girl. MC's physical condition was similar to the clinical symptoms described by Sawaishi and Takada (2002). The neuropsychological assessment began 45 days after the onset of AC during the course of the neurological recovery process, and performed under psychopharmacological treatment.
As for intellectual level, MC scored as borderline (WISC-III), which is below expectations for her age. This result was corroborated by a second instrument. The previous study did not associate the AC onset with IQ losses (Schatz, Hale, & Myerson, 1998). It is important to highlight that her full IQ was classified as borderline, because she had a borderline verbal IQ (Riva & Giorgia, 2000), in contrast to an almost average performance IQ.
MC had trembling experience during the time of the neuropsychological assessment, which could have affected in particular tests that demanded fine motor coordination and time control (Ghez & Fahn, 1985; Schatz, Hale & Myerson, 1998). Despite of it, she obtained nearly normal scores in both Performance IQ and Processing Speed Index. Her scores for all performance IQ subtests were suitable for her age, except for Object Assembly, in which she performed 1SD below average. As for subtests timed with a chronometer (verbal and non-verbal ones), her errors were never associated with the limit of time or lack of motivation.
Other skills, such as attention, executive function, and working memory were appropriate for her age band (Schatz et al., 1998) while the reading ability was very good, contrasting with results provided by Hennes and et al., (2012). Therefore, MC presented a good functioning on fluid skills (Cattell & Horn, 1978; Lee et al., 2011; Primi, 2002; Schelini, 2006).
MC also displayed good long-term memory skills. Overall, she obtained suitable scores in episodic memory for visual and verbal stimulus. Therefore,it confirms that the full IQ of MC is not in accordance with a global cognitive impairment, but reveals a selective impairment in specific skills, even that her CT and MRI scans were normal.
MC's results were below expectations for her age and education, in activities involving language domain (Vocabulary and Similarities, WISC-III; and Verbal Fluency for Animals and letter A, Writing subtest of SAT), except in reading. Chiaretti et al. (2011) and Dimova et al. (2009), evaluated girls with AC aged from 6 years to 7 years. They observed that sequel restricted to speech, affecting more expressiveness than receptive language, whereas MC was impaired in both verbal abilities, with greater difficulty in lexical knowledge and concept formation.
In numerical cognition, her performance was appropriate for most quantitative skills. However, there were deficits in tasks demanding number processing (counting backwards, reading numbers, and written comparison) and calculation (mental calculation), and her difficulties were independent of modality (verbal and non-verbal material). According to von Aster and Shalev's model of numerical cognition (2007), MC had satisfactory Cardinal system, which is innate, but had problems with both Arabic and Verbal number systems, while the fourth step still under development because she is young. Her profile does not suit the criteria for Mathematical Learning Disabilities, because she presents poor arithmetic skills without deficits in working memory, visual-spatial processing, executive functions or attention (Rubinsten, 2009).
In scholar achievement, the child's performance was classified as inferior for her age counterparts. Taking into account the ICD-10 (OMS, 1995), since the child is attending the second grade of the elementary school, her difficulties did not fulfill criteria for diagnosis of any Learning Disabilities yet. However, she might be at risk of developing learning disabilities if she still having such delay in learning without any support. In case her difficulties persist and get worse, she possibly will fit the criteria for mixed disorders for scholastic skills (F81.3; ICD-10, OMS, 1995), because she had poor scores in writing and calculation.
Nevertheless, we are not sure that MC impairments in writing and calculation can be assumed as direct consequences of the AC, because previously to the disease onset there was already a learning difficult complaint reported by the teacher and the family. Besides, according to them the literacy process was disturbed by organizational issues at school. On the other hand, emotional factors could interfere with her performance, and raise the pre-existent schooling difficulties because both MC and her family were experiencing emotional distress with the disease, the hospitalization, and the custody affair. However, based on the behavioral scales, the child was not under stress or depression by the time of the neuropsychological assessment. For this reason, it is more likely that MC's learning difficulties could be cognitively grounded.
Of course, acomprehensive view of her neurocognitive profile must consider three aspects. First, she was under psychopharmacological treatment throughout the neuropsychological assessment, and it could have residual side effects affecting her cognitive performance (Melo, 2000) and/or ameliorating the emotional self-report. Second, the majority of the studies mentioned in the literature were founded on self-report or proxy (Chiaretti, Fantacci, Bersani, Valentini, Pierri, & Serranti, 2011; Hennes, Zotter, Dorninger, Hartmann, Häusler, Huppke, & Jacobs, 2012; Dimova, Bojinova & Milanov, 2009), instead of using a detailed neuropsychological assessment. This might explain part of the discrepancy acrossthestudies. Third, her assessment could reflect the AC outcome, in transition to a regular brain functioning, as suggested by her IQ asymmetry.
Considering her scores are very near to average, we do believe that using her preserved skills and appropriate stimulation, her scores can improve with time. For this purpose, we provided guidance for both family and school, in the sense of offering an enriched environment to support MC's learning difficulties, as well as to accomplish a neuropsychological follow-up to see if the problems remained after the intervention. Because during the neuropsychological assessment, no signals of emotional distress were observed, she was not indicated for psychotherapy.
The priori hypothesis was partially refuted, because she had the typical impairment in language seemed in AC cases, but her deficits extended the profile described in the literature associated for this disease. It would be easier to assign her current difficulties to her AC insult or to her emotional issues. However, she obtained worse scores in crystallized skills, which are more consistent with the pre-existent inabilities rather than disrupted by the AC. In fact, it is possible that, her learning difficulties would receive attention from the family or school later on, even without her AC insult.
Conclusion
In conclusion, the neuropsychological assessment showed good fluid skills in contrast with slight and moderate impairments in crystallized abilities, respectively in mathematical skills and language. Reports from the mother and her teacher indicated that her difficulties were present previously to the AC. At the same time, these difficulties may present an earlier stage of a development learning disability, which reinforce the need of neuropsychological rehabilitation and follow up.
Acknowledgements
We particularly thank the child, her parents, and teacher for their participation in this study.
References
Alves, I. C., & Duarte, J. L. (2001). Escala de maturidade mental Colúmbia: Manual para aplicação e interpretação. São Paulo: Casa do Psicólogo Livraria e Editora Ltda. [ Links ]
Barkovich, A. J. (2005). Pediatric neuroimaging. Philadelphia: Limpicott Williams & Wilkins. [ Links ]
Batten, F. E. (1905). Ataxia in childhood. Brain, 28, 484-505. [ Links ]
Bugalho, P., Correa, B., & Viana-Baptista, M. (2006). Role of the cerebellum in cognitive behavioural control: Scientific basis and investigation models. Acta Médica Portuguesa, 19(3), 257-267. [ Links ]
Burgemeister, B., Blum, L., & Lorge, I. (1959). Columbia mental maturity scale manual. New York: World Book. [ Links ]
Cattell, R. B., & Horn, J. L. (1978). A check on the theory of fluid and crystallized intelligence with description of new subtest designs. Journal of Educational Measurement, 15, 139-164. [ Links ]
Chiaretti, A., Fantacci, C., Bersani, G., Valentini, P., Pierri, F., & Serranti, D. (2011). Acute pediatric cerebellitis and mutism. Case report and review of the literature. Signa Vitae, 6(2), 78-81. [ Links ]
Connolly, A. M., Dodson, W. E., Prensky, A. L., & Rust, R. S. (1994). Course and outcome of acute cerebellar ataxia. Annals of Neurology, 35(6), 673-679. [ Links ]
Cunha, J. A., Trentini, C. M., Argimon, I. L., Oliveira, M. S., Werlang, B. G., & Prieb, R. G. (2005). Teste Wisconsin de Classificação de Cartas - Adaptação e Padronização Brasileira. São Paulo: Casa do Psicólogo. [ Links ]
De Bruecker, Y., Claus, F., Demaerel, P., Ballaux, F., Sciot, R., Lagae, L., Buyse, G., & Wilms, G. (2004). MRI findings in acute cerebellitis. European Radiology, 14(8), 1478-1483.
Desai, J., & Mitchell, W. G. (2012). Acute cerebellar ataxia, acute cerebellitis, and opsoclonus- myoclonus syndrome. Journal of Child Neurology, 27(11), 1482-1488. [ Links ]
Dimova, P. S., Bojinova, V. S., & Milanov, I. G. (2009). Transient mutism and pathologic laughter in the course of cerebellitis. Journal of Pediatric Neurology, 41(1), 49-52. [ Links ]
Farré, A., & Narbona, J. (2003). Escala para la evaluación del trastorno por déficit de atención con hiperactividad. Madrid: TEA Ediciones. [ Links ]
Figueiredo, V. L. (2002). WISC-III: Escala de inteligência Wechsler para crianças - adaptação brasileira da. 3ª edição. São Paulo: Casa do Psicólogo. [ Links ]
Ghez, C., & Fahn, S. (1985). The cerebellum. In E. R. Kandel, & J. H. Schwartz (editors), Principles of neural science, 2nd ed. New York: Elsevier. [ Links ]
Grant, D. A. & Berg, E. A. (1948). A behavioral analysis of degree of impairment and ease of shifting to new responses in a Weigl-type card-sorting problem. Journal of Experimental Psychology, 38(4), 404-411. [ Links ]
Hennes, E., Zotter, S., Dorninger, L., Hartmann, H., Häusler, M., Huppke, P., Jacobs, J., Kraus, V., Makowski, C., Schlachter, K., Ulmer, H., Van Baalen, A., Koch, J., Gotwald, T., & Rostasy, K. (2012). Long-term outcome of children with acute cerebellitis. Neuropediatrics, 43(5), 240-248. [ Links ]
Kovács, M. (1993). The Children's Depression Inventory: A self-rated depression scale for school - aged youngsters. University of Pittsburg. [ Links ]
Lee, E. S., Yeatman, J. D., Luna, B., & Feldman, H. M. (2011). Specific language and reading skills in school-aged children and adolescents are associated with prematurity after controlling for IQ. Neuropsychologia, 49(5), 906-913. [ Links ]
Leiner, H. C., Leiner, A. L., & Dow, R. S. (1993). Cognitive and language functions of the human cerebellum. Trends in Neuroscience, 16(11), 444-447. [ Links ]
Lezak, M. D. (1995). Neuropsychological assessment. New York: Oxford University Press. [ Links ]
Lipp, M. E., & Lucarelli, M. D. (1998). Escala de Estresse Infantil - ESI. São Paulo: Casa do Psicólogo. [ Links ]
Melo, J. M. (2002). Dicionário de especialidades farmacêuticas. Rio de Janeiro: EPUC. [ Links ]
Moojen, S., Lamprecht, R. R., Santos, R. M., Freitas, G. M., Brodacz, R., Siqueira, M., Correa, A., & Guarda, E. (2003). CONFIAS - Consciência Fonológica: instrumento de avaliação seqüencial. São Paulo: Casa do Psicólogo. [ Links ]
Moure, R. C. (2007). Stress infantil em crianças institucionalizadas e não institucionalizadas: Um estudo comparativo. São Paulo. Dissertação. Faculdade de Ciências da Saúde de São Paulo. [ Links ]
Nussinovitch, M., Prais, D., Volovitz, B., Shapiro, R., & Amir, J. (2003). Post-infectious acute cerebellar ataxia in children. Clinical Paediatrics, 42(7), 581-584. [ Links ]
Organização Mundial da Saúde ]OMS]. (1995). Classificação Internacional de Doenças - CID-10, 10ª revisão. São Paulo: OMS. [ Links ]
Poeta, L. S., & Rosa Neto, F. (2004). Epidemiological study on symptoms of attention deficit/hyperactivity disorder and behavior disorders in public schools of Florianopolis/SC using the EDAH. Revista Brasileira de Pisquiatria, 26 (3), 150-155. [ Links ]
Primi, R. (2002). Inteligência fluida: Definição fatorial, cognitiva e neuropsicológica. Paidéia, 12 (23), 57-77. [ Links ]
Riva, D., & Giorgi, C. (2002). The contribution of the cerebellum to mental and social functions in developmental age. Fiziologiia Cheloveka, 26(1), 27-31. [ Links ]
Rubinsten, O. (2009). Co-occurrence of developmental disorders: The case of developmental dyscalculia. Cognitive Development, 24, 362-370. [ Links ]
Santos, F. H. (2002). Memória operacional de crianças normais e com lesões congênitas: Desenvolvimento cognitivo e reorganização cerebral. São Paulo. Tese de Doutorado. Universidade Federal de São Paulo. Escola Paulista de Medicina. [ Links ]
Santos, F. H., & Bueno, O. F. (2003). Validation of the Brazilian children's test of pseudoword repetition in Portuguese speakers aged 4 to 10 years. Journal of Medical and Biological Research, 36(11), 1533-1547. [ Links ]
Santos, F. H., Mello, C. B., Bueno, O. F., & Dellatolas, G. (2005). Cross-cultural differences for three visual memory tasks in Brazilian children. Perceptual and Motor Skills, 101(2), 421-433. [ Links ]
Santos, F. H., Silva, P. A., Ribeiro, F. S., Dias, A. L. R. P., Frigério, M. C., Dellatolas, G., & Von Aster, M. (2012). Number processing and calculation in Brazilian children aged 7-12 years. The Spanish Journal of Psychology, 15(2), 513-525. [ Links ]
Sawaishi, Y., & Takada, G. (2002). Acute cerebellites. Cerebellum, 1(3), 223-228. [ Links ]
Schatz, J., Hale, S., & Myerson, J. (1998). Cerebellar contribution to linguistic processing efficiency revealed by focal damage. Journal of the International Neuropsychological Society, 4(5), 491-501. [ Links ]
Schelini, P. (2006). Teoria das inteligências fluída e cristalizada: Início e evolução. Estudos de Psicologia, 11(3), 323-332. [ Links ]
Shepherd, A. B. (1848). Paralysis after scarlet fever. The Medical Times and Gazette, 1868(1), 144. [ Links ]
Signoret, J. L. (1991). Baterie d'efficience mnésique - BEM-144. Paris: Elsevier. [ Links ]
Silva, P. A., & Santos, F. H. (2011) Discalculia do Desenvolvimento: Avaliação da Representação Numérica pela ZAREKI-R. Psicologia: Teoria e Pesquisa, 27(2), 35-44. [ Links ]
Silva, A. N., Andrade, V. M., & Oliveira, H. A. (2007). Avaliação neuropsicológica em portadores de epilepsia do lobo temporal. Arquivos de Neuro-psiquiatria, 65(2b), 492-497. [ Links ]
Stein, L. M. (1994). TDE: Teste de Desempenho Escolar: Manual para aplicação e interpretação. São Paulo: Casa do Psicólogo. [ Links ]
Strauss, E., Sherman, E. M., & Spreen, O. (2006). A compendium of neuropsychological tests: Administration, norms, and commentary. New York: Oxford University Press. [ Links ]
Van der Maas, N. A., Bondt, P. E., de Melker, H., & Kemmeren, J. M. (2009). Acute cerebellar ataxia in the Netherlands: a study on the association with vaccinations and varicella zoster infection. Vaccine, 27(13), 1970-1973. [ Links ]
Von Aster, M., Dellatolas, G., & Zareki, R. (2006). Batterie pour l'évaluation du traitement des nombreset du calcul chez l'enfant. Paris: ECPA. [ Links ]
Von Aster, M., & Shalev, R. S. (2007). Number development and developmental dyscalculia. Developmental Medicine & Child Neurology, 49 (11), 868-873. [ Links ]
Wechsler, D. (1991). The Wechsler intelligence scale for children, 3rd edition. San Antonio, TX: The Psychological Corporation. [ Links ]
Weiss, S., & Carter, S. (1959). Course and prognosis of acute cerebellar ataxia in childhood. Neurology, 9, 711. [ Links ]
Wilson, B. A., Cockburn, J. M., Baddeley, A. D., & Hiorns, R. (1989). The development and validation of a test battery for detecting and monitoring everyday memory problems. Journal of Clinical and Experimental Neuropsychology, 11(6), 855-870. [ Links ]

Profa. Dra. Flávia Heloísa dos Santos
Universidade Estadual Paulista
Laboratório de Neuropsicologia
Departamento de Psicologia Experimental e do Trabalho
Avenida Dom Antônio, 2100
CEP 19806-900 - Assis/SP
E-mail: flaviahs@assis.unesp.br
Recebido em 14/03/2013
Revisto em 24/04/2013
Aceito em 29/04/2013

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}