










Serviços Personalizados
artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Compartilhar

 Permalink
PermalinkContextos Clínicos
versão impressa ISSN 1983-3482
Contextos Clínic vol.10 no.1 São Leopoldo jan./jun. 2017
http://dx.doi.org/10.4013/ctc.2017.101.01
ARTIGOS
Methodological quality of strength-based intervention programmes in latin america: a systematic review of the literature
Qualidade metodológica de programas de intervenção baseados em fortalezas na américa latina: uma revisão sistemática da literatura
Helen Bedinoto Durgante
Universidade Federal do Rio Grande do Sul. Rua Ramiro Barcellos, 2600, Santa Cecília, 90035-003, Porto Alegre, RS, Brasil. helen.durga@gmail.com
ABSTRACT
This review systematically synthesised information of strengthen-based intervention programmes for adults conducted in Latin America, and summarized the current body of evidence available about the methodological quality, efficacy and/or effectiveness of these programmes, as well as implications of the findings for future research and evidence-based practices in Psychology. Medline, Scopus and PsycINFO databases (no chronological window restriction) were searched for empirical work on strengthen-based interventions programme. Overall, 15 studies were included and assessed for methodological quality. The interventions selected focused on assertiveness, empathy, coping, forgiveness, gratitude, optimism and resilience. The results revealed that 100% of the studies identified some kind of positive effect after intervention. However, methodological quality of studies showed a variety of pitfalls. Only 46% of studies achieved high quality and two studies applied experimental design (randomization). Implications for future research on intervention outcome assessment are discussed.
Keywords: positive psychology, methodological quality, intervention programme.
RESUMO
Esta revisão sintetizou sistematicamente informações sobre programas de intervenção baseados em fortalezas, para adultos, conduzidos na América Latina, e resumiu o atual corpo de evidências disponíveis sobre a qualidade metodológica, eficácia e/ou efetividade desses programas, bem como as implicações dos resultados para futuras pesquisas e práticas baseadas em evidências em Psicologia. Buscas foram feitas nos bancos Medline, Scopus e PsycINFO (sem restrição cronológica) por artigos empíricos sobre programas de intervenção baseados em fortalezas. Ao todo, 15 estudos foram incluídos e avaliados quanto à qualidade metodológica. As intervenções selecionadas focaram em assertividade, empatia, enfrentamento positivo do estresse, perdão, gratidão, otimismo e resiliência. Os resultados revelaram que 100% dos estudos identificou algum tipo de efeito positivo após a intervenção. No entanto, a qualidade metodológica dos estudos mostrou uma variedade de falhas. Apenas 46% dos estudos alcançou alta qualidade, e dois estudos utilizaram delineamento experimental (randomização). Implicações para futuras pesquisas sobre avaliação de resultados de intervenção são discutidas.
Palavras-chave: psicologia positiva, qualidade metodológica, programa de intervenção.
Introduction
Interventions in Psychology have mostly emphasized the role of evidence-based health-related programmes aimed at providing optimal human functioning (Straub, 2012). Following the guidelines for evidence-based practices in Psychology (EBPP), within the last decades psychological interventions have prompted excellence in the delivery of health services, in line with empirical support from the best available research and expertise in the fields of healthcare applied to professional practices (APA, 2006). In that, empirical evidence set the basis for health interventions programme and subsequent evaluation criteria for programmes' outcomes. The rationale underlying EBPP is not only to improve the quality of health promotion programmes in Psychology, but also to ensure the efficacy of programmes resultsand impact on public health policies in the long run (APA, 2002). Efficacy refers to the scientifically detected beneficial effects produced by the programme to a target population when delivered in a controlled setting, whereas effectiveness refers to outcomes when intervention programmes are delivered in real-world conditions or clinical settings (APA, 2002; APS, 2010). On this basis, this paper focuses on summarizing evidence available about the methodological quality, efficacy and/or effectiveness of strength-based programmes for health promotion, addressing implications of the findings in the fields of evidence-based practices in Psychology.
The use of consolidated scientific evidence for the implementation of cost-effective health intervention programmes has become a major standpoint fordecision-making in terms of worldwide public healthcare (APS, 2010). The evidence-based approach in psychological research and practice illustrates the significant role and responsibility of psychologists in developing and delivering effective health programmes relevant to patient's needs and culture (APA, 2006). In this case, it is expected that programmes successfully meet the requirements for a high-quality service by not only achieving their previously set goals and agenda, but also contributing to social welfare. This is expected to be achieved by empowering individuals and communities to successfully get hold of their own determinants of health (physical, emotional, spiritual and environmental factors that influence health) through the dissemination of education for health practices (Albee, 1982; HPI, 2014; Jack et al., 2012; Schwartz, 2000). This is considered a fundamental and sustainable principle for health promotion, when individuals assume responsibility for their own health, and deliberately act towards health-promoting behaviours. In this regard, it is known that empirically-supported and well-structured health intervention programmes extend to provide long-lasting effects and positively impact on a wide range of individuals' health behaviours and health outcomes (Shapiro et al., 2000).
Also aligned with the changing nature of EBPP and demands in healthcare perspectives, Biopsychosocial approaches to health grounded on concepts from Positive Psychology have been systematically applied as an effort to enhance the preventive aspects of health programmes in Psychology (Snyder and Lopez, 2007; Straub, 2012). In other words, recent psychological interventions started to pinpoint the preventive role of strength-based programmes including biological, psychological and social variables that were previously overlooked in empirical science and research. Strength-based perspectives for health promotion entail a wide variety of personal (dispositional factors, such as positive goal-setting, problem-solving and empathic skills, an optimistic take on live) and interpersonal factors (family and peer relations, positive environment, and so forth), all of which function as pillars to building on one's capacity to better deal with life stressors and demands (Norman, 2000; Masten, 2014; Snyder and Lopez, 2007). Such factors were also referred to as universal character strengths, and the very principal underlying strength-based interventions is that of highlighting one's already existing strengths (potentials or virtues), or helping one develop such strength and optimal functioning (Aspinwall and Staudinger, 2013; Seligman, 2002). The strength-based perspective happens to contrast previous health intervention approaches that would primarily focus on individuals' deficits or lack of skills - psychopathology - as an attempt to reduce symptomathology (Seligman, 2002; Seligman and Csikszentmihalyi, 2000).
This shift in perspectives helped to identify that some less obvious psychological resources, happen to be significant predictors of incremented health and decreased likelihood of illness (Seligman and Csikszentmihalyi, 2000; Straub, 2012). It turns out that by promoting human strengths, may function as protective factors for the development and maintenance of health (Seligman, 2002). Amongst the strengths identified useful for psychological and physical health (Aspinwall and Staudinger, 2013; Linley et al., 2007; Falcone, 1999) are constructs related to social skills, thought to be central to foster one's resources to effectively engage, and remain in social interactions along the course of individuals' lives. Social skills entail the various interpersonal patterns of an individual's behaviours learned from previous social interactions. In that sense, empathy is seen as a key component for the quality and length of interpersonal relationships, due to being a main factor necessary for individuals be more sensitive and emotionally engaged in the needs of others (Falcone, 1999; Correa, 2008), be socially connected (Ward and Durrant, 2013) and for the establishment of positive interpersonal relationships, hence reduced social violence (Mytton et al., 2002). Empathy was also associated with the effectiveness of health interventions in previous reviews (Grenard et al., 2006).
In a similar manner, empathy seems to be a precursor to trigger other fundamental strengths such as gratitude and forgiveness (Emmons and McCullough, 2003; Snyder and Lopez, 2007). Gratitude refers to the disposition of recognizing and being thankful for people or things in life. Recent evidence suggests that individuals who express more gratitude also present increased life satisfaction, positive affect and subjective well-being. Not surprisingly, gratitude and positive gratitude outcomes also correlate with incremented physical activities, more optimistic views of life situations and less frequent visits to physicians (Emmons and McCullough, 2003). Likewise, interventions to promote one's ability to forgive (personal disposition to abandon the resentment against a transgressor) have been documented to result in decreased levels of depression-like symptoms, less frequent episodes of anxiety, as well as increased hope, optimism in the future and life satisfaction (Livingstone et al., 1996). The combination of these psychological and physical outcomes are considered core variables underlying human capacity to overcome adversities (Resilience), thus crucial for a well-balanced physical and mental health (Aspinwall and Staudinger, 2013; Snyder and Lopez, 2007; Straub, 2012).
The recognition of human strengths as fundamental psychological resources, and mediating factors for one's competent social repertoire (Seligman and Csikszentmihalyi, 2000; Straub, 2012), reduced health-related implications (Trivedi, 2015) and preventive measures to health (Sarafino and Smiths, 2014), led to the increasing development of a wide range of health promotion interventions to different target populations worldwide (Kelm et al., 2014). It is worth noting still that due to the multitude of variables that tend to play a role in an individual's well-being and optimal states of health functioning, researchers have stressed the need of delivering multicomponent intervention programmes. That is, programs that incorporate a combination of efforts/practices, as well as different variables of interest to maximize benefits of targeted outcome variables (Shults et al., 2009).
However, although considerable amount of empirical evidence state clear the need of evidence-based health practices in psychological science, the number of interventions that have been put under scientific scrutiny for adequate methodological quality, efficacy and/ or effectiveness, and impact on programme receiver's needs, remains below the ideal level. This is particularly true in Latin American contexts, where lack of resources (financial and human resources), public policies to ensure paramount health practices and, at times, lack of professional expertise in the delivery of services, put additional burden on evidence-based health practices in Latin America (Babor and Caetano, 2005).
So far, the vast majority of strengthen-based intervention studies that have been systematically assessed for outcome measures and cost-effective results, are those conducted in English-speaking countries, or published in English language (Coren, 2013). Yet, the scarcity of research available on studies of such interventions in non-English speaking countries leaves no grounds for comparisons about the quality, efficacy and/or effectiveness of these interventions. This is a critical issue to be addressed once current Psychology main task-force has been to ensure the dissemination of effective preventive measures, as opposed to only lessen individuals' already existing illnesses (APA, 2006; Straub, 2012).
Thus, despite the recent growing interest in the fields of healthcare in delivering strength-based intervention programmes (Albee, 1982; Coren, 2013; Shults et al., 2009), it is crucial that the question of having empirically-supported interventions is also addressed for non-English speaking contexts, so that comparative conclusions of effective health interventions may be drawn thoroughly. On this basis, the purposes of this systematic review are: (i) to describe and discuss the studies available about strengthen-based intervention programmes for adults conducted in Latin America; (ii) to summarize the current body of evidence available about the methodological quality, efficacy and/or effectiveness of these programmes in Latin America; (iii) to point out implications of these findings for future research and evidence-based practices in Health Psychology.
Methods
Literature searches were conducted in August 2015 and April 2016, to assess existing reviews related to the present research questions on: the Cochrane Database of Systematic Reviews (CDSR); the Database of Abstracts of Reviews of Effects (DARE); the Campbell Library of Systematic Reviews; the database of systematic and non-systematic reviews of public health interventions (DoPHER) available from the Evidence for Policy and Practice Information (EPPI) Centre (CRD, 2009). The searched terms were: 'empathy programmes/programs', 'empathy'; 'forgiveness programmes/programs', 'forgiveness'; 'assertiveness programmes/programs', 'assertiveness'; 'resilience programmes/ programs', 'resilience'; 'optimism programmes/ programs', 'optimism'; 'coping programmes/ programs', 'coping'; 'gratitude programmes/ programs', 'gratitude', and 'strength-based', 'strength-based intervention'.
A series of published reviews was found across the different databases including interventions for the promotion of physicians empathy (Shapiro et al., 2000), psychotherapeutic interventions to promote forgiveness (Living-stone et al., 1996), assertiveness interventions to reduce aggressive behaviour in people with learning disabilities (Hassiotis and Hall, 1996);
psycho-educational interventions for resilience in children (Coren, 2013), coping with multiple sclerosis (Busch et al., 2014) and cancer (Li and Loke, 2014). There were no reviews identified for the searches including 'gratitude', 'optimism' and 'strength-based' key terms. All literature reviews identified gather articles mostly from North America, Europe and Oceania. Thus, not having found evidence of previous review that addresses the present research questions for adult population, within the Latin American context, and that applied criteria for programme evaluation, this reinforces the need for conducting this review.
Eligibility criteria for studies
The studies selected included empirical programme intervention for adults (18 years of age or above) conducted in the Latin American countries (language of publication: English, Spanish and Portuguese), that state at least two variables of interest (empathy, forgiveness, assertiveness, resilience, optimism, coping and gratitude) as primary or secondary outcome measures, in order to assess multicomponent intervention programmes. Additional to those, papers had to incorporate criteria for programme evaluation (qualitative or quantitative research methods; present objective or subjective measures/indicators of programme evaluation; and/or follow-up results), as well as to have made use of at least one standardized instrument to be included. The databases used were PsychINFO, Medline and SCOPUS including English, Spanish and Portuguese terminology. There was no restriction (chronological window or timeline) of dates or publication period for the studies evaluated. The publication timeline of evaluated studies was kept open to check the progress of health research in Latin America including the variable of interest. Keywords used for the searches were: intervention; AND adults; AND Latin America; AND empathy; AND gratitude; AND forgiveness; AND optimism; AND assertiveness; AND resilience; OR strength-based; OR programme OR program OR training; without the words: child*, adolescent*, school*, youth*. The keywords were adapted to each database in accordance with thesaurus for the control of terms and indexation in health and psychological sciences. The reference lists of full-text articles evaluated for eligibility were analyzed as supplementary resources to identify potentially relevant articles for this review.
Study selection
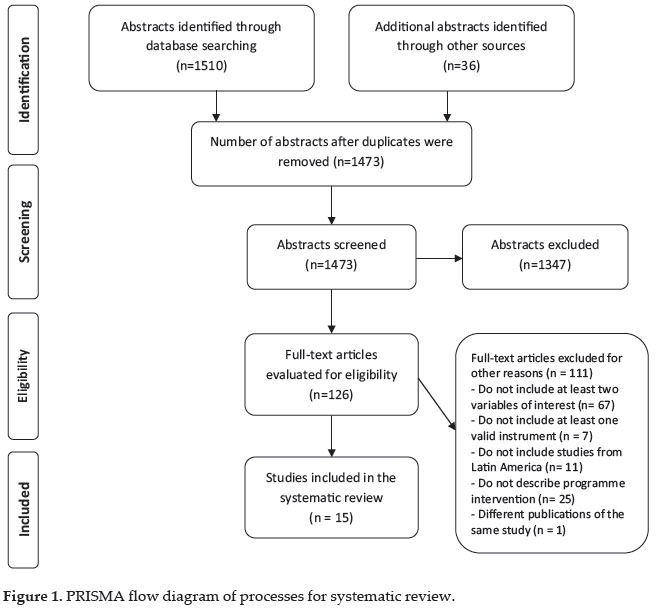
Figure 1 shows the different phases of studies selection. Each paper title and abstract generated by the searches was individually examined in contrast with the eligibility criteria for study inclusion in the review. Screening for duplicates was conducted simultaneously to abstract extraction, paying particular attention to participants, intervention, outcomes or outputs and study design. Those that matched inclusion criteria were compiled and the full-text article version was further investigated for methodological adequacy. Out of 1510 results of non-duplicated abstracts available for the search, 126 articles were analyzed in further details. Of these, 111 studies were excluded for other reasons (did not include at least two variables of interest [n= 67]; did not include at least one valid instrument [n = 7]; did not include studies from Latin America [n= 11]; did not describe programme intervention [n= 25]; different publications of the same study [n = 1]). The searches, analysis and selection process of obtaining data was conducted by the author (H.D.), and further checked by an independent researcher from the same higher education institution, to reduce methodological bias in the review process.
Methodology quality assessment of selected studies
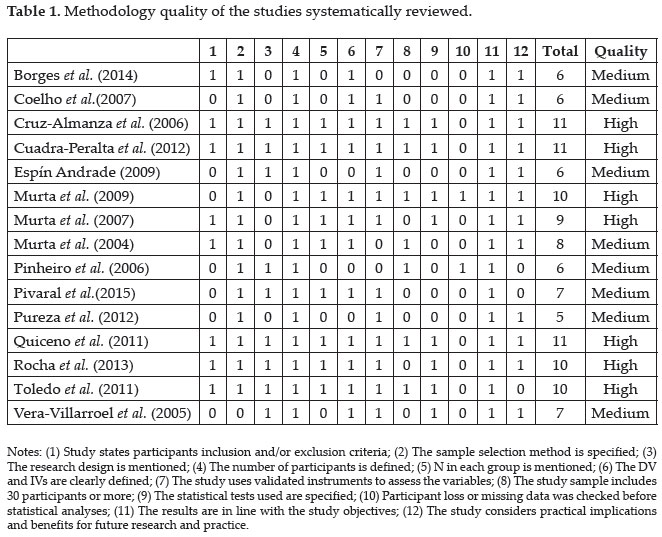
Each selected study was rated for methodology quality to reduce the risk of bias and increase measures of consistency for studies quality assessment. This was adapted and followed Barra et al. (2008) and García-Llana et al. (2014) instrument for critical evaluation of cross-sectional studies, also in accordance with PRISMA guidelines for evidence-based research. The rating consisted of awarding one point for each of the required quality criteria fulfilled by the analysed study. The 12-point quality criteria are described in Table 1. It includes four main types of criteria: Research selection and design (includes five criteria); Study variables: Definition and measurement (includes two criteria); Method and analysis of data (includes three criteria); Results and discussion (includes two criteria). Based on a 12-point scale, high quality articles comprise studies that reach 9-12 points; medium quality includes 5-8 points; and low quality articles rate between 1-4 points. Details of studies quality benchmarks are available in Table 1.
Results
The studies evaluated presented different degrees of research design quality. The majority of studies only presented modest support for effectiveness interventions (see details in Table 2). Out of 15 full-text articles reviewed, seven showed high-quality, whereas the other eight studies reached medium-quality standards. Of the high-quality, only two studies utilized experimental design (Cruz-Almanza et al., 2006; Rocha et al., 2013) with adequate random allocation of participants to conditions, despite none of the studies have ensured control over double-blind procedures to treatment groups (Shaughnessy et al., 2012). Nonetheless, if we ought to agree that in order to fulfil methodological requirements for a high level programme intervention, designs should include at least pre-post evaluation and, ideally follow-up studies, the number of high-quality papers which included pre-test and post-test outcome measures drops to only six studies being a CBT group intervention for abused women in Mexico (Cruz-Almanza et al., 2006); a Positive Psychology programme to improve depressive symptoms and life satisfaction of the elderly in Chile (Cuadra-Peralta et al., 2012); two occupational stress management interventions in Brazil (Murta and Tróccoli, 2009, 2007); a brief intervention to foster Resilience in chronically ill patients in Colombia (Quiceno et al., 2011); and an intervention programme to improve anxiety and emotional regulation of working labours in Cuba (Toledo et al., 2011).
In terms of follow-up studies for the impacts of high-quality programmes in the long-term, results are even more sparse where only three papers reported follow-up assessments at T2 (three months), T3 (six months) and T4 (18 months) (Cruz-Almanza et al., 2006); T2 (three months) (Quiceno et al., 2011); and a social skills educational programme for mothers of ADHD children in Brazil, which included but did not report follow-up length (Rocha et al., 2013). Despite having reached high-quality statues, only one study showed significant results for all primary outcome measures- for the purpose of this review: Coping and Assertiveness (Cruz-Almanza et al., 2006). Of the six other papers rated high-quality, two outlined at least two variables of interest for this review as primary outcome measures. Of those, an anxiety and emotional regulation intervention for labours (Toledo et al., 2011) showed significant differences for Coping across groups, and one study (Murta and Tróccoli, 2007) presented no significant results for any variable of interest (expected to improve Assertiveness and Coping) following a stress management intervention. Two high-quality papers (Rocha et al., 2013; Quiceno et al., 2011) showed only one variable of interest as primary outcome measure (Assertiveness and Resilience, respectively), stated in the programmes' main objectives. These studies were included in this review due to presenting other variables of interest as unexpected secondary outcome measures (as a results of interaction effects of primary outcome measures) following a social skills educational programme - also expected to improve Coping and Empathy (Rocha et al., 2013) and a brief intervention for chronically ill patients - expected to improve Gratitude and Assertiveness (Quiceno et al., 2011). Similar interaction effects were detected in two other studies following a stress management intervention - to improve Coping (Murta and Tróccoli, 2009), and a Positive Psychology programme - Forgiveness, Gratitude and Optimism as secondary outcome measures (Cuadra-Peralta et al., 2012).
The number of medium-quality papers which included pre-post evaluations is modest to only four studies including a psycho-education intervention for self-care of elderly males in Brazil (Borges and Seidl, 2014); a social skills educative training for parents of children with behavioural problems in Brazil (Pinheiro et al., 2006); a social skills training for university students with social anxiety/phobia in Brazil (Pureza et al., 2012); and a brief behavioural intervention for the management of emotional states of teachers in Chile (Vera-Villarroel et al., 2005). Only one medium-quality paper used follow-up study at T2 (four months) and reported improvement in Assertiveness and Empathy following a psycho-education intervention (Borges and Seidl, 2014). One medium-quality study utilized a pre-experimental design and was shown to result in increased Coping and no significant results for Assertiveness following a psycho-education intervention for carers of demented elderly (Espín-Andrade, 2009). Another medium-quality paper analysed the levels of satisfaction and dissatisfaction of hospital workers with a Cognitive Behavioural Model for stress reduction (Murta and Tróccoli, 2004) and did not include analysis of programme's main effects and/or outcomes, efficacy, pre-post evaluations and follow-up studies. Unexpected high dropout rates for severe anxiety individuals, as well as no significant results for Assertiveness and Empathy were detected following a social skills training intervention for university students with social anxiety and/or social phobia (Pureza et al., 2012). A group training programme for parental educational practices (Coelho and Murta, 2007) and a psycho-educative intervention to reduce Burnout in the workplace (Pivaral et al., 2015) reported increases in Coping and Empathy. Assertiveness was reported to improve and no significant result was found for Optimism after a brief behavioural intervention for emotional states of teachers (Vera-Villarroel et al., 2005), as well as improvement in Assertiveness and Empathy following a social skills educative training for parents of children with behavioural problems (Pinheiro et al., 2006).
Methodology quality
The overall score for methodology quality criteria of high-quality papers (9-12 points) was achieved by seven studies out of 15; where as the other eight studies achieved medium-quality (5-8 points). No study was classified as low quality (1-4 points). The item-by-item break down for methodology quality is shown in Table 1. Only two studies (Murta and Tróccoli, 2009; Pinheiro et al., 2006) reported clear in the text whether the loss of participants and/or the data lost was correctly addressed, or at least that the quality of the data had been reviewed before statistical analysis. All studies reported results in line with the objectives proposed, despite seven studies having reported the variables of interest for this review as secondary outcome measures (e.g., Borges and Seidl 2014; Coelho and Murta, 2007; Cuadra-Peralta et al., 2012; Murta and Tróccoli, 2009; Pivaral et al., 2015; Pureza et al., 2012; Rocha et al., 2013). The majority of studies published achieved good standards in terms of methodology quality.
Bias assessment: Participants' characteristics, gender, age and/or socioeconomic status
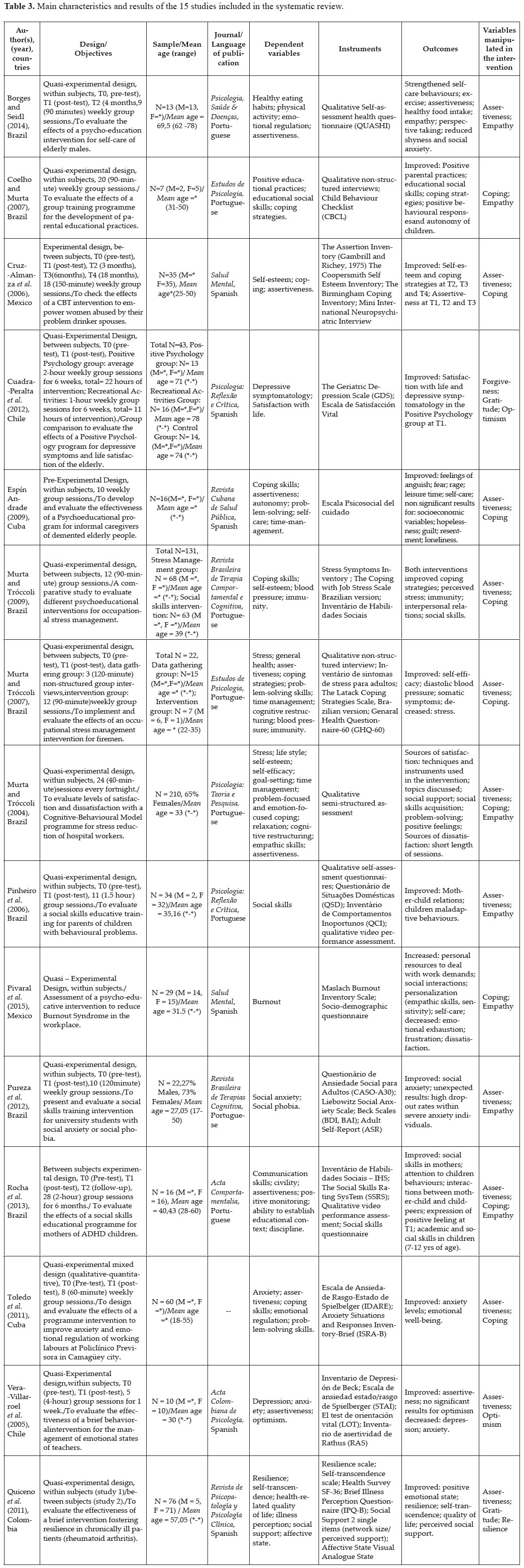
Although the studies compiled in this review were drawn from samples of a diverse cultural background including countries like Brazil, Colombia, Mexico, Chile and Cuba, the predominant target population identified amongst the studies was workers/labours (Murta and Tróccoli, 2009; Pivaral et al., 2015; Toledo et al., 2011), including teachers (Vera-Villarroel et al., 2005), firemen (Murta and Tróccoli, 2007), hospital staff (Murta and Tróccoli, 2004) and carers of demented people (Espín-Andrade, 2009). For those, the variables of interest manipulated in intervention programmes include Assertiveness, Coping, Empathy and Optimism. Out of the remaining studies reviewed there were three interventions for parents of children with cognitive or behavioural problems (Coelho and Murta, 2007; Pinheiro et al., 2006; Rocha et al., 2013), aimed to improve Assertiveness, Coping and/ or Empathy; two for elderly people (Borges and Seidl, 2014; Cuadra-Peralta et al., 2012), aiming to positively impact on Assertiveness, Empathy, Forgiveness, Gratitude and/or Optimism; one intervention for Rheumatoid Arthritis patients (Quiceno et al., 2011), focusing on Assertiveness, Gratitude and Resilience; one for abused women (Cruz-Almanza et al., 2006), to improve Assertiveness and Coping; and one intervention programme for students with social anxiety and social phobia (Pureza et al., 2012), which aimed to but did not present significant results for Assertiveness or Empathy. Also in terms of participants' characteristics, 46.6% (seven studies) reported to have included at least 30 participants to compose the sample (Cruz-Almanza et al., 2006; Cuadra-Peralta et al., 2012; Murta and Tróccoli, 2004, 2009; Pinheiro et al., 2006; Quiceno et al., 2011; Toledo et al., 2011). The lowest number of participants identified in a study was N=7 (Coelho and Murta, 2007), in a group training programme to promote Coping and Empathy. Conversely, the highest sample described in a study included N=210 participants (Murta and Tróccoli, 2004) in a Cognitive-Behavioural Model programme to improve Assertiveness, Coping and Empathy.
There was an observed trend in results for gender where no study in this review seemed to have accounted for gender differences (counterbalance the number of male and female participants) and only seven intervention programmes (Coelho and Murta, 2007; Murta and Tróccoli, 2004, 2007; Pinheiro et al., 2006; Pivaral et al., 2015; Pureza et al., 2012; Quiceno et al., 2011) were delivered to a mixed sample. Of those, the number of female participants (N=277) outstood males (N=108) by more than double, and the variables of interest manipulated included Assertiveness, Coping, Empathy, Gratitude and/or Resilience as primary or secondary outcome measures. Three programmes were specifically delivered for women (Cruz-Almanza et al., 2006; Rocha et al., 2013; Vera-Villarroel et al., 2005) (N=76),aiming to improve Assertiveness, Coping, Empathy and/or Optimism, whereas one intervention programme specific for men (Borges and Seidl, 2014) (N=13) focused on Assertiveness and Empathy. Five studies (Cuadra-Peralta et al., 2012; Espín-Andrade, 2009; Murta and Tróccoli, 2007, 2009; Toledo et al., 2011) failed to provide information of participant's gender, including the variables Assertiveness, Coping, Gratitude, Forgiveness and Optimism. Participants' ages in the reviewed papers ranged between 17 and 82 years of age for mixed sample designs. Within the intervention programmes delivered to female participants, age ranged from 25 to 60, whereas to males age ranged from 62 to 78. On the whole, only one study did not provide details of sample Mean age (Espín-Andrade, 2009).
The majority of participants included in the studies were identified as low to middle socioeconomic status (SES). Interventions were conducted in university settings (Borges and Seidl, 2014; Coelho and Murta, 2007; Murta and Tróccoli, 2009; Pureza et al., 2012), community centres (Cruz-Almanza et al., 2006; Cuadra-Peralta et al., 2012), schools (Pinheiro et al., 2006; Rocha et al., 2013; Vera-Villarroel et al., 2005), hospital setting (Murta and Tróccoli, 2004), health centres (Espín-Andrade, 2009; Toledo et al., 2012; Quiceno et al., 2011) and government workplaces (Murta and Tróccoli, 2007; Pivaral et al., 2015).
Time frame choice for assessing outcomes and lasting effects
Intervention programmes duration varied expressively amongst the reviewed studies ranging from one week to a one-year period (see Table 2). Eight studies utilized quantitative design in which programmes lasted from 1-18 weeks. Of those, six studies included pre-test - post-test evaluations and reported post-test at: 18 weeks (Cruz-Almanza et al., 2006) and at eight weeks (Toledo et al., 2011) to improve Assertiveness and Coping; at ten weeks (Pureza et al., 2012) for Assertiveness and Empathy; at one week (Vera-Villarroel et al., 2005) in a brief intervention to improve Assertiveness and Optimism; and at six weeks in two interventions, one to promote Assertiveness, Gratitude and Resilience (Quiceno et al., 2011), and another to improve Forgiveness, Gratitude and Optimism (Cuadra-Peralta et al., 2012). Overall, all variables of interest for this review (Assertiveness, Coping, Empathy, Forgiveness, Gratitude, Optimism and Resilience) were covered by different quantitative designs.
Of the six qualitative studies assessed, intervention lengths ranged between nine weeks to six months, including the variables Assertiveness, Coping and Empathy. Post-test assessments in qualitative designs were reported in only four studies at: six months (Rocha et al., 2013) in an intervention to improve Assertiveness, Coping and Empathy; at 12 weeks (Murta and Tróccoli, 2007) for Assertiveness and Coping; and at four months (Borges and Seidl, 2014), and at 11 weeks (Pinheiro et al., 2006) in different interventions to promote Assertiveness and Empathy. One qualitative study to improve Assertiveness and Coping for caregivers of demented elderly people (Espín Andrade, 2009) did not provide information of intervention length and/ or long-term main effects. The most enduring programme reviewed (Murta and Tróccoli, 2004) presented a mixed design (qualitative-quantitative) and lasted for 48 weeks to improve hospital workers' Assertiveness and Coping skills. The results reported by this study include participants' levels of satisfaction and dissatisfaction with the intervention, thus lacking evidence of outcome variables and intervention main effects.
Out of the only four studies reviewed that reported follow-up assessment for long-term effects, a social skills educational programme for mothers of ADHD children (Rocha et al., 2013) did not state follow-up length and was found to improve Assertiveness, Coping and Empathy at T2. A psycho-education intervention to promote Assertiveness and Empathy in elderly males (Borges and Seidl, 2014) reported follow-up at four months with lasting effects for both variables in only 31% (N=4) of participants. A brief intervention for Assertiveness, Gratitude and Resilience in chronically ill patients reported lasting effects for Resilience at three months (Quiceno et al., 2011), whereas a CBT intervention for abused women reported follow-up at three, six and 18 months, focusing on Assertiveness and Coping (Cruz-Almanza et al., 2006). Results for this intervention showed improvements in coping strategies at T2 (three months), T3 (six months) and T4 (18 months), and in Assertiveness at T1 (post-test), T2 (three months) and T3 (six months).
Standardized instruments most frequently selected as outcome measure and sensitivity to change after program delivery
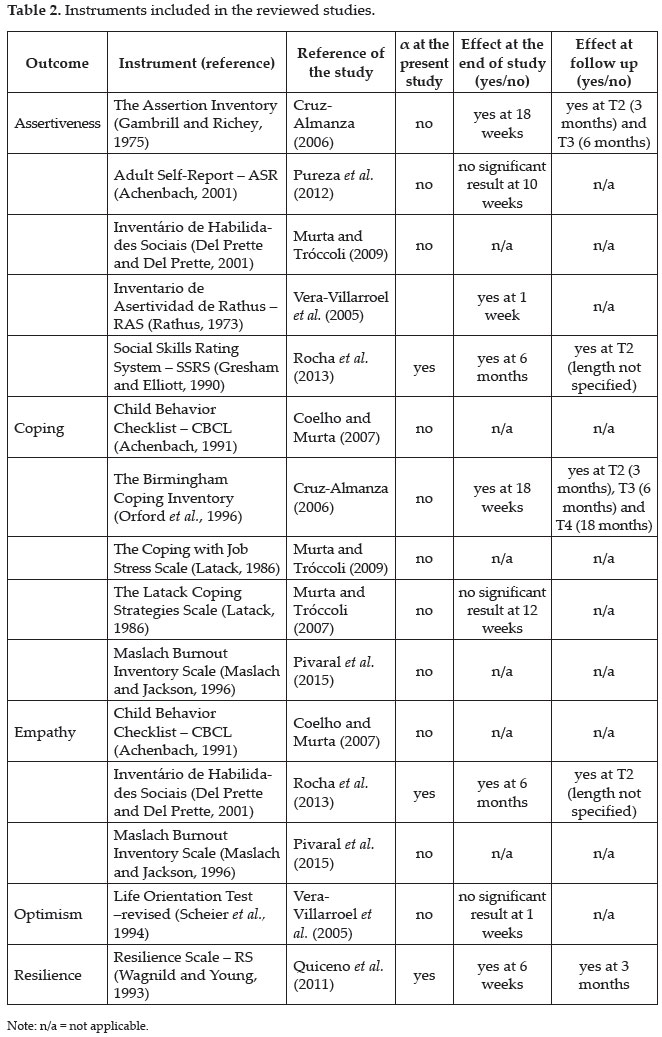
The most commonly used instruments reported in the reviewed papers for the assessment of each variable, as well as instruments' sensitivity to detect changes are described in Table 3. The instruments were classified according to the type of outcome they were subject to measure, and sensitivity effects identified at post-test and at follow up assessments.
It is worth noting that the only instrument used to evaluate Optimism was the Life Orientation Test (LOT) (Scheier et al., 1994, in Vera-Villarroel et al., 2005). Likewise, Resilience was measured by the Resilience Scale (RS) (Wagnild and Young, 1993 in Quiceno et al., 2011). No study reported to have made use of valid and/or reliable instrument to measure Gratitude or Forgiveness, and the assessment of these outcome variables were based on qualitative methods. Three instruments (Inventário de Habilidades Sociais; Child Behavior Checklist - CBCL; Maslach Burnout Inventory Scale) were utilized to measure more than one variable of interest across different studies. Those were the Inventário de Habilidades Sociais for the assessment of Assertiveness (Murta and Tróccoli, 2009) and Empathy (Rocha et al., 2013); the Child Behavior Checklist - CBCL to assess Coping (Coelho and Murta, 2007) and Empathy (Coelho and Murta, 2007); and the Maslach Burnout Inventory Scale was also used to evaluate Coping and Empathy (Pivaral et al., 2015). Only two studies carried out evaluations of reliability levels (Cronbach Alpha) of instruments chosen to ensure internal consistency at the time of the study and for that particular sample (Quiceno et al., 2011; Rocha et al., 2013).
In a similar manner only three studies out of 15, reported the reliability of the instruments within the sample of the intervention. Likewise, only six out of 15 measures were able to detect change after intervention (i.e., The Assertion Inventory; Rathus Assertiveness Schedule; Social Skills Rating System; The Birmingham Coping Inventory; Inventário de Habilidades Sociais; Resilience Scale).
Discussion
Considering the impact of EBPP for long-term public healthcare decisions, allocation of resources and personnel, the limited number of programme interventions studies (i.e., 10) included in this review that carried out internal rigorous manipulation checks (assessment at baseline and post-intervention) for programme efficacy leads to the conclusion that, there is lacking evidence to support the effects of Psychological programmes implemented to promote human strengths in Latin America. In a similar manner, a common rule for the assessed papers was lack of follow-up assessment (included in only four studies), which conceals the real power to detect intervention effects in the long-term and/or intervention efficacy. In this case, conclusions regarding interventions' in this review are drawn from the few studies that included pre-test - post-test (ten studies) and follow-up evaluations (four studies). The overall picture, at present, indicates that strength-based intervention programmes implemented in Latin America would benefit from more structured methodological procedures, including strict outcome measure analysis, also stating clear which variable(s) has/ have presented expected or unexpected significant changes following programmes' implementation and final assessments.
The same applies to detected significant results other than the ones predicted by programmes' main objectives. That is, studies should make clear any significant changes due to interaction effects from primary outcome measures, resulting in unexpected significant results for secondary outcome measures, which was a common trait amongst the evaluated studies. Yet the sum of evidence compiled from the reviewed studies indicate that 73.3% of programmes evaluated aimed to improve Assertiveness, 46.6% Coping, 40% Empathy, 13.3% of programmes addressed Gratitude and Optimism and 6.6% included Forgiveness and Resilience as outcome variables. Nevertheless, without rigor at baseline and subsequent assessments (including specific cutting-points for follow-up studies) based on guidelines for programme's efficacy, it is not feasible to point out the extent to which interventions managed to achieve their proposed objectives.
Additionally, the studies reviewed presented different degrees of research design quality. The majority of studies did not achieve criteria for well-established treatments according to the American Psychological Association guidelines (APA, 2002) (i.e. required two studies or more using between subject design, done by different researchers in order to demonstrate the superiority of the treatment under study to a placebo, or a different treatment, OR its equivalence in outcome to another established empirically supported treatment). That is, two experimental studies demonstrating superiority to no treatment or alternative treatments OR equivalence of the evaluated treatment outcome to an empirically supported treatment. Such treatments employed must also be manualized to allow replication in different settings. All the mentioned treatment guidelines were violated or absent in the published papers included in this review. Thus, based on APA guidelines (APA, 2002) for treatment control and implementation, design quality or the assessed papers generally remained unsatisfactory.
Also in terms of empirical quality, none of the studies reviewed controlled effects by gender, age or participants' SES over the results. In that, high levels of gender/age disparity resulted in strength-based programmes being predominantly delivered to female participants, aged from 25 to 60, for the variables Assertiveness, Coping, Empathy, Gratitude, Resilience and/or Optimism. As well as inferred unsuitable control of sampling methods, the high index of female participants detected across studies could have also been due to the fact that women are known to be more compliant with treatments and more likely to seek help, whereas men tend to generally be more resistant to adopt a support-seeking role (Sarafino and Smiths, 2014). Recent findings in this direction indicate that self-reliance, as well as traditional masculinity, may function as mediating variables for men look after their health, keep regular attendance to physician, adhere to treatment and health promoting behaviours (Murray-Law, 2011). Once male participants were underrated in the majority of studies, health providers should bear in mind the extent of influence of additional psychological and cultural variables that could go against and prevent individuals from, primarily identifying their need of assistance, and, ultimately take part in health-related intervention programmes. This concern should be accounted for in the design process of programmes, also considering which variables should be more appropriately addressed for a 'male-oriented programme', and methodological processes of sampling selection. This may help reduce the likelihood of leaving out those participants who might need the most. With regard to the programmes reviewed delivered to male participants, the variables worked included Assertiveness, Coping, Empathy, Gratitude and Resilience for a sample aged 62 to 78. However, taking the number of studies that failed to inform participants' gender and/or age (overall six studies), generalization of results is very limited.
In a similar manner, the majority of papers covered samples of low to middle SES, nonetheless, mostly comprised of employed individuals. That is, participants that presented some degree of social interactions and/or socioeconomic security. Put another way, despite being classified as low-middle SES, this sample (employed individuals) may present advantages when compared to retired, or unemployed participant samples (Talbott, 2009). The latter tend to, for instance, lack or perceive reduction in socioeconomic stability, social interactions/support, present reduced autonomy and increased levels of anxiety and depression, all of which result in being a more at risk (high vulnerability) population (Goldman-Mellor, 2015). At present, interpretations in this review also suggest insufficient number of programmes being delivered to more vulnerable populations such as unemployed or even retired individuals, and people who live in peripheral areas and do not have access to social mechanisms (community or health centres, main hospitals, universities, etc).
Extrapolating from the results, thus, it is possible to identify considerable bias in the delivery of strength-based programmes, with less emphasis being given to the promotion of health via intervention programmes to those unable to access health services or take part in interventions sponsored by workplaces. It is also true that healthcare providers and services should invest in the dissemination of education for health practices (Albee, 1982; Zimmerman, 2004) via manualized (standardized) interventions, allowing widespread replication and diffusion of health knowledge/ information, in order to reach ample spheres of society. This would include those kept apart from mainstream centres, or those who do not have means to participate in health interventions otherwise.
In terms of quality of outcome measures presented by each study, only five variables of interest for this review (Assertiveness, Coping, Empathy, Optimism and Resilience) were evaluated by means of standardized instruments. Researchers are prioritizing ad hoc instruments (or qualitative observations) over proper validated measures. However, one should note the importance of having validated and reliable instruments for the assessment of subjective constructs in Psychological science (Carretero-Dios and Pérez, 2007). In this perspective, the selection criteria for instruments utilized across studies were not fully detailed. In that, the reliability level (e.g., Cronbach's alpha) of the target measurements utilized was omitted in various studies, as well as missing evaluations (not carried out) for internal consistency of instruments at the time of the study, and for that particular sample. This may hamper conclusions on the adequacy of instruments chosen to evaluate different variables of interest in the reviewed studies. Hence, positive changes in outcome variables reported following intervention programmes that were assessed by means of unreliable instruments, should be interpreted carefully. An optimistic take on this would be to accept that the majority of studies reported significant changes for at least one variable, whereas a realistic take would also concern the inflation of Type I error due to inadequate measurement as opposed to interventions' efficacy (Shaughnessy et al., 2012).
Thus, much of the reported studies would be considered pilot or feasibility studies, however continuity of the studies was not found. Researchers must persevere in replicating and perfecting interventions. A single study does not allow practitioners to believe in the efficacy of interventions, and even less credibility may be given to effectiveness claims. The identified studies would be much more properly labelled as pilot or even feasibility studies, as opposed to trials to infer the efficacy or effectiveness of interventions (Bowen et al., 2009; Lancaster, 2015). Researchers within Latin America should consider in more detail the guidelines for intervention development and outcome assessment. As a limitation of the present review is the possible risk of bias assessment, once the processes of data selection and evaluation was further checked by and independent researcher form the same institution as the first author. This could arguably result in a tendency to assess studies in a similar perspective/paradigm, narrowing the scope of critical judgements in terms of studies methodological quality and adequacy to be included in the review. Future investigations could include a team of professionals from different health spheres, and/or also different approaches in Psychology.
To conclude, despite the methodological limitations identified in the reviewed studies, it is important to note that strength-based intervention programmes are generally reported to result in increased levels of life satisfaction and emotional well-being (Cuadra-Peralta et al., 2012), satisfaction with the intervention itself (Murta and Trócolli, 2004) and social interactions (Espín-Andrade, 2009; Murta and Trócolli, 2009), all as positive side-effects of participation. Through the results from this review it is highlighted caution in designing methodologically viable programmes, including explicitly benefits and risks analysis (APA, 2002), the main objectives expected to be achieved and: (a) for which outcome variables; (b) for which target population; (c) what outcome measures be used, followed by empirical support for this decision; (d) introduce baseline, post-test and follow-up assessment as a norm, to allow inference of interventions efficacy in the long-term; and (e) provide instruction manuals or guides, so that others may implement the programme in different settings, and for different samples; (f) state suggestions and future indications for prospective research and practice in the fields; would all be valuable contributions for the implementation of strength-based programmes interventions in Latin America.
As an additional challenge is the need to design cultural-sensitive intervention programmes that contemplate individuals who do not necessarily fit in the 'normal' plot. In other words, designing strength-based programmes addressed and sensitive to marginalized, peripheral individuals, who in the majority of cases end up being deprived from participation due to not having access to health services, not being part of the productive sphere of society (not employed or active labours), or social mechanisms in workplaces at all. This was also true for the absence in literature of strength-based programmes being delivered to same sex couples in Latin America. Thus, taking the cultural and socioeconomic reality in Latin America, at present, cultural-specific sensitivity, along with methodological rigor during the design, implementation and posterior outcome evaluations of health intervention programmes may be highlighted as a must for an incipient evidence-based Psychological science in Latin America.
Acknowledgements
This study was partially funded by The Brazilian National Counsel of Technological and Scientific Development (CNPq) through the doctoral grant to the author.
A kind thanks and appreciation to the independent researcher, who contributed to methodological enrichment of this article.
References
ALBEE, G.W. 1982. Preventing psychopathology and promoting human potential. American Psychologist, 37:1043-1050. https://doi.org/10.1037/0003-066X.37.9.1043 [ Links ]
AMERICAN PSYCHOLOGICAL ASSOCIATION (APA). 2002. Criteria for evaluating treatment guidelines. American Psychologist, 57:1052-1059. https://doi.org/10.1037/0003-066X.57.12.1052 [ Links ]
AMERICAN PSYCHOLOGICAL ASSOCIATION (APA). 2006. Evidence-based practice in psychology: APA presidential task force on evidence-based practice. American Psychologist, 61:271-285. https://doi.org/10.1037/0003-066X.61.4.271 [ Links ]
ASPINWALL, L.G.; STAUDINGER, U.M. 2013. A psychology of human strengths: Fundamental questions and future directions for a positive psychology. Washington, American Psychological Association, 369 p. [ Links ]
AUSTRALIAN PSYCHOLOGICAL SOCIETY (APS). 2010. Evidence-based psychological interventions in the treatment of mental disorders: a literature review. 3rd ed., Melbourne, The Australian Psychological Society Ltd., 173 p. [ Links ]
BABOR, T.F.; CAETANO, R. 2005. Evidence-based alcohol policy in the Americas: strengths, weaknesses, and future challenges. Revista Panamericana de Salud Pública, 18(4-5):327-337. https://doi.org/10.1590/S1020-49892005000900013 [ Links ]
BARRA S.; ELORZA-RICART J.M.; SÁNCHEZ E. 2008. Instrumento para la lectura crítica y la evaluación de estudios epidemiológicos transversales. Gaceta Sanitaria, 22(5):492-497. https://doi.org/10.1157/13126932 [ Links ]
BORGES, L.M.; SEIDL, E.M.F. 2014. Hábitos saudáveis na velhice: efeitos de uma intervenção psicoeducativa com homens idosos. Psicologia, Saúde & Doenças, 15(2):468-481. https://doi.org/10.15309/14psd150211 [ Links ]
BOWEN, D.J.; KREUTER, M.; SPRING, B.; COFTA-WOERPEL, L.; LINNAN, L.; WEINER, D.; BAKKEN, S.; KAPLAN, C.P.; SQUIERS, L.; FABRIZIO, C.; FERNANDEZ, M. 2009. How We Design Feasibility Studies. American Journal of Preventive Medicine, 36(5):452-457. https://doi.org/10.1016/j.amepre.2009.02.002 [ Links ]
BUSCH, A.K.; SPIRIG, R.; SCHNEPP, W. 2014. Coping with multiple sclerosis in partnerships: a systematic review of the literature. Der Nervenarzt, 85(6):727-737. https://doi.org/10.1007/s00115-014-4017-7 [ Links ]
CARRETERO-DIOS, H.; PÉREZ, C. 2007. Standards for the development and review of instrumental studies: considerations about test selection in psychological research. International Journal of Clinical and Health Psychology, 7(3):863-882. [ Links ]
COELHO, M.V.; MURTA, S.G. 2007. Treinamento de pais em grupo: um relato de experiência. Estudos de Psicologia, 24(3):333-341. https://doi.org/10.1590/S0103-166X2007000300005 [ Links ]
COREN, E. 2013. Interventions for promoting reintegration and reducing harmful behaviour and lifestyles in street-connected children and young people: a systematic review. Cochrane Database of Systematic Reviews, CD009823(3):1-129. https://doi.org/10.4073/csr.2013.6 [ Links ]
CORRÊA, C.I.M. 2008. Habilidades sociais e educação: programa de intervenção para professores de uma escola pública. Universidade Estadual Paulista-UNESP, 1:12-140. [ Links ]
CRUZ-ALMANZA, M.A.; GAONA-MÁRQUEZ, L.;SÁNCHEZ-SOSA, J.J. 2006. Empowering women abused by their problem drinker spouses: effects of a cognitive-behavioral. Salud Mental, 29(5):25-31. [ Links ]
CUADRA-PERALTA, A.; VELOSO-BESIO, C.; PUDDU-GALLARDO, G.; SALGADO-GARCÍA, P.; PERALTA-MONTECINOS, J. 2012. Impacto de un programa de psicología positiva en sintomatologia depresiva y satisfaccion vital en adultos mayores. Psicologia: Reflexão e Crítica, 25(4):644-652. https://doi.org/10.1590/s0102-79722012000400003 [ Links ]
EMMONS, R.A.; MCCULLOUGH, M.E. 2003. Counting blessings versus burdens: an experimental investigation of gratitude and subjective well-being in daily life. Journal of Personality and Social Psychology, 84(2):377-389. https://doi.org/10.1037/0022-3514.84.2.377 [ Links ]
ESPÍN ANDRADE, A.M. 2009. "Escuela de Cuidadores" como programa psicoeducativo para cuidadores informales de adultos mayores con demencia. Revista Cubana de Salud Pública, 35(2). [ Links ]
FALCONE, E. 1999. Avaliação de um programa de treinamento da empatia com universitários. Revista Brasileira de Terapia Comportamental e Cognitiva, 1:23-32. [ Links ]
GAMBRILL, E.D.; RICHEY, C.A. 1975. An assertion inventory for use in assessment and research. Behavior Therapy, 6(4):550-561. https://doi.org/10.1016/S0005-7894(75)80013-X [ Links ]
GARCÍA-LLANA, H.; REMOR, E.; DEL PESO, G.; SELGAS, R. 2014. The role of depression, anxiety, stress and adherence to treatment in dialysis patients' health-related quality of life: a systematic review of the literature. Revista Nefrología, 34(5):637-57. [ Links ]
GOLDMAN-MELLOR, S.J. 2015. Unemployment and mental health. Encyclopedia of Mental Health, p. 350-355. [ Links ]
GRENARD, J.L.; AMES, S.L.; PENTZ, M.A.; SUSSMAN, S. 2006. Motivational interviewing with adolescents and young adults for drug-related problems. International Journal of Adolescent Medicine and Health, 18(1):53-67. https://doi.org/10.1515/IJAMH.2006.18.1.53 [ Links ]
HASSIOTIS, A.; HALL, I. 1996.Behavioural and cognitive-behavioural interventions for outwardly-directed aggressive behaviour in people with learning disabilities. Reviews, 33(3):91-106. [ Links ]
HEALTH PROMOTION INTERNATIONAL (HPI). 2014. Health Promotion International, 29(1):195-197. https://doi.org/10.1093/heapro/dat095 [ Links ]
JACK, L.; GRIM, M.; AULD, M.E. 2012. Health promotion practice expands focus on global health promotion. Health Promotion Practice, 13(3):289-292. https://doi.org/10.1177/1524839912443244 [ Links ]
KELM, Z.; WOMER, J.; WALTER, J.K.; FEUDTNER, C. 2014. Interventions to cultivate physician empathy: a systematic review. BMC Medical Education, 14(1):219. https://doi.org/10.1186/1472-6920-14-219 [ Links ]
LANCASTER, G.A. 2015. Pilot and feasibility studies come of age! Pilot and Feasibility Studies, 1(1). https://doi.org/10.1186/2055-5784-1-1 [ Links ]
LI, Q.; LOKE, A.Y. 2014. A systematic review of spousal couple-based intervention studies for couples coping with cancer: direction for the development of interventions. Psycho-Oncology, 23(7):731-739. https://doi.org/10.1002/pon.3535 [ Links ]
LINLEY, A.P.; MALTBY, J.; WOOD, A.M.; JOSEPH, S.; HARRINGTON, S.; PETERSON, C.; PARK, N.; SELIGMAN, M.E.P. 2007. Character strengths in the United Kingdom: The VIA inventory of strengths. Personality and Individual Differences, 43:341-351. https://doi.org/10.1016/j.paid.2006.12.004 [ Links ]
LIVINGSTONE, N.; MACDONALD, G.; CARR, N. 1996. Restorative justice conferencing for reducing recidivism in young offenders. Cochrane Database of Systematic Reviews, p. 1-17. [ Links ]
MASTEN, A.S. 2014. Ordinary magic. Resilience in development. New York, Guilford Press, 147 p. [ Links ]
MURRAY-LAW, B. 2011. Why do men die earlier? Monitor on Psychology, 42(6):58-63. [ Links ]
MURTA, S.G.; TRÓCCOLI, B.T. 2009. Intervenções psicoeducativas para manejo de estresse ocupacional: um estudo comparativo. Revista Brasileira de Terapia Comportamental e Cognitiva, 11(1):25-42. [ Links ]
MURTA, S.G.; TRÓCCOLI, B.T. 2004. Avaliação de intervenção em estresse ocupacional. Psicologia: Teoria e Pesquisa, 20(1):39-47. https://doi.org/10.1590/s0102-37722004000100006 [ Links ]
MURTA, S.G.; TRÓCCOLI, B.T. 2007. Stress ocupacional em bombeiros: efeitos de intervenção baseada em avaliação de necessidades. Estudos de Psicologia, 24(1):41-51. https://doi.org/10.1590/S0103-166X2007000100005 [ Links ]
MYTTON, J.A.; DIGUISEPPI C.; GOUGH, D.A.; TAYLOR, R.S.; LOGAN, S. 2002. School-based violence prevention programs: systematic review of secondary prevention trials. Archives of Pediatrics and Adolescent Medicine, 156(8):752-762. https://doi.org/10.1001/archpedi.156.8.752 [ Links ]
NORMAN, E. 2000. Resiliency enhancement: Putting the strengths perspective into social work practice. New York, Columbia University Press, 40 p. https://doi.org/10.7312/norm11800 [ Links ]
PINHEIRO, M.I.S.; HAASE, V.G.; DEL PRETTE, A.; AMARANTE, C.L.D.; DEL PRETTE, Z.A.P. 2006. Treinamento de habilidades sociais educativas para pais de crianças com problemas de comportamento. Psicologia: Reflexão e Crítica, 19(3):407-414. https://doi.org/10.1590/s0102-79722006000300009 [ Links ]
PIVARAL, C.E.C.; CRUZ, L.K.R.; GUILLERMO J.; GONZÁLEZ PÉREZ, G.J.; VEGA LÓPEZ, M.G.; FIGUEROA, I.V. 2015. Efecto de una intervención psicoeducativa para disminuir el Síndrome Burnout en personal de confianza de La Comisión Federal de Electricidad. Salud Mental, 3:215-221. [ Links ]
PUREZA, J.R.; RUSCH, S.G.S.; WAGNER, M.; OLIVEIRA, M.S.O. 2012. Treinamento de habilidades sociais em universitários: uma proposta de intervenção. Revista Brasileira de Terapias Cognitivas, 8(1):2-9. [ Links ]
QUICENO, J.M.; VINACCIA, S.; REMOR, E. 2011. Programa de potenciación de La resiliencia para pacientes com artritis reumatoide. Revista de Psicopatología y Psicología Clínica, 16(1):27-47. https://doi.org/10.5944/rppc.vol.16.num.1.2011.10349 [ Links ]
ROCHA, M.M.; DEL PRETTE, Z.A.P.; DEL PRETTE, A. 2013. Avaliação de um programa de habilidades sociais educativas para mães de crianças com TDAH. Acta Comportamentalia, 21(3):359-375. [ Links ]
SARAFINO, E.P.; SMITHS, T.W. 2014. Health Psychology. Biopsycho social interactions. 8th ed., New Jersey, Library of Congress Cataloging-in-Publication Data, 16 p.
SCHEIER, M.F.; CARVER, C.S.; BRIDGES, M.W. 1994. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. Journal of Personality and Social Psychology, 67(6):1063-1078. https://doi.org/10.1037/0022-3514.67.6.1063 [ Links ]
SELIGMAN, M.E.P. 2002. Authentic happiness: using the new positive psychology to realize your potential for lasting fulfillment. New York, Free Press, 125 p. [ Links ]
SELIGMAN, M.E.P.; CSIKSZENTMIHALYI, M. 2000. Positive psychology: An introduction. American Psychologist, 55(1):5-14. https://doi.org/10.1037/0003-066X.55.1.5 [ Links ]
SHAPIRO, S.L.; SHAPIRO, D.E.; SCHWARTZ, G.E. 2000. Stress management in medical education: a review of the literature. Academic Medicine, 75(7):748-759. https://doi.org/10.1097/00001888-200007000-00023 [ Links ]
SHAUGHNESSY, J.J.; ZECHMEISTER, E.B.; ZECHMEISTER, J.S. 2012. Research Methods in Psychology. 9th ed., New York, McGraw Hill, 341 p. [ Links ]
SHULTS, R.A.; ELDER, R.W.; NICHOLS, J.L.; SLEET, D.A.; COMPTON, R.; CHATTOPADHYAY, S.K. 2009. Effectiveness of multicomponent programs with community mobilization for reducing alcohol-impaired driving. American Journal of Preventive Medicine, 37(4):360-371. https://doi.org/10.1016/j.amepre.2009.07.005 [ Links ]
SCHWARTZ, R. 2000. Health promotion practice: advancing the state of health promotion and education practice. Health Promotion Practice, 1(1):5-9. https://doi.org/10.1177/152483990000100101 [ Links ]
SNYDER, C.R.; LOPEZ, S.J. 2007. Positive Psychology: The scientific and practical explorations of human strengths. New York, Sage Publications, 69 p. [ Links ]
STRAUB, R. 2012. Health Psychology. A Biopsychological approach. 3rd ed., New York, Worth Publishers, 359 p. [ Links ]
TALBOTT, J.A. 2009. Case-control study of unemployment and parasuicide. Yearbook of Psychiatry and Applied Mental Health, 48(6):511-515. https://doi.org/10.1016/s0084-3970(08)79148-5 [ Links ]
TOLEDO, Y.C.; CARDOSO, L.F.; AMADOR, A.T.; PÉREZ, O.M.; REYES, A.G. 2011. Programa para estimular autocontrol emocional en población laboral con ansiedad del área previsora. Municipio Camagüey. Revista Humanidades Médicas, 5(3):1-17. [ Links ]
TRIVEDI, D. 2015. Cochrane review summary: barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: qualitative evidence synthesis. Primary Health Care Research & Development, 16(04):326-328. https://doi.org/10.1017/S1463423615000341 [ Links ]
VERA-VILLARROEL, P.; VALENZUELA, P.; ABARCA, O.; RAMOS, N. 2005. Evaluación de una intervención conductual intensa y breve para el manejo de estados emocionales: un estudio piloto. Acta Colombiana de Psicología, 13:121-131. [ Links ]
WARD, T.; DURRANT, R. 2013. Altruism, empathy, and sex offender treatment. International Journal of Behavioral Consultation and Therapy, 8(3-4):66-71. https://doi.org/10.1037/h0100986 [ Links ]
ZIMMERMAN, M. 2004. Health education and behavior.Health Education & Behavior,31(6):657-657. https://doi.org/10.1177/109019810403100601 [ Links ]
Submetido: 28/07/2016
Aceito: 13/10/2016


{kind=link}
{kind=link}
{kind=link}
{kind=link}