











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo

 Permalink
Permalink
INTRODUCTION
Down syndrome is the most common genetic cause of intellectual disability. Its incidence, in different populations, varies from 1 in 319 to 1 in 1000 live births1,2. Down syndrome is related to maternal age and has increased worldwide3. Down syndrome is caused by a complete or partial trisomy of chromosome 214. In Brazil, the incidence is one case of Down syndrome for every 600 to 800 live births5-7.
Down syndrome presents several brain alterations, such as maturation of the central nervous system, degenerative processes of the nervous system, regulation of neuronal apoptosis, and reduction in the release of neurotransmitters. This generates psychomotor delays (e.g., cognitive deficits), hindering learning, speech skills, and gross and fine motor gestures8. According to Menghini et al., (2011), short- and long-term memory performance, as well as visual-perceptual abilities, are impaired due to the dysfunction of different parts of the brain9.
Individuals with Down syndrome need assistance in playing, understanding the rules of a game, and interacting with others10,11. These problems explain intellectual disability and reduced social skills12, because social interaction is an important variable for a child’s overall development. Social interaction begins in childhood, within the family, and in other environments (e.g., neighborhood, daycare, and kindergarten), and the conditions of the environments influence the quality of subsequent interpersonal relationships. As such, the child with special educational needs will relate to himself according to the environment13.
According to Moriyama et al., (2019), children and adolescents with Down syndrome need more time to acquire functional skills, and it is essential to offer assistance as soon as possible by parents, caregivers, and professionals. This suggests the need for professional support that is not restricted to school activities14. One of the ways to help in the development of these individuals is through technologies capable of including and generating social interaction15, such as learning games, which enable cognitive and motor stimuli16-18.
Assistive technology to aid literacy and communication of individuals with intellectual disabilities is being widely applied, however, little attention is being paid to augmented reality games19. According to Menezes et al., (2015), individuals with Down syndrome respond positively to tasks that are different and complementary to conventional therapy, especially therapy involving virtual reality20 or augmented reality21,22.
The use of augmented reality in serious games allows the creation of learning situations and user immersion. This combination can even increase learning rate gains21. Games such as MoviLetrando and total reaction time (TRT_S 2012 Software), proved to be useful as a support in education, as they help to improve the cognitive, motor, and literacy skills of people with intellectual disability22, autism spectrum disorder, and elderly23,24. Therefore, the aim of the present study is to compare statistical differences in learning between individuals with Down syndrome and individuals with typical development using augmented reality games.
METHODS
Ethical aspects
This study was approved by the Ethics Committee of Centro Universitário FMABC (report number: CAAE 54605616.5.0000.0082). All participants signed the free consent in informed consent. Participants < 18 old accepted to participate through the informed free assent in informed consent and, in this case, their parents signed the consent form.
Eligibility criteria
We included individuals diagnosed with Down syndrome, for the experimental group, and with typical development, for the control group, who were able to understand the instructions regarding the proposed task in each game and perform the necessary movement (without motor impairment of the limbs superiors). We excluded individuals who could not understand the guidelines regarding the proposed task, had some limitation of movement of the upper limbs and/or limitation in visual acuity that prevented them from playing the game, those who could not or did not want to complete the proposed task or who reported pain or discomfort while playing the games.
Participants
Participants were 46 individuals with Down syndrome, 20 females with a mean age of 21.1 years (SD=8.0); range 7–35 years; 26 males with a mean age of 21.1 years (SD=7.0); range 8–31 years; and 46 individuals with typical development, 25 females, with a mean age of 21.1 years (SD=7.0); range 7–33 years; 21 males, with a mean age of 19.3 years (SD=9.4); range of 8–39 years.
Participants in the experimental group (Down syndrome) were recruited from two associations that offer specialized educational services for people with intellectual disabilities, located in the cities of Vitória and Vila Velha, Espírito Santo, Brazil, São Paulo–SP. Participants in the control group (typical development) were recruited from two public schools located in Potim City, SP, Brazil.
Assessments and instruments
MoviLetrando game
A computer game that creates mirror images so participants can see themselves on the screen. Developed at the Visual Applications Research Laboratory at the State University of Santa Catarina, Brazil25,26. MoviLetrando makes use of augmented reality based on projection using a webcam, as presented by Guarnieri et al.,22. A face-to-face learning computer program that involves interacting with a virtual symbol projected onto the screen; letters of the alphabet (vowels and/or consonants) and numbers (1 to 10). The software allows the therapist or education professional to control nine different phases such as alphabet, numbers, and sets. In each phase, the software offers several levels of difficulty (generation of symbols on the left side, on the right side, or on both sides; increase/decrease the number of symbols; increase/decrease the size of the symbols; increase/decrease the display of symbols). In this study, we used two phases (an alphabetical phase, with vowels, and a numerical phase).
Game shows a symbol (alphabet or number according to the phase) at the top center of the screen (figure 1) and the participant must reach the same symbol, moving their hands in the virtual environment. The total game time is defined at the beginning and can vary from 2 to 5 min, in this study, 2 min were used. The score that each participant achieved is determined by whether participants reached a symbol, whether it was correct, and the time taken to complete each task.

TRT_S2012 Software
Total reaction time (TRT_S 2012 Software) was built and validated by Crocetta et al.,27. This software consists of promoting stimuli in the form of a yellow square in the center of the computer screen at previously defined time intervals. Participants must react as quickly as possible by pressing the space bar on the computer keyboard. The software records the time between the appearance of the stimulus and pressing the space bar (figure 2).
Procedures
All participants performed the same research protocol involving two instruments without any previous practice. Sitting in front of a laptop, in a quiet room, they started with 14 attempts at TRT_S2012, followed by 4 min practicing MoviLetrando games, 2 min in the alphabetical phase using vowels (Phase A-5), and 2 min in the numerical phase (Phase C-5). After this practice, all participants finished the protocol with another 14 attempts on TRT_S2012. During the practice of MoviLetrando, in the alphabetical phase (Phase A-5), two vowels were presented on each side of the participant, and only one is the target vowel. In the numerical phase, three numbers were displayed on each side of the participant and only one number is the target.
Statistical analysis
Data were presented as mean ± standard deviation (SD) and analyzed using IBM-SPSS for Windows software (version 20; IBM Corporation). The normality of data distribution was not confirmed with the Shapiro-Wilk test. Mann–Whitney U test of independent samples was performed to analyze differences between groups for the total score, number of correct answers, incorrect answers, omitted answers, and mean time to reach the symbols in both phases. Non-parametric Wilcoxon tests were performed for group comparisons. Spearman’s rank-order correlation coefficient was used to investigate correlations among age, sex, and reaction time.
RESULTS
Ninety-two (n = 92) participants met the inclusion and exclusion criteria. Namely, 46 in the Down syndrome group and 46 in the typical development group. There were no significant differences between the characteristics of individuals with Down syndrome and typical development (table 1).
Table 1 Characteristics of all participants
| Variables | Down syndrome (n=46) | Typical development (n=46) | p-value |
|---|---|---|---|
| Sex (% female) | 43.5 | 54.3 | U = 0.30 |
| Age, mean (standard-deviation) | 21.1 (7.4) | 20.3 (8.1) | |
| Median (years) | 21.0 | 19.0 | U = 0.43 |
| Range of age (years) | 7-35 | 7-39 |
U: Mann–Whitney U test.
In testing the hypothesis that the Down syndrome and typical development groups differ in game performance, we used the Mann–Whitney U test to test the differences in all variables generated by the MoviLetrando game (table 2) and the performance of the total reaction time (TRT), generated by the TRT_S2012 Software.
Table 2 : Mean (standard-deviation) of the total score, individual answers, and mean time to reach the symbols, in the alphabetic and numerical phases of the MoviLetrando game. In the last two rows of the table the TRT was performed before and after the MoviLetrando phases
| MoviLetrando variables | DS (n=46) | TD (n=46) | Outcomes (DS x TD) |
|---|---|---|---|
| Alphabetical phase | |||
| Total score | 56.6 (23.2) | 93.7 (18.8) | U (92)=1915; p<0.001 |
| Correct | 6.6 (3.5) | 13.0 (2.7) | U (92)=1949; p<0.001 |
| Incorrect | 5.7 (2.9) | 1.4 (1.3) | U (92)=144.5; p<0.001 |
| Omitted | 1.3 (1.6) | 0.1 (0.4) | U (92)=548; p<0.001 |
| Mean time (seconds) | 6.2 (0.7) | 5.6 (0.7) | U (92)=363.5; p<0.001 |
| Numerical phase | |||
| Total score | 44.0 (18.1) | 86.2 (19.5) | U (92)=1951; p<0.001 |
| Correct | 4.6 (2.9) | 11.9 (2.9) | U (92)=1991.5; p<0.001 |
| Incorrect | 6.7 (3.6) | 1.7 (1.5) | U (92)=214.5; p<0.001 |
| Omitted | 1.8 (1.7) | 0.3 (0.6) | U (92)=434; p<0.001 |
| Mean time (seconds) | 6.4 (0.8) | 5.9 (0.7) | U (92)=605; p<0.001 |
| Total reaction time (seconds) | |||
| TRT before | 2.6 (1.2) | 0.4 (0.1) | U (87)=1.0; p<0.001 |
| TRT after | 1.9 (1.0) | 0.4 (0.1) | U (85)=58.5; p<0.001 |
DS: Down syndrome group; TD: typical development group; U: Mann–Whitney U test.
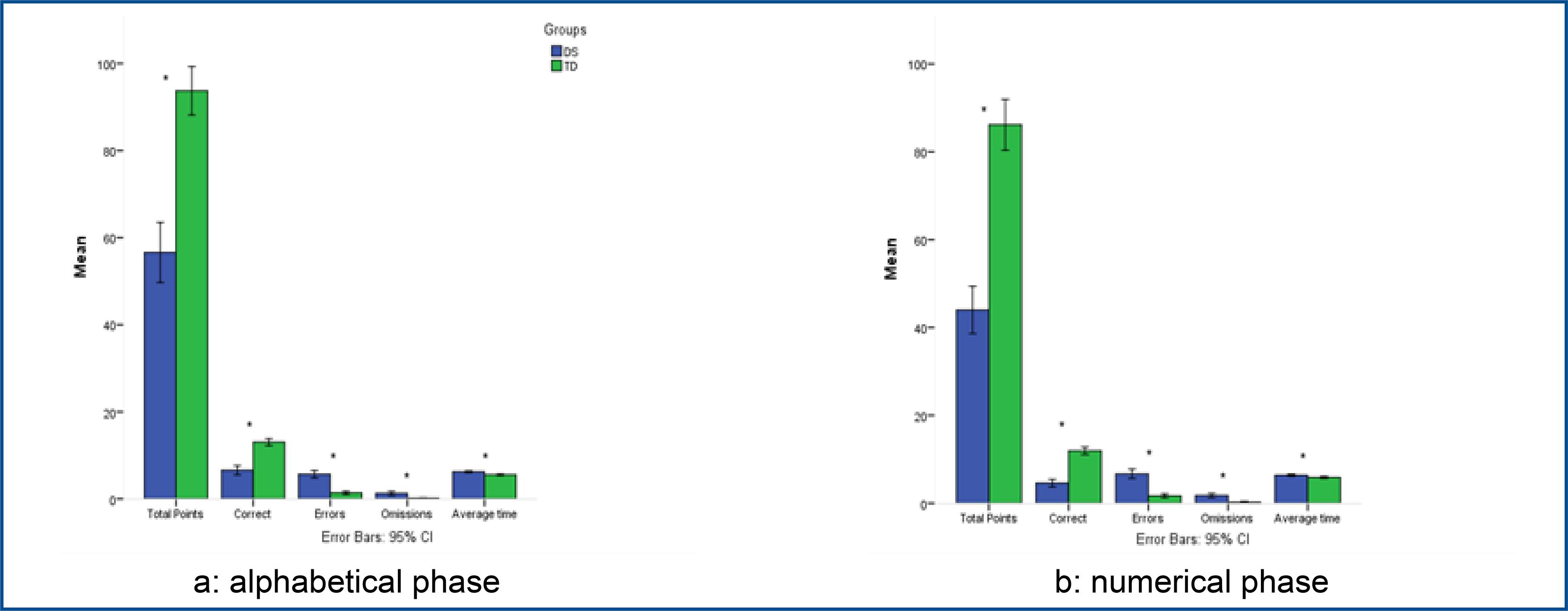
Means and standard deviations of the total score in the alphabetic (AP) and numerical (NP) phases of the MoviLetrando game indicated that the highest number of correct symbols was achieved by children with typical development (M = 13.0, M = 11.9) when compared to those with Down syndrome (M = 6.6, M = 4.6) for AP and NP, respectively. Significant differences were found among all the variables provided by the MoviLetrando game in both phases of the game (table 2). It was verified that the performance of Down syndrome is low when compared to the participants with typical development.
Results indicated that participants in both groups were more accurate in identifying alphabetic symbols when compared to numerical symbols (table 3), with a high total score and correct symbols and low errors, omissions, and mean time to reach the symbols. This suggests a possible greater complexity in the numerical phase (figure 3).
Table 3 : Total score, individual answers, and mean time to reach the symbols, in the alphabetic and numerical phases of the MoviLetrando game. In the last column the differences between TRT performance before and after the MoviLetrando game
| Total score | Correct | Incorrect | Omitted | Mean time | TRT | |
|---|---|---|---|---|---|---|
| (AP x NP) | (AP x NP) | (AP x NP) | (AP x NP) | (AP x NP) | (B x A) | |
| DS | W=242.5 | W=121.0 | W=667.5 | W=460.0 | W=619.0 | W=97.0 |
| p=0.001 | p<0.001 | p=0.042 | p=0.095 | p=0.391 | p<0.001 | |
| TD | W=185.0 | W=185.0 | W=441.5 | W=47.0 | W=889.0 | W=540.0 |
| p<0.001 | p=0.001 | p=0.080 | p=0.193 | p<0.001 | p=0.996 |
DS: Down syndrome group; TD: typical development group; W: Wilcoxon Signed-Rank Test; AP: alphabetical phase; NP: numerical phase; TRT: total reaction time; B: before; A: After.
Source: Prepared by the authors
Figure 3 : Mean and standard-deviation of the total score, individual answers, and mean time to reach the symbols during phases (a) alphabetic and (b) numerical. The symbol * indicates a group difference between the Down syndrome and typical development groups at p < 0.05
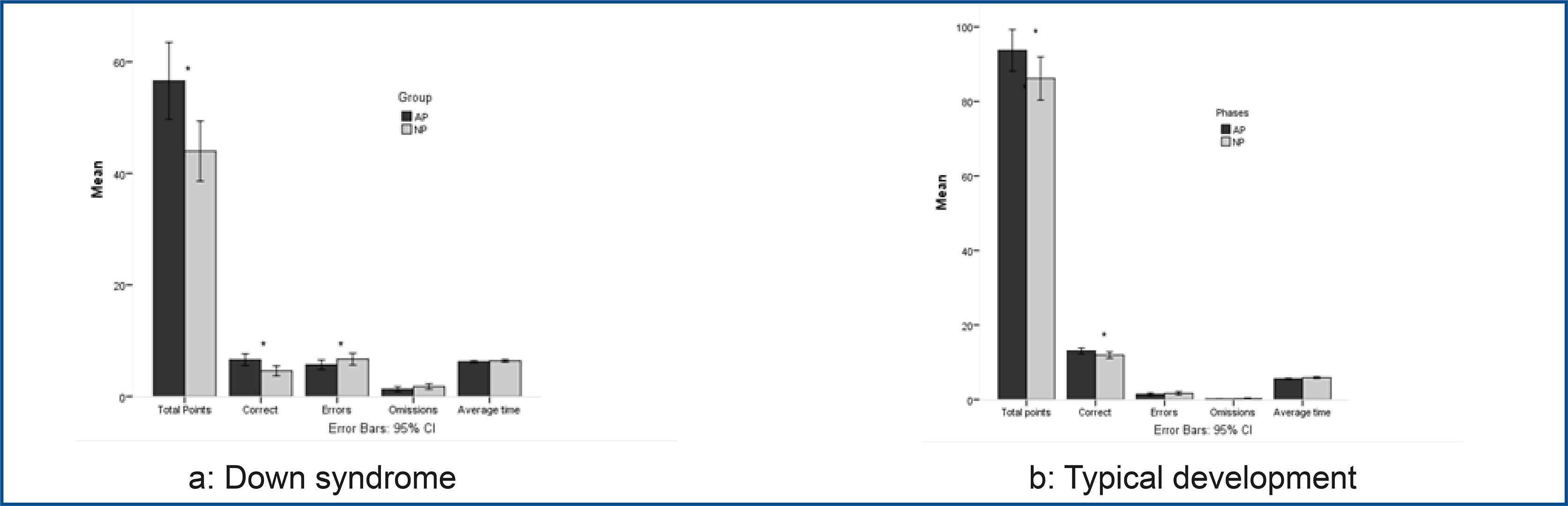
Inspection of performance at the alphabetic and numeric phases suggested that accuracy declined in both groups, suggesting that the increase in the number of symbols to be reached may have played a role in how accurately participants correctly discriminated between the correct number to reach.
Summarizing, we can say that accuracy in both groups was sensitive to the number of symbols presented in each phase. The Down syndrome group had a lower performance when compared to the typical development group. Reaction time in the MoviLetrando and TRT_S2012 tests were examined for correlations with age and gender (table 4).
Table 4 Spearman correlations on the time to reach the symbols and other measures of MoviLetrando
| Variables | Age | Sex | TRT before | Time AP | Time NP | TRT after |
|---|---|---|---|---|---|---|
| Age | 0.03 | 0.06 | -0.18 | 0.02 | 0.11 | |
| Sex | -0.15 | -0.15 | 0.17 | 0.38** | 0.01 | |
| TRT before | -0.25 | -0.06 | 0.10 | 0.05 | 0.62** | |
| Time AP | -0.16 | -0.04 | 0.08 | 0.20 | 0.39* | |
| Time NP | -0.34* | 0.00 | 0.21 | 0.67** | -0.10 | |
| Time after | -0.38** | -0.01 | 0.77** | 0.21 | 0.40** |
Correlations are presented above the diagonal for the Down syndrome group and below for the typical development group. Time AP: mean time to reach a symbol in the alphabetical phase; Time NP: mean time to reach a symbol in the numerical phase; TRT: total reaction time. * p <0.05 (two-tailed); ** p <0.01 (two-tailed).
Source: Prepared by the authors
Figure 4 : Mean and error bars of the total score, individual answers, and mean time to reach symbols during the alphabetical and numerical phases for Down syndrome (a) and typical development (b) groups. The * symbol indicates a significant difference between the AP and NP phases at p < 0.05
There were no significant correlations of time to reach the symbol in the MoviLetrando game (phases AP and NP) and TRT before this execution, however, there was a significant correlation of TRT afterward with AP for the Down syndrome group, and NP for the typical development group.
DISCUSSION
In this study, we found differences in performance between the groups. Both groups showed a similar pattern of decreased performance between the alphabetical and numerical phases. Antao et al.,28 show similar outcomes when evaluating a population with autism spectrum disorder, in which the autism spectrum disorder group, the results showed that in PN the performance was lower when compared to AP. They suggested that the task demanded by numbers presented a more difficult target and that this was the reason for the lower performance.
According to Favero et al.,29, children with Down syndrome have more difficulties in acquiring numerical skills than reading and writing skills. Thus, the acquisition of mathematical concepts and mathematical activities becomes complex for individuals with Down syndrome. According to Farias et al.,25, as the number of generated symbols increases, the player is faced with situations in which he needs to reflect and develop less obvious movements to reach a certain letter that may be “behind” another letter, making the game more demanding in terms of the visual-motor aspect. Perhaps this explains the reason the typical development group also performed less well on the numerical symbol task.
There are need of effective intervention proposals, aiming at the acquisition of different areas of knowledge to improve the treatment quality and rehabilitation30 31 . Farias et al.,25 emphasize that the use of serious games with virtual reality technologies seems to be the appropriate type of software capable of promoting stimulation and adaptability and, at the same time, entertainment and playfulness.
In this study, participants with Down syndrome improved their reaction time after performing the virtual reality projection game task, while the typical development group maintained the same reaction time. Similar results were found in the study by Antão et al.,28, who used a total reaction time task before and after the augmented reality game application in a population with autism spectrum disorder. It was observed that only the experimental group showed improvement.
In the study by Herrero et al.32, the reaction time performance was investigated in participants of two groups, autism spectrum disorder, and typical development, after a virtual reality task (coincident time task) the results showed that the training had a positive influence on the reaction time of both groups, being typical development of greater expression.
CONCLUSION
The use of augmented reality games has clinical utility and functional benefits for people with Down syndrome. We noticed significant differences between the groups in the total points scored, correct symbols, and errors in the two phases. The total points for the control group were higher when compared to the group of individuals with Down syndrome.

