











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo

 Permalink
Permalink
INTRODUCTION
In Brazil, existing evidence primarily concentrates on individual states1-6 or compares states within specific geographic regions7. However, there’s a gap in research that directly compares states from different geographical areas. To address this and comprehensively monitor the evolving landscape of the COVID-19 pandemic in Brazil, along with the associated response measures, the COVID-19 Brazil/Ireland Observatory was established. This initiative is led by the Study Design and Scientific Writing Laboratory at the FMABC University Center. COVID-19 is identified as a metabolic disorder caused by the SARS-CoV-2 virus and is associated with severe acute respiratory syndrome (SARS). Predominant symptoms include fever (≥ 37.8°C), cough, myalgia, fatigue, headache, dyspnea, upper respiratory, and gastrointestinal manifestations. The Ministry of Health designates flu syndrome as the most prevalent presentation, potentially progressing to pneumonia and SARS, characterized by respiratory distress and oxygen saturation levels falling below 95%. Elevated levels of angiotensin-converting enzyme 2 (ACE2), particularly in individuals with underlying health conditions, are correlated with respiratory symptoms8-10.
The SARS-CoV-2 virus was initially identified in the central region of China, specifically in the city of Wuhan, in December 2019. Demonstrating high transmissibility, it profoundly affected global health and the economy. Responding swiftly to the escalating situation, the World Health Organization (WHO) declared it a pandemic. In light of the increasing global cases, the WHO issued health recommendations, urging countries to adopt containment strategies and protective measures. These measures encompassed social distancing, quarantine protocols, the closure of educational institutions such as schools and universities, and the implementation of remote work policies11-12.
This virus is highly contagious, and one of the main transmission routes includes direct contact with airborne droplets released during conversation, coughing, and sneezing from infected people. However, recent research suggests that the virus also can spread by air via aerosols13.
According to data from the World Health Organization (WHO) on Coronavirus - COVID-19, as of March 5, 2023, there have been 759,408,703 confirmed cases of COVID-19 globally, with 6,866,434 documented deaths attributed to the disease14. In February 2020, Brazil reported its initial confirmed case of COVID-19. Despite three years of sustained efforts to combat the pandemic, Brazil currently holds the unfortunate distinction of having the highest number of COVID-19 deaths globally, second only to the United States of America15. Given the elevated rate of spread, incidence, and mortality associated with COVID-19, managers of the Unified Health System (SUS) and their teams must formulate effective strategies for dealing with the situation. Developing comprehensive risk management plans at the national, state, municipal, and local levels is crucial. Understanding regional factors that influence the contagion and spread of the virus is essential in this endeavor. Additionally, employing time series studies is instrumental in analyzing the evolving patterns and behavior curves of the pandemic16. Hence, the objective of this study is to analyze the incidence, mortality, and lethality rates of COVID-19 in the States of Pará and Rio Grande do Sul and the trends of these key indicators over the period from 2020 to 2022.
METHODS
It is a Population-based ecological study with time series analysis. Time series are necessary to make valid inferences from the data, accounting for the correlation between repeated observations over time17.
The analysis of indicators for each State followed the protocol by Elmulsharaf and Siqueira (2021)18 with official secondary data from government public disclosure. The database was extracted from the electronic pages made available by the Ministry of Health19 of the States of Pará and Rio Grande do Sul. All cases confirmed by laboratory, clinical, clinical-epidemiological, or/and clinical-imaging diagnosis of COVID-19 from February 2020 to December 2022 were included. The disease was classified according to the International Classification of Diseases, 10th edition (ICD-10), as “U07.1 COVID-19 – identified virus” or “U07.2 COVID-19, unidentified virus”20. Cases without information on the date of notification or death were excluded.
Cases were classified based on the date of notification and fatal cases according to the date of death.
Characterization of the study site
Pará and Rio Grande do Sul, situated in distinct geographical regions, possess unique territorial attributes. Figure 1 depicts the map illustrating the geographic positioning of each state, and table 1 outlines the key sociodemographic features specific to each region.
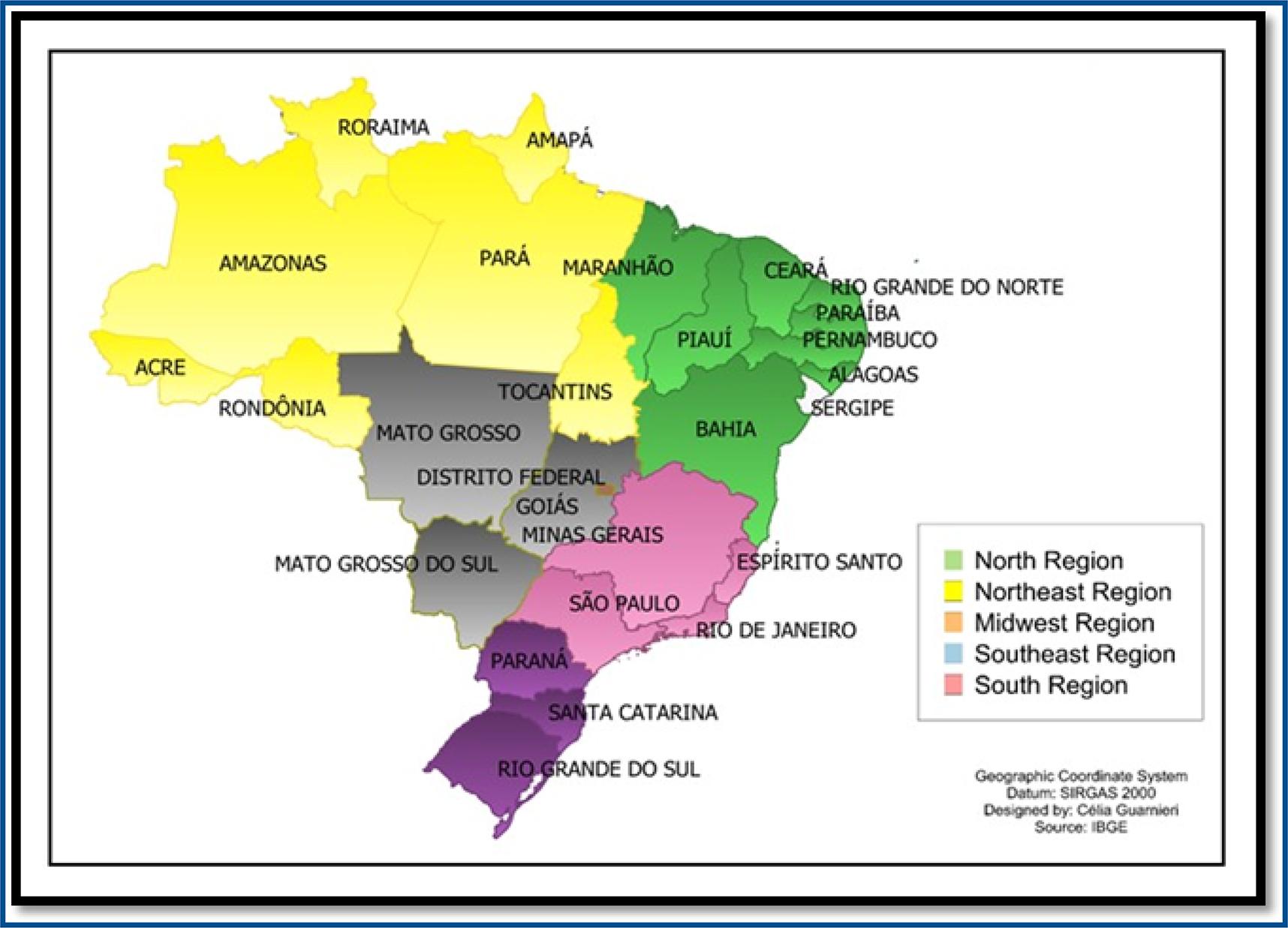
Table 1 : Sociodemographic characteristics of Brazil and the States of Pará and Rio Grande do Sul according to the last Census carried out in Brazil in 2010
| Sociodemographic characteristics | Description | |||
|---|---|---|---|---|
| BRASIL | PARÁ | RIO GRANDE DO SUL | ||
| Region | North | Soulth | ||
| Number of municipalities | 5.570 | 144 | 497 | |
| capital | Brasília | Belém | Porto Alegre | |
| Territorial Extension (2021) - KM2 | 8.510.345,54 | 1.245.870,70 | 281.707,15 | |
| Population (Last Census 2010) - People | 190.755.799 | 7.581.051 | 10.693.929 | |
| Estimated population (2021) | 213.317.639 | 8.777.124 | 11.466.630 | |
| Demographic Density (Last Census, 2010) - Inhabitants/km2 | 22,43 | 6,07 | 37,96 | |
| Per capita home monthly monthly income | R$ 1.625,00 | R$ 1.061,00 | R$ 2.087,00 | |
| Human Development Index (HDI) (Last Census, 2010) | 0,699 | 0,646 | 0,746 | |
| Basic Health Units of the Unique Health System - SUS (2009)* | 63.184 | 2.300 | 3.868 | |
| establishments | Ambulatory SUS* | 52.394 | 2.019 | 3.066 |
| SUS Dialysis* | 923 | 16 | 81 | |
| SUS Emergency* | 5.553 | 210 | 327 | |
| SUS Internment* | 5.415 | 218 | 324 | |
| SUS ICU/CTI* | 1.099 | 25 | 71 | |
| Number of beds for hospitalization in health facilities (2009)* | 431.996 | 13.720 | 31.055 | |
| beds | Public* | 152.892 | 5.830 | 4440 |
| Private* | 279.104 | 7.890 | 26615 | |
Source: Brazilian Institute of Geography and Statistics (IBGE, 2021)21. Note 1: 2010 Census; SUS=Unified Health System.
Statistical analysis of data
The number of COVID-19 cases and deaths were described by absolute (n) and relative frequency (%).
The incidence rate (number of cases per 100.000 inhabitants), mortality (number of deaths per 100.000 inhabitants), and lethality (%) were calculated for each State as described in the formulas (1), (2), and (3):
The study considered the Population Projection of the Federation Units from 2000 to 2060 to determine the number of inhabitants. Specifically, population estimates for 2020, 2021, and 2022 were utilized. This approach ensures a comprehensive understanding of the impact of the pandemic on these regions relative to their demographic dynamics during the specified timeframe22.
Prais-Winsten regression was applied to examine indicator trends, and the daily percentage change (DPC) was determined to classify trends as increasing, decreasing, or stationary. Stationary trends were considered when p>0.05.
We followed the methodological guidelines proposed by Antunes and Cardoso (2015)23 for the construction of time series, considering a significance level of 95%, according to the equations below (1), (2), and (3):
Where β is the linear regression slope, the indices ul mean the upper limit, and ll is the lower limit of the confidence level.
Statistical analyses were performed using STATA 14.0 software (College Station, TX, USA 2013).
Legal and ethical aspects
The data obtained from the information systems maintained by the State Health Department are official, enabling their use as a feasible tool for analyzing the epidemiological indicators of COVID-19. As this is public and widely accessible data without patient identification, the Scientific Research Ethics Committee does not need to assess this research, respecting the institutional precepts of resolution 466/12.
RESULTS
In the State of Pará, from January 2020 until December 2022, a total of 860,013 cases and 21,504 deaths were recorded through the Ministry of Health’s Coronavirus Panel.
The first cases confirmed by COVID-19 in March 2020 correspond to <0.001% of the total cases throughout the analyzed period. As for deaths, the first records appeared in April of the same year, corresponding to a relative frequency of 0.96% of deaths. In 2020, the state of Pará reported a total of 29,352.9 confirmed cases and 718.3 deaths due to COVID-19. Notably, the months with the highest confirmed cases were June (7.586%), July (5.985%), and August (5.217%). Regarding deaths, the standout months were May (12.625%), June (9.286%), and July (3.757%).
Moving to 2021, the number of cases and deaths in Pará amounted to 27,618.08 and 1,038, respectively. March, April, and May were significant months for both confirmed cases and deaths, representing 6.148%, 6.283%, and 5.238% of the total cases, and 20.414%, 11.881%, and 7.082% of the total deaths during the specified period.
In 2022, the number of COVID-19 cases in Pará was 19,588.92, with 155.41 deaths. January emerged as a notable month, contributing to 2.577% of the total cases, followed by February with 8.277% and July with 3.278%. Regarding deaths, the months of January, February, and March were significant, representing relative frequencies of deaths equivalent to 1.181%, 2.120%, and 1.362%, respectively.
Table 3 shows the monthly distribution of cases and deaths confirmed by COVID-19 in Pará and Rio Grande do Sul over time (2020 to 2022).
Table 3 : Monthly distribution of cases and deaths confirmed by COVID-19 in the States of Pará and Rio Grande do Sul, Brazil, from January 2020 to December 2022
| Year | Month | Confirmed Cases | Confirmed Deaths | ||
|---|---|---|---|---|---|
| absolut frequency (n) | relative frequency (%) | absolut frequency (n) | relative frequency (%) | ||
| PARÁ | |||||
| 2020 | January | 0 | 0 | 0 | 0 |
| February | 0 | 0 | 0 | 0 | |
| March | 21 | 0,002 | 0 | 0 | |
| April | 2.844 | 0,330 | 208 | 0,960 | |
| May | 35.085 | 4,079 | 2.715 | 12,625 | |
| June | 65.245 | 7,586 | 1.997 | 9,286 | |
| July | 51.479 | 5,985 | 808 | 3,757 | |
| August | 44.871 | 5,217 | 418 | 1,943 | |
| September | 30.893 | 3,592 | 427 | 1,985 | |
| October | 22.470 | 2,612 | 165 | 0,767 | |
| November | 17.629 | 2,049 | 172 | 0,799 | |
| December | 22.992 | 2,673 | 273 | 1,269 | |
| Total 2020 | 293.529 | 34,125 | 7.183 | 33,391 | |
| 2021 | January | 35.260 | 4,099 | 448 | 2,083 |
| February | 35.337 | 4,108 | 955 | 4,441 | |
| March | 52.880 | 6,148 | 4.390 | 20,410 | |
| April | 54.036 | 6,283 | 2.555 | 11,880 | |
| May | 45.055 | 5,238 | 1.523 | 7,082 | |
| June | 36.323 | 4,223 | 965 | 4,487 | |
| July | 19.519 | 2,269 | 579 | 2,692 | |
| August | 11.341 | 1,318 | 405 | 1,883 | |
| September | 7.521 | 0,874 | 205 | 0,953 | |
| October | 7.097 | 0,825 | 87 | 0,404 | |
| November | 10.281 | 1,195 | 155 | 0,720 | |
| December | 16.767 | 1,949 | 189 | 0,878 | |
| Total 2021 | 331.417 | 38,529 | 12.456 | 57,913 | |
| 2022 | January | 22.165 | 2,577 | 254 | 1,181 |
| February | 71.187 | 8,277 | 456 | 2,120 | |
| March | 34.651 | 4,029 | 293 | 1,362 | |
| April | 11.629 | 1,352 | 175 | 0,813 | |
| May | 9.113 | 1,059 | 106 | 0,492 | |
| June | 8.173 | 0,950 | 90 | 0,418 | |
| July | 28.194 | 3,278 | 80 | 0,372 | |
| August | 21.015 | 2,443 | 192 | 0,892 | |
| September | 7.986 | 0,928 | 117 | 0,544 | |
| October | 4.854 | 0,564 | 35 | 0,162 | |
| November | 7.046 | 0,819 | 35 | 0,162 | |
| December | 9.054 | 1,052 | 32 | 0,148 | |
| Total 2022 | 235.067 | 27,328 | 1.865 | 8,666 | |
| Total triennium | 860.013 | 100,00 | 21.504 | 100,00 | |
| RIO GRANDE DO SUL | |||||
| 2020 | January | 0 | 0 | 0 | 0 |
| February | 33 | 0,001 | 0 | 0 | |
| March | 1.264 | 0,043 | 4 | 0,009 | |
| April | 3.607 | 0,123 | 60 | 0,144 | |
| May | 10.175 | 0,347 | 182 | 0,437 | |
| June | 25.581 | 0,873 | 440 | 1,057 | |
| July | 57.060 | 1,948 | 1.391 | 3,344 | |
| August | 62.303 | 2,127 | 1.606 | 3,861 | |
| September | 48.290 | 1,649 | 1.282 | 3,082 | |
| October | 57.298 | 1,956 | 1.000 | 2,404 | |
| November | 121.909 | 4,163 | 1.167 | 2,805 | |
| December | 123.048 | 4,202 | 2.111 | 5,075 | |
| Total 2020 | 510.568 | 17,432 | 9.243 | 22,218 | |
| 2021 | January | 93.303 | 3,186 | 1.776 | 4,269 |
| February | 189.941 | 6,487 | 2.048 | 4,923 | |
| March | 200.621 | 6,852 | 8.445 | 20,303 | |
| April | 96.858 | 3,308 | 4.534 | 10,900 | |
| May | 136.372 | 4,657 | 2.964 | 7,126 | |
| June | 104.827 | 3,580 | 2.895 | 6,960 | |
| July | 46.802 | 1,598 | 1.697 | 4,079 | |
| August | 31.093 | 1,061 | 796 | 1,913 | |
| September | 26.665 | 0,910 | 616 | 1,480 | |
| October | 31.607 | 1,079 | 664 | 1,596 | |
| November | 18.519 | 0,632 | 595 | 1,430 | |
| December | 19.411 | 0,662 | 257 | 0,617 | |
| Total 2021 | 996.019 | 34,012 | 27.287 | 65,593 | |
| 2022 | January | 559.912 | 19,123 | 678 | 1,630 |
| February | 237.036 | 8,095 | 1.431 | 3,440 | |
| March | 52.772 | 1,802 | 606 | 1,456 | |
| April | 36.897 | 1,260 | 196 | 0,471 | |
| May | 115.364 | 3,940 | 293 | 0,704 | |
| June | 94.756 | 3,236 | 482 | 1,158 | |
| July | 87.758 | 2,997 | 425 | 1,021 | |
| August | 47.428 | 1,619 | 356 | 0,855 | |
| September | 9.543 | 0,325 | 180 | 0,432 | |
| October | 3.776 | 0,128 | 59 | 0,141 | |
| November | 39.493 | 1,348 | 72 | 0,173 | |
| December | 136.587 | 4,665 | 286 | 0,687 | |
| Total 2022 | 1.421.322 | 48,538 | 5.064 | 12,168 | |
| Total triennium | 2.927.909 | 100,00 | 41.594 | 100,00 | |
The first confirmed cases of COVID-19 in Rio Grande do Sul were registered in February 2020, corresponding to 0.001% of the total cases throughout the period analyzed, with the first death registered in March, representing 0.009 % of the total number of deaths about the period analyzed.
In 2020, the number of cases and deaths confirmed by COVID-19 was 42,547.33 and 770.25, respectively. The months with the highest number of cases were October (1,956%), November (4,163%) and December (4,202%). Regarding deaths, the months that stood out were July (3.344%), August (3.861%) and December (5.075%).
In 2021, the number of cases and deaths confirmed by COVID-19 was 83,001.58 and 2,273.91, respectively. February, March and May stand out for cases, being 6.487%, 6.852%, and 4.657%, respectively, concerning the total period. However, for deaths, the months with the highest number of records were March (20.303%), April (10.900%) and May (7.126%).
In 2022, until July, the number of cases and deaths confirmed by COVID-19 was 118,443.5 and 422, respectively. January represents 19.123% of the total cases, followed by February, 8.095%, and December, 4.665%. Regarding the deaths, the months with the highest number were January, February, and March, with the relative frequencies equivalent to 1.630%, 3.440%, and 1.456, respectively.
For both States, table 4 shows the mortality, lethality, and incidence rates of COVID-19.
Table 4 Monthly distribution of mortality, lethality and incidence rates of COVID-19 in the States of Pará and Rio Grande do Sul, Brazil, from January 2020 to July 2022
| Year | Month | PARÁ | RIO GRANDE DO SUL | ||||
|---|---|---|---|---|---|---|---|
| Mortality | Incedence | Letality | Mortality | Incedence | Letality | ||
| 2020 | January | 0 | 0 | 0 | 0 | 0 | 0 |
| February | 0 | 0 | 0 | 0 | 0,289 | 0 | |
| March | 0 | 0,37 | 0 | 0,035 | 11,071 | 0,316 | |
| April | 2,410 | 32,959 | 7,313 | 0,525 | 31,593 | 1,663 | |
| May | 31,464 | 406,598 | 7,738 | 1,594 | 89,122 | 1,788 | |
| June | 23,143 | 756,121 | 3,06 | 3,853 | 224,062 | 1,72 | |
| July | 9,363 | 596,588 | 1,569 | 12,183 | 499,785 | 2,437 | |
| August | 4,844 | 520,008 | 0,931 | 14,066 | 545,708 | 2,577 | |
| September | 4,948 | 358,017 | 1,382 | 11,228 | 422,9696 | 2,654 | |
| October | 1,97 | 260,403 | 0,734 | 8,758 | 501,87 | 1,745 | |
| November | 1,993 | 204,301 | 0,975 | 10,221 | 1067,795 | 0,957 | |
| December | 3,163 | 266,453 | 1,187 | 18,49 | 1077,771 | 1,715 | |
| Total 2020 | 83,301 | 3401,823 | 2,447 | 80,958 | 4472,039 | 1,81 | |
| 2021 | January | 5,143 | 410,614 | 1,27 | 15,52 | 815,388 | 1,903 |
| February | 11,56 | 414,506 | 2,702 | 17,897 | 1659,922 | 1,078 | |
| March | 21,066 | 607,092 | 8,301 | 73,802 | 1753,256 | 4,209 | |
| April | 29,332 | 620,364 | 4,728 | 39,623 | 846,456 | 4,681 | |
| May | 17,484 | 517,257 | 3,38 | 25,902 | 1191,775 | 2,173 | |
| June | 11,078 | 417,008 | 2,656 | 25,299 | 916,098 | 2,761 | |
| July | 6,647 | 224,089 | 2,966 | 14,83 | 409,009 | 3,625 | |
| August | 4,649 | 130,201 | 3,571 | 6,956 | 271,726 | 2,56 | |
| September | 2,353 | 86,345 | 2,725 | 5,383 | 233,029 | 2,31 | |
| October | 0,998 | 81,477 | 1,225 | 5,802 | 276,218 | 2,1 | |
| November | 1,779 | 118,031 | 1,507 | 5,199 | 161,84 | 3,212 | |
| December | 2,169 | 192,494 | 1,127 | 2,245 | 169,635 | 1,323 | |
| Total 2021 | 114,266 | 3819,484 | 3,758 | 238,465 | 8704,355 | 2,739 | |
| 2022 | January | 2,889 | 258 | 1,145 | 5,913 | 4883,363 | 0,121 |
| February | 5,188 | 809,943 | 0,64 | 12,48 | 2067,348 | 0,603 | |
| March | 3,333 | 394,248 | 0,845 | 5,285 | 460,259 | 1,148 | |
| April | 1,991 | 132,311 | 1,504 | 1,709 | 321,803 | 0,531 | |
| May | 1,206 | 103,684 | 1,163 | 2,555 | 1006,165 | 0,253 | |
| June | 1,023 | 92,989 | 1,101 | 4,203 | 826,429 | 0,508 | |
| July | 0,91 | 320,782 | 0,283 | 3,706 | 765,39 | 0,484 | |
| August | 2,184 | 239,102 | 0,913 | 3,104 | 413,65 | 0,75 | |
| September | 1,331 | 90,862 | 1,465 | 1,569 | 83,23 | 1,886 | |
| October | 0,386 | 55,227 | 0,721 | 0,514 | 32,932 | 1,562 | |
| November | 0,398 | 80,167 | 0,496 | 0,627 | 344,444 | 0,182 | |
| December | 0,364 | 103,013 | 0,353 | 2,494 | 1191,265 | 0,209 | |
| Total 2022 | 21,208 | 2680,333 | 0,793 | 44,166 | 12 396,289 | 0,356 | |
| Total triennium | 218,775 | 9901,641 | 2,5 | 363,59 | 25 572,683 | 1,42 | |
When comparing lethality between Para and Rio Grande do Sul, it was noted that during the period analyzed, the total rate remained higher in Pará, with April/2020 being highlighted (7.313% - 1.663 %), May/2020 (7.738% - 1.788%) and March/2021 (8.301% - 4.209%).
When comparing incidences, Rio Grande do Sul stands out compared to Pará, presenting the highest rates. In 2022, it was the highest incidence rate for COVID-19 in Rio Grande do Sul, with a total of 12,396.289/100,000 inhabitants, compared to a rate of 2,680.333/100,000 inhabitants in Pará. In 2020, the rate was higher by 1.31 times, and in 2021, the rate was 2.27 times higher.
Although lethality in Pará was higher throughout the period, mortality was higher in Pará than in Rio Grande do Sul only in 2020, reaching a rate of 83.301/100,000 inhabitants against 80.859/100,000 inhabitants. For 2021 and 2022, Rio Grande do Sul recorded a mortality rate of 2.08 and 2.09 times higher than Pará, respectively.
The trends in mortality, lethality, and incidence rates of COVID-19 in Pará and Rio Grande do Sul are shown in Table 5.
Table 5 : Estimates of Prais-Winsten regression and daily percentage variation (DPV) of mortality, lethality and incidence rates of COVID-19 in the States of Pará and Rio Grande do Sul, Brazil, from January 2020 to December 2022
| Rate/year | Pará | Rio grande do sul | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Linear regression | Linear regression | |||||||||
| β | P | VPD | 95%CI | Trend | β | P | VPD | 95% CI | Trend | |
| Mortality | ||||||||||
| 2020 to 2022 | -0.0011841 | <0.001 | -0.30 | -0.33: -0.21 | Descending | 0.0002123 | 0.630 | 0.05 | -0.15: 0.25 | Stationary |
| 2020 | -0.0013088 | 0.217 | -0.30 | -0.78: 0.18 | Stationary | 0.007 | <0.001 | 1.16 | 1.31: 2.02 | Growing |
| 2021 | -0.003438 | <0.001 | -0.80 | -0.99: -0.59 | Descending | -0.003 | <0.001 | -0.76 | -1.02: -0.50 | Descending |
| 2022 | -0.002467 | <0.001 | -0.60 | -0.70: -0.43 | Descending | -0.002 | <0.001 | -0.61 | -0.82: -0.40 | Descending |
| Lethality | ||||||||||
| 2020 to 2022 | -0.000641 | <0.001 | -0.20 | -0.19: -0.11 | Descending | -0.0006 | <0.001 | -0.14 | -0.20: -0.08 | Descending |
| 2020 | -0.003552 | <0.001 | -0.80 | -1.05: -0.58 | Descending | -0.0002 | 0.305 | -0.06 | -0.16: 0.05 | Stationary |
| 2021 | -0.000695 | 0.022 | -0.20 | -0.30: -0.02 | Descending | -0.0002 | 0.473 | -0.07 | -0.24: 0.11 | Stationary |
| 2022 | -0.000531 | 0.156 | -0.10 | -0.29: 0.05 | Stationary | 0.001 | 0.107 | 0.25 | -0.05: 0.56 | Stationary |
| Incidence | ||||||||||
| 2020 to 2022 | -0.000203 | 0.200 | -0.10 | -0.12: 0.02 | Stationary | 0.0009 | 0.122 | 0.22 | -0.06: 0.51 | Stationary |
| 2020 | 0.007291 | <0.001 | 1.69 | 0.82: 2.58 | Growing | 0.007 | <0.001 | 1.70 | 1.31: 2.09 | Growing |
| 2021 | -0.002774 | <0.001 | -0.60 | -0.64: -0.83 | Descending | -0.002 | <0.001 | -0.64 | -0.85: -0.43 | Descending |
| 2022 | -0.002247 | <0.001 | -0.50 | -0.52: -0.73 | Descending | -0.002 | 0.295 | -0.46 | -1.32: 0.41 | Stationary |
Mortality rates in 2020 showed an increasing trend in Rio Grande do Sul and remained stationary in Pará. In 2021 and 2022, the trends were decreasing for both states.
Lethality rates showed decreasing trends for 2020 and 2021 and remained stationary in 2022 in Pará; however, in Rio Grande do Sul, they remained stationary throughout the analyzed period (2020 to 2022).
Incidence rates showed increasing trends during 2020, both in Pará with a DPC of 1.69% (p <0.05) and 1.70% (p <0.05) in Rio Grande do Sul. In 2021, the incidence decreased (p <0.05) in both states, with a DPC of 0.60% in Pará and 0.64% in Rio Grande do Sul; and continued this trend in Pará in 2022 (DPC of -0.50% p <0.05), remaining stationary in Rio Grande do Sul, with a non-significant p-value (p> 0.05).
DISCUSSION
The distinct socioeconomic vulnerabilities in the North and South regions of Brazil underscore the need to identify factors influencing the evolution of COVID-19 epidemiological indicators. Understanding the unique pandemic situations in different states is crucial for devising effective disease control strategies. In this study, we delve into the analysis of COVID-19 incidence, mortality, and lethality in Pará and Rio Grande do Sul, examining trends from 2020 to 2022.
Throughout this period, both states confronted critical episodes. In Pará, a significant surge occurred between May and June 2020, marked by 5,520 deaths and 161,595 new cases of COVID-19. Meanwhile, in Rio Grande do Sul, another notable period unfolded between November and December, witnessing 3,278 deaths and 244,947 new cases. These episodes serve as pivotal points for understanding the dynamics and challenges faced by each state in managing the impact of the pandemic. The second critical period unfolded between March and May 2021 in Pará, witnessing a nearly doubling of both deaths and COVID-19 cases compared to the most critical period of the previous year. This significant surge played a decisive role in overwhelming the health system25, as previously analyzed concerning the capacity of hospital infrastructure to cope with the pandemic and the effectiveness of government actions in combating the pandemic26.
While scrutinizing the evolution of COVID-19 epidemiological indicators throughout 2020, 2021, and 2022 in Pará and Rio Grande do Sul, notable differences and distinctive aspects emerge. Each year unfolds a unique scenario, emphasizing the dynamic and evolving nature of the pandemic in these regions. In 2020, the peak number of COVID-19 cases in Pará was recorded in June (65,245), while in Rio Grande do Sul, it occurred in December (123,048). Despite the higher absolute numbers in Rio Grande do Sul, the incidence rate in Pará for the same period was 3,401.82 per 100,000 population, which was lower than that in Rio Grande do Sul, which reached 4,472.03 per 100,000. It’s noteworthy that both states reported incidence rates higher than the national average for this period, which stood at 3,129 per 100,000 population. This information underscores the variations in the spread of COVID-19 between these states during 2020.
In 2020, the incidence in Pará was still lower than the North region’s average (4,262.4/100,000 inhabitants). Notably, Roraima in the North region reported the highest incidence in the country, reaching 10,678 cases per 100,000 inhabitants. The seven states in the North region collectively accounted for 11.9% of the country’s total COVID-19 cases. Among these, the municipalities with the highest number of new cases were Manaus/AM (2,026), Belém/PA (1,686), and Boa Vista/RR (1,328). In July 2020, Pará held the fourth position with one of the highest COVID-19 case counts nationally. The findings from Lélis da Silva F. et al., (2021)27 highlight that the most significantly affected states in the North were Pará and Amazonas. According to the study, one week after the notification of the first case of COVID-19 in Pará, 0.82% of municipalities reported cases. This figure increased to 5.56% in the second week and substantially rose to 15.3% in the third week. Seven weeks after the initial case, 81.8% of municipalities had reported cases of COVID-19. The highest case numbers were concentrated in the capital’s metropolitan region, specifically in and around Belém.
Contrastingly, the incidence of COVID-19 in Rio Grande do Sul exceeded that of the South region (3,471.7/100,000), with Santa Catarina registering the highest incidence rate at 5,493.6 cases per 100,000 inhabitants. According to the Ministry of Health’s epidemiological bulletin (2020), by the end of the year, Rio Grande do Sul ranked as the third federative unit with the highest number of COVID-19 cases after São Paulo and Santa Catarina. Notably, there was an increase in the number of cases in Rio Grande do Sul (+26%), Santa Catarina (+16%), and Paraná (+11%), collectively representing 15.8% of total COVID-19 cases in Brazil. The municipalities with the highest frequency of new cases were Porto Alegre/Rio Grande do Sul (4,179), Joinville/SC (3,540), and Florianópolis/SC (2,627).
In terms of deaths, in 2020, Pará reported its highest number in May (2,715), while Rio Grande do Sul peaked in December (2,111). The mortality rate in Pará was 83.30 deaths per 100,000 inhabitants, and in Rio Grande do Sul, it was 80.95 deaths per 100,000 inhabitants. Notably, both states had lower mortality rates than the national average of 84 deaths per 100,000 inhabitants. Furthermore, Pará exhibited a lower mortality rate than the North region, with 92 deaths per 100,000 inhabitants. On May 6, the government of Pará declared a lockdown in the capital and in municipalities close to the metropolitan region to reduce human trafficking and try to control the spread of the pandemic27.
In contrast, Rio Grande do Sul had the highest mortality rate in the Brazilian South region. The municipalities with the highest number of deaths from COVID-19 were Porto Alegre, Curitiba, and Blumenau28.
The values of the number of cases and deaths impacted the trend behavior of the analyzed indicators; thus, it is observed that at the end of 2020, the incidence trend was increasing in both Pará and Rio Grande do Sul. Mortality was stationary in Pará and increasing in Rio Grande do Sul, with decreasing lethality in Pará and stationary in Rio Grande do Sul.
The evolution of epidemiological indicators in 2021 in Rio Grande do Sul was marked by an aggressive second wave of the pandemic, the implementation and progress of the vaccination program against COVID-19 conducted by the Unified Health System (Sistema Único de Saúde - SUS), and at the end of December the arrival of the Omicron variant.
The quarter formed by March, April, and May 2021 recorded the highest volume of cases and deaths in Pará and Rio Grande do Sul of the entire period analyzed (table 2). These numbers coincide with national data; in fact, on March 23, 3,251 deaths were recorded in one day in Rio Grande do Sul. One month later, on April 8, Brazil sadly registered a new record in the number of fatalities, recording 4,249 deaths from COVID-19 in 24 hours in Rio Grande do Sul, according to data from CONASS (2021)29.
Table 2 : projection of the population of Brazil and Federation Units by sex and age for the period 2010-2060 (2018 edition)
| Federation Region/Unit | 2020 | 2021 | 2022 |
|---|---|---|---|
| North Region | 18.672.591 | 18.906.962 | 19.133.894 |
| For | 8.690.745 | 8.777.124 | 8.861.974 |
| South Region | 30.192.315 | 30.402.587 | 30.606.047 |
| Rio Grande do Sul | 11.422.973 | 11.466.630 | 11.507.906 |
Source: IBGE/Research Directorate. Population Coordination and Social Indicators. Management of Studies and Analysis of Demographic Dynamics (DATASUS, 2023)21,22.
In the subsequent months, from June to November 2021, both Pará and Rio Grande do Sul experienced a decline in cases and deaths from COVID-19. This reduction can be attributed to the consistent implementation of non-pharmacological measures and the successful coverage of the vaccination program in these states. The combination of ongoing public health measures and widespread vaccination played a crucial role in mitigating the impact of the virus during this period.
However, mortality and incidence in 2021 were higher in Rio Grande do Sul than in Pará. The higher incidence rates of COVID-19 in Rio Grande do Sul compared to Pará in 2021 and 2022 were divergent from other studies. The highest incidence rates of COVID-19 occurred in Brazil’s North and Northeast regions, where areas with lower human development converge7.
Pará initiated its vaccination program on January 19, 2021. By September 24 of the same year, it had achieved a vaccination rate of 46.04% for the first dose and 29% for the second or single dose. In contrast, by December 2021, Rio Grande do Sul had a higher vaccination coverage, with 70.3% of the population receiving two doses and 80.9% receiving at least the first vaccine against COVID-1928. These vaccination figures underscore the progress made in immunization efforts in both states, contributing to the observed decline in COVID-19 cases and deaths during the mentioned period. At the national level, by December 2021, Brazil had reached 80% of its target population fully vaccinated30.
The national immunization strategy against COVID-19 was implemented in stages, following the prioritized order of groups defined by the PNI (National Immunization Program)31. The strategy aimed to prioritize individuals at the highest risk of developing severe forms of the disease and facing an increased risk of death. This included specific groups such as health professionals, older adults, institutionalized older people, individuals with comorbidities like hypertension and diabetes mellitus, and those with a high degree of social and economic vulnerability, such as indigenous people, quilombolas, riverside communities, and the population deprived of liberty32. This phased and targeted approach aimed to efficiently and equitably distribute the available vaccines, considering the varying degrees of vulnerability and risk across different population segments.
Mass vaccination against COVID-19 has proven to be an effective weapon in combating the pandemic. The WHO supported more countries to have access to vaccines to prevent people from becoming more seriously ill and, therefore, save more lives.
The increase in COVID-19 cases and deaths observed in both Pará and Rio Grande do Sul in December 2021, continuing into January and February 2022, aligns with the emergence of the Omicron variant. This variant, first identified in South Africa and Botswana in November, was classified as a variant of concern by the World Health Organization33. The designation was due to its numerous mutations34, making it more transmissible than the original strain of the virus. The rise in cases and deaths during this period underscores the challenges posed by the Omicron variant and its potential impact on the trajectory of the COVID-19 pandemic.
Furthermore, at the end of 2021, coinciding with the year-end holiday period, the population felt more confident due to the protection of vaccines, and there was a relaxation in the maintenance of non-pharmacological measures against COVID-19, which favored the spread of the virus in all regions of the country35. The results of this study reflect the reality of other regions of Brazil during January and February 2022. Pará totaled 93,352 cases of COVID-19, and R io Grande do Sul registered 796,948, the highest values of the entire period analyzed. This situation impacted the incidence rates, which were also the highest in the three years analyzed.
The influence of the extensive vaccination program is evident in the December 2022 trends, where mortality decreased in both Pará and Rio Grande do Sul. Despite the significant increase in cases attributed to the Omicron variant, the lethality trend remained stable in both states. The incidence decreased in Pará and remained steady in Rio Grande do Sul for 2022. However, considering the entire period, the incidence shows a consistent trend in both states, indicating the importance of ongoing monitoring of cases and morbidity across various age groups.
In both states, the spread of the virus and the high number of cases and deaths throughout the analyzed period compromised the structure of the public and private health systems due to the exponential increase in primary health services and the need for more complex services that require hospitalization and invasive mechanical ventilation27.
Despite the relevance of these epidemiological data for understanding the evolution of the disease for possible planning following statistics, some factors such as the rapid spread of the virus, the reduced number of tests carried out, especially at the beginning of the pandemic, the asymptomatic cases that often, go unnoticed by the health system, among other conditions, making it difficult to estimate the actual number of cases, generating considerable underreporting throughout the country36.
The evolution of the pandemic is influenced by several factors, where the context of vulnerability is considered a determining factor in the incidence and mortality of COVID-19. In this scenario, it is essential to mention the presence of indigenous groups in each region. According to the last Census carried out by IBGE21, Rio Grande do Sul had a population of approximately 32,989 indigenous people, and Pará had approximately 60,000 people of indigenous origin. These communities are significantly more vulnerable to epidemics because they live in remote locations, with precarious socioeconomic and health conditions, they live in remote places, with a lack of human resources in the health area, and communication limitations due to the native language. Living in collective houses and sharing utensils favors the spread of the virus. It is stated that the indigenous population affected by COVID-19 is underreported37.
The total number of cases and victims and the corresponding incidence, mortality, and lethality caused by the coronavirus during 2020, 2021, and 2022 in Pará and Rio Grande do Sul show three possible pandemic waves. The first occurred between March and November 2020, marked by high circulation of the virus38. The second, from February to July 2021, marked the emergence of several variants, and the third, from December 2021 to December 2022, was characterized by the presence of the Omicron variant. From January 2020 to May 2021, changes in the frequency of dominant lineages were recorded in Brazil, according to data from the Fiocruz Genomic Network. At the beginning of the epidemic, it was mainly driven by the B.1.1.28 and B.1.1.33 lineages, which were the most prevalent until October 202039. After this period, there was an increase in the circulation of two variants of national origin, P.1 and P.2, originating from the B.1.1.28 lineage. Regarding the notification of variants of concern and interest in public health, four variants classified as VOC and two (Zeta and Lambda) of the seven variants classified as VOI by the WHO were registered in Brazil40.
Since the beginning of the pandemic, replacements of variants have been observed, which remained throughout the period analyzed37,41.
Therefore, it is a priority to monitor the behavior of different variants to adjust control measures. According to the Pan American Health Organization40, the best way to contain the spread of the virus, regardless of the variant, is to maintain infection quarantine, patient isolation, physical distancing, use of masks, and vaccination.
This study presents some limitations in the spatial analysis arising from the methodology of ecological studies and secondary database analysis, such as delays in notifications, changes in the household that can cause distortions in the number of cases and deaths per city or municipality, and underreporting cases of the disease.
Furthermore, the results presented are partial data as the pandemic continues to be studied. The number of cases found may be higher, considering the limitations of mass testing for detecting COVID-19.
CONCLUSION
The spread of the virus and the high number of cases and deaths throughout the analyzed period compromised the structure of the health system due to the exponential increase in primary health services.
The positive impact of the vaccination program is reflected in the evolution of the pandemic and the stationary trend in incidence for both States.

