











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo

 Permalink
PermalinkINTRODUCTION
The physical, cognitive and psychosocial development of children and adolescents occurs in a harmonious and simultaneous way, through favourable conditions for their improvement. Sensory-motor stimuli (e.g. daily physical activity, sports, dance, school physical education), adequate nutrition, and good self-perception (e.g. self-efficacy, self-competency, self-image) are fundamental factors for the development of physical, cognitive, and psychosocial capacities1,2. On the other hand, unhealthy eating behaviours3, obesity4, alcoholism5and sedentary lifestyle6 are called risk behaviours, as they negatively affect the health and development of the young population7.
Monitoring, on a population scale, the risk factors for the healthy development of the population is a governmental challenge, especially in developing countries8. In these cases (such as Brazil, where this study was developed), monitoring strategies must take into account the wide social and economic inequality, considering which factors can be modified to provide conditions of equity for young people. In this way, the relevance of large-scale periodic surveys and follow-ups is noted9,10.
In the Brazilian context, life habits evaluated on a large scale have been considered as factors that can directly influence the health of the adolescent population. Among the main habits evaluated, the regular physical activities and the time spent in sedentary behaviour (e.g. screen time, reclining or sitting time, lying without sleeping) are highlighted because they are associated with several components of cardiovascular11, musculoskeletal12, mental health13, and with cognitive performance14.
In this context, Brand et al. (2020)15 show that family nucleus (specially mother) was identified as important for promoting a physically active life, and healthy eating15,16. Although parents/guardians play a key role in the child health status17,18, other factors seem to influence the health habits as well (for example, social and educational factors, gender and socioeconomic status), both positively and negatively.
Moura et al. (2018)19 showed that women and adolescents girls with low socioeconomic status had higher rates of physical inactivity and inadequate nutrition in Brazil. Other socioeconomic aspects such as the use of screens, but especially the constant use of smartphones, were also identified as a factor correlated with levels of obesity and sedentary lifestyle, being mediated by personal characteristics such as image self-perception, gender and age20. Finally, the excessive use of social medias and electronic games are also pointed out as a factor that promotes damage to biopsychosocial health (especially self-image), favouring the use of licit and illicit drugs and a sedentary lifestyle21.
Despite the vast evidence on different risk factors and their associations with behaviours that affect the development of young people, there is still a gap in the literature, the evidence base that addresses the components of health in an integral way (or planetary health)22. Evidence on isolated risk behaviours, using as outcome variables, often disregards the complexity of the phenomena and their inter-influences15,19,20. When evaluating health phenomena in a unique way, the different factors related to health impairment are overlooked, as in addition to being evaluated based on several outcome variables, it is also influenced by several individual, social, economic and family factors19.
However, one possibility to approach adolescent health variables in a complex way is to try to identify a set of conditions that can express a reality/characteristic23. Some studies16-19 have already used variable unification strategies to represent a health phenomenon. This set of variables can be a more sensitive warning indicator, revealing a reality that requires more punctual action, but above all a multidisciplinary one.
Carrying out a study considering this gap is a challenge, as it is necessary to collect several variables in a sample heterogeneous enough to represent the population and large enough to support statistical inferences. In this way, the data produced by surveys carried out by government agencies can help in this process by having standardized collection procedures and enabling a wide reach in the population. Furthermore, the process of creating methods and strategies to evaluate/interpret data on a large scale is a way of providing feedback to government research itself.
With the a of standardizing the process of evaluating the health conditions of school-aged children, the Brazilian Ministry of Health proposed the National School Health Survey (PeNSE)24, corresponding to the largest investigation carried out in the country involving community students and teenagers. PeNSE provided a rich overview of the social, parental, geographic, structural and physical factors of Brazilian students9,25, contributing with indicators that could guide local actions in the search for improvements in the conditions of these populations.
To collaborating with the development and improvement of the PeNSE research strategy, and considering the scientific gap previously presented, the present study aims to propose a combined indicator with the intention of concatenating risk behaviours into a single primary outcome, called Health Impaired Physics (IPH), and after that, identify socioeconomic indicators that can help to understand how this commitment affects the Brazilian students investigated in the PeNSE project, 2012 edition.
METHODS
Study design, participants, and data source
This is a transversal-secondary analysis study of a Brazilian public database from PeNSE. The data are available from the Brazilian Institute of Geography and Statistics (IBGE) (https://www.ibge.gov.br/). The first PeNSE edition was held in 2009, evaluating 60,973 students from the 26 capitals and the Federal District of Brazil. The second edition of PeNSE, held in 2012, expanded its scope, including issues related to work, hygiene habits, mental health, use of health services and prevalence of asthma, expanding its reach beyond the capitals of the Brazilian states and the District Federal, covering a total of 109,104 students.
For 2012 data, some cities, outside the State capitals were grouped into a stratum for each of the Federation Unities, totalizing 26 strata. The primary sampling units were schools, the secondary were classrooms, and the schoolchildren are the sample in each stratum for each city and in the Brazilian capital. The sample was randomized and equiprobability for cities and capitals. In 2012 data collection was carried out with smartphones, in which was inserted the self-administered questionnaire24.
The IBGE have a public directory, and data available by PeNSE 201224 were collected regarding 108778 female (n=51931; 48.0%) and male (n=57036; 52.0%) schoolchildren aged between 11 and 18 years (see the complete sampling methods in (www.ibge.gov.br/). Participants who self-reported the three fundamental questions for the classification of IPH were considered eligible for the analysis of the present study, disregarding the other participants for this study.
Variables
Two groups of variables were considered for the development of the present study: 1) variables related to the combined outcome that came to be called IPH; and 2) variables potentially related to IPH.
IPH components variables
To create the IPH variable we joined three categorical variables (figure 1). As the IPH is a composite categorical variable, we consider that an adolescent with IPH should be in the following three categories at the same time: negative classification of physical activity, poor perception of nutritional status and lack of effort to change weight. We highlighted these conditions are pointed out by the scientific literature as potential health risk factors to which they are exposed children and adolescents in school-age context26.
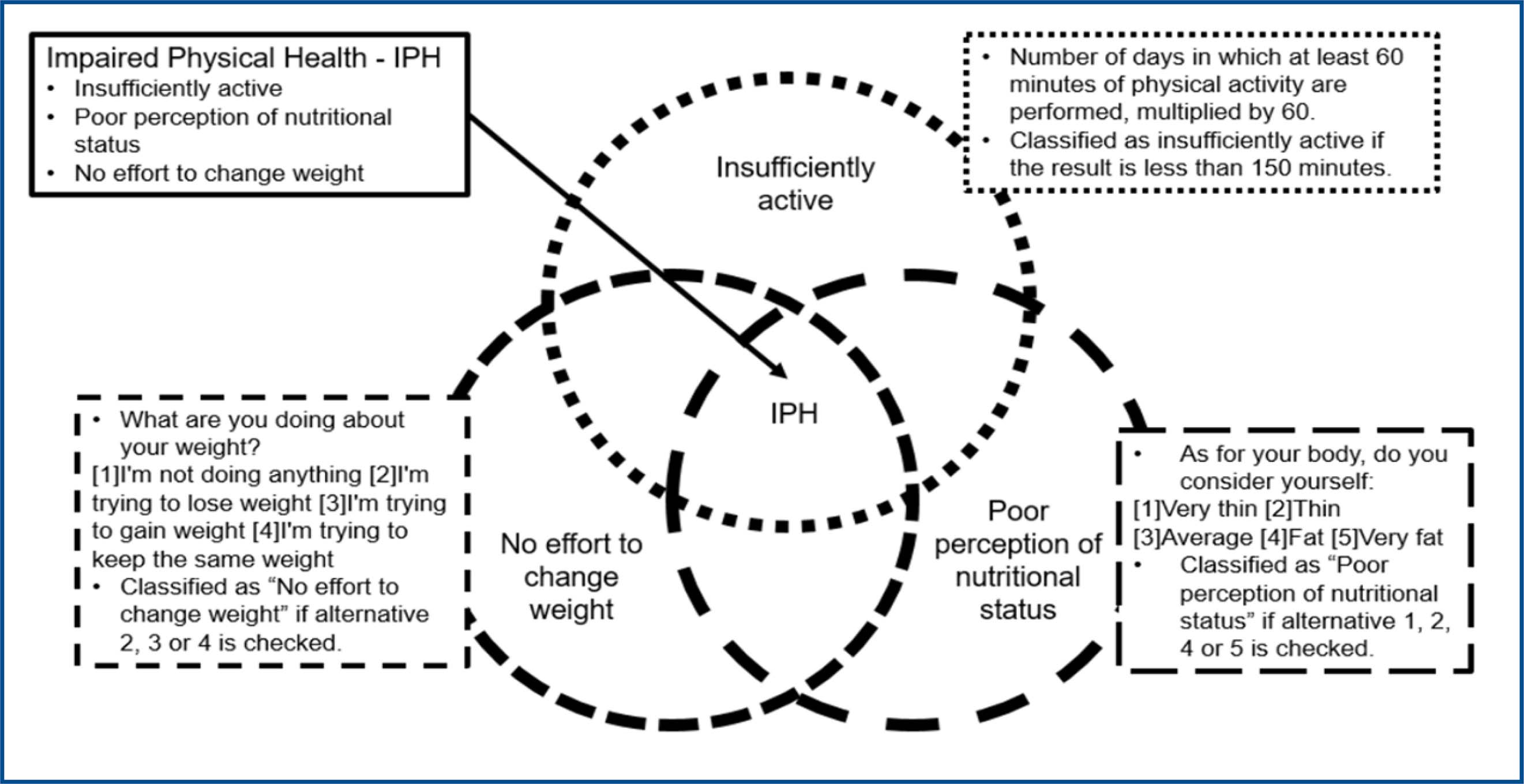
Source: Prepared by the authors.
Figure 1 : Criteria for classifying participants in Impaired Physical Health
Regarding the physical activity, it was assessed by recording the number of days in which at least 60 minutes of physical activity are performed (question B03011 - PeNSE). The classification of insufficiently active corresponded to a volume of fewer than 3 days, which corresponds to physical activity practice of fewer than 180 minutes per week. Regarding the perception of nutritional status (question B11001 – PeNSE), those who declared themselves classified as “thin”, “very thin”, “fat” and “very fat” were considered inadequate. In relation to body weight (question B11002 – PeNSE), the alternatives: “I am trying to lose weight”, “I am trying to gain weight” or “I am trying to maintain the same weight” were considered inadequate.
Variables potentially related to IPH
As variables potentially related to IFS, gender, race/ethnicity, age, residence with the father and/or mother, cell phone use, internet access and consumption of cigarettes, alcohol and other drugs were considered. The age in years of the participant was collected, we used this variable as continuous and categorical. Regarding race/ethnicity, participants could declare themselves as white, Black, Yellow, Brown or Indigenous, it is the literal language used in the PeNSE questionnaire. For this study, we adapted this to the universal read following the APA’s guidelines for talking about racial and ethnic identity with inclusivity and respect. We used Black, indigenous people, White, African American, and Native American24. The other variables presented dichotomous responses (yes or no).
Ethical aspects
As this is a study based on secondary data extracted from public databases where it is not possible to identify the study participants. The approval of an Ethics Committee in Research with Human Beings was not necessary, as directed by resolution nº 510 of April 7, 2010 of Brazilian Health Council27.
Statistical Analysis
From PeNSE 2012 microdata, a new study outcome variable (IPH) was created (see figure 1). IPH was considered a dependent variable, while gender, race/ethnicity, age, residence with the father and/or mother, phone use, internet access and smoking, alcohol and other drugs consumption were considered as independent variables in Poisson regression with robust variance. To interpret the results, the following were analysed: The Prevalence Ratio (PR), the 95% Confidence Interval, the coefficient of determination (R2) and the p-value. To analyse the IPH prevalence as a function of each variable individually, the Chi-Square test was used. Data analysis was conducted using the R statistical soft-ware (R Project). The significance level was adopted at p<0.05.
RESULTS
We observed that the South, Southeast and Northeast regions have the states with the highest frequencies of IPH. Figure 2 shows the prevalence of IPH in schoolchildren investigated by the Brazilian states, highlighting that Black and African American represent higher per-centages.
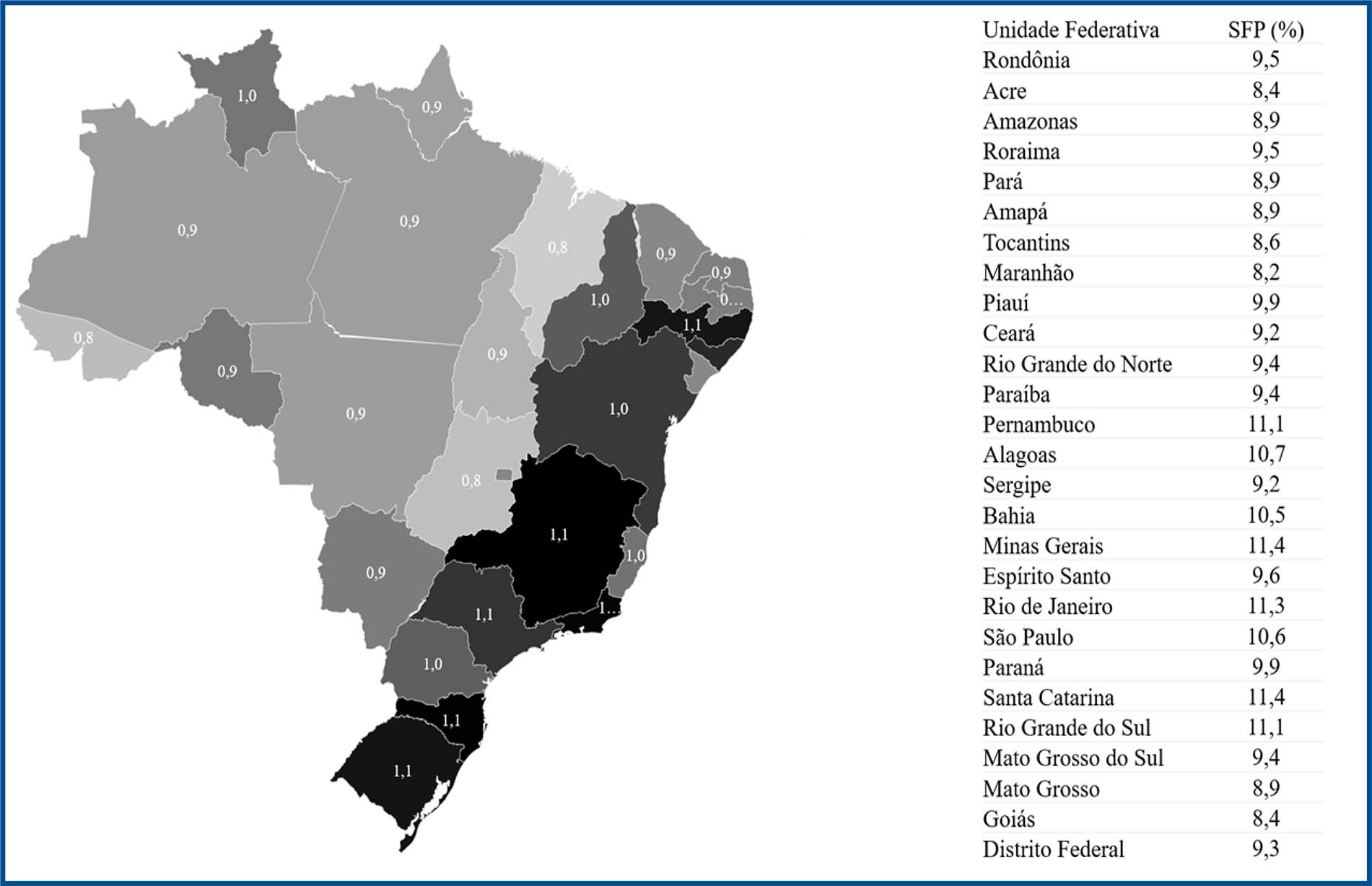
Source: Prepared by the authors
Figure 2 Geographic distribution of the prevalence of Impaired Physical Health of schoolchildren residing in Brazil in 2012
Overall, the prevalence of IPH was 9.4% of the schoolchildren, with statistical differences according to gender, ethnicity, living with the father/guardian and phone use. No significant differences were found in relation to age, living with the mother/guardian and internet access (table 1).
Table 1 Prevalence and factors associated with impaired physical health in Brazilian children and adolescents, PeNSE-2012
| Variables | N (%) | IPH (%) | p-value* | PR (CI 95%) | p-value** |
|---|---|---|---|---|---|
| 108778 (100%) | 10221 (9.4%) | ||||
| Gender | |||||
| Male | 51931 (47.6) | 3964 (38.8) | <0.001 | - | - |
| Female | 57036 (52.3) | 6257 (61.2) | 1.43 (1.38; 1.49) | <0.001 | |
| Ethnicity | |||||
| White individuals | 37632 (34.6) | 3680 (36.0) | <0.001 | - | - |
| Black | 14495 (13.3) | 1440 (14.1) | 1.02 (0.96; 1.08) | 0.612 | |
| Native American | 4817 (4.4) | 517 (5.1) | 1.01 (1.001; 1.2) | 0.048 | |
| African American | 48176 (44.2) | 4250 (41.6) | 0.90 (0.86; 0.94) | <0.001 | |
| Indigenous | 3781 (3.5) | 327 (3.2) | 0.88 (0.79; 0.99) | 0.003 | |
| Age group | |||||
| 10 - 12 | 858 (0.8) | 96 (0.8) | 0.256 | - | - |
| 13 - 15 | 72417 (66.5) | 6788 (66.5) | 0.83 (0.69; 1.01) | 0.068 | |
| 15 - 18 | 35692 (32.7) | 3337 (32.8) | 0.84 (0.69; 1.01) | 0.066 | |
| Living with father | |||||
| Yes | 69188 (63.6) | 6308 (61.8) | <0.001 | 0.92 (0.89; 0.96) | <0.001 |
| No | 39626 (36.4) | 3902 (38.2) | - | - | |
| Living with mother | |||||
| Yes | 96903 (89.0) | 9063 (88.7) | 0.362 | 0.97 (0.92; 1.03) | 0.316 |
| No | 12008 (11.0) | 1157 (11.3) | - | - | |
| Phone use | |||||
| Yes | 94116 (86.5) | 8666 (84.8) | <0.001 | 0.87 (0.83; 0.92) | <0.001 |
| No | 14740 (13.5) | 1552 (15.2) | - | - | |
| Internet access | |||||
| Yes | 69173 (63.6) | 6435 (63.0) | 0.255 | 0.97 (0.93; 1.01) | 0.211 |
| No | 39665 (36.4) | 3781 (37.0) | - | - |
IPH: Impaired Physical Health; *Chi-square; ** Poisson logistic regression; PR: Prevalence ratio; CI 95%: Confidence Interval of 95%. Source: Prepared by the authors.
Based on Poisson regression, adjusted values of the prevalence ratio were estimated, noting that girls have a PR of 1.43 (p<0.00) in relation to boys, that is, a prevalence of IPH 43% higher, regardless of the other variables included in the analysis. The ethnicity variable did not show statistical significance for Black students in relation to White students. Native American students had only 1% more than White students (p<0.05), while African American and indigenous students had 10% less prevalence in reaction to White individuals (p<0.01). Although the progression of the age group has shown a reduction in the PR values, these changes in relation to the reference age group (10 to 12 years) did not show statistical significance.
Schoolchildren living with their father have an 8% lower prevalence of having IPH (PR: 0.92; p<0.001), while living with their mother had 3% fewer IPH, however, this result was not significant in the adjusted model (RP: 0.97; p>0.05). This protective behaviour was also observed among students who use cell phones, with a 13% lower prevalence of IPH (PR: 0.87; p<0.001).
Figure 3 shows the prevalence of IPH as a function of the age and gender of school-children. We found a higher prevalence of IPH in the ages up to 11 years and a significant reduction among boys over the years (p<0.001). Girls have a higher prevalence than boys from the age of 11, without showing significant differences across ages.
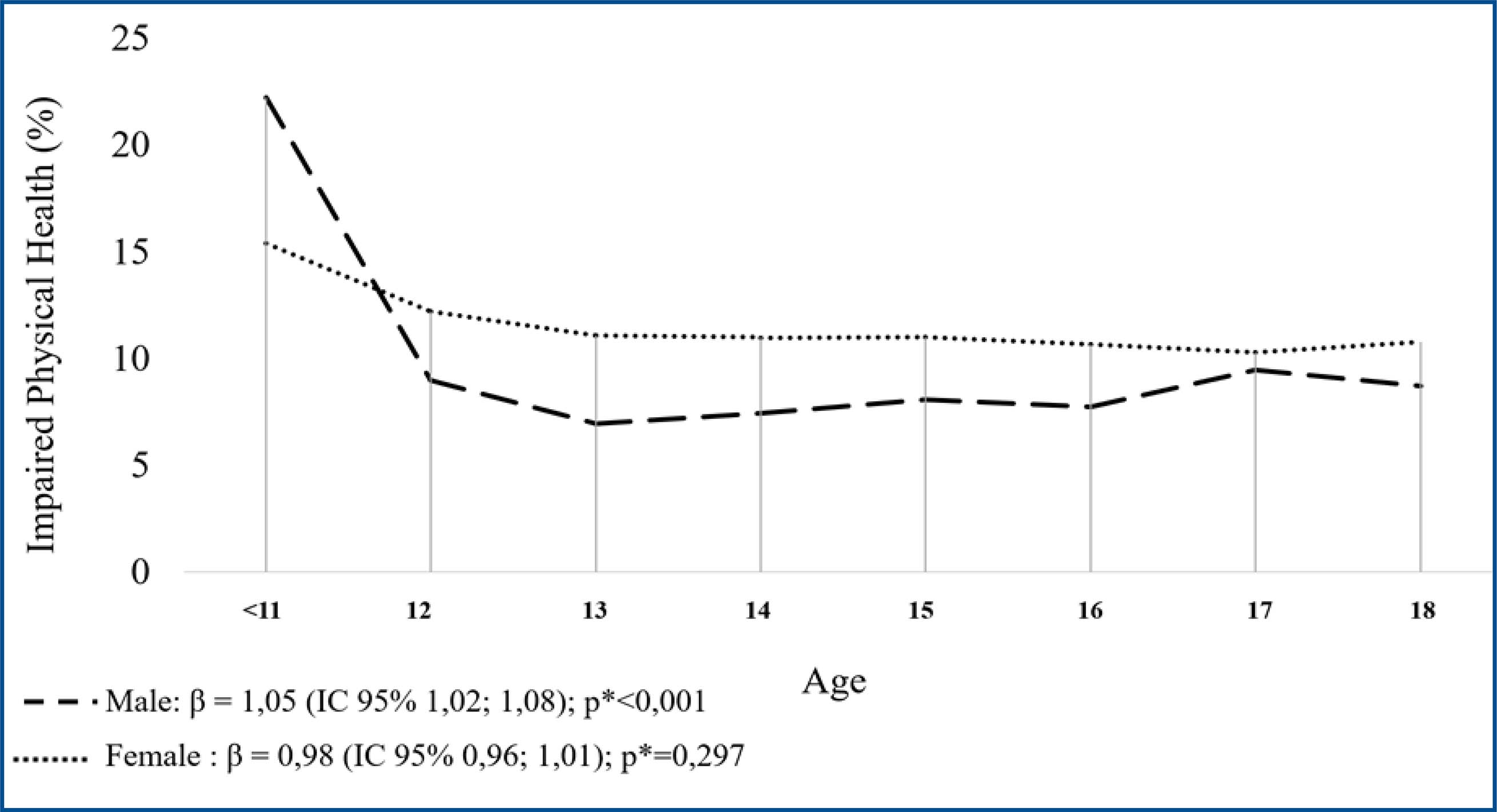
Source: Prepared by the authors.
Figure 3 Prevalence of Impaired Physical Health with age according to gender
Table 2 presents the relationship of other risky habits (smoking, alcohol and other drugs) with the prevalence of IPH. We found that only the smoking habit was associated with the prevalence of IPH (p<0.001). When analysed in an adjusted way from the variables identified as significant in table 1 (gender, living with the father, ethnicity and phone use), cigarette smoking (PR: 1.09; p<0.01) remained a significant variable and consumption of other drugs (PR: 1.08; p<0.05) was also identified as associated with the prevalence of IPH.
Table 2 Association between compromised physical health and risky habits
| Variables | N (%) | SFP (%) | RP | p -value** | PR | p -value** | |
|---|---|---|---|---|---|---|---|
| No | Yes | Adjusted | |||||
| 108778 | 98.557 | 10221 | (IC 95%) | (IC 95%) | |||
| (100%) | (90,6%) | (9,4%) | |||||
| Smoking | 22753 | 20463 | 2290 | 1,07 | <0,001 | 1,09 | <0,001 |
| (100%) | (89,9) | (10,1) | (1,03-1,12) | (1,05-1,13) | |||
| Alcohol | 72930 | 66021 | 6909 | 1,01 | 0,216 | 1,003 | 0,588 |
| (100%) | (90,5) | (9,5) | (0,99-1,02) | (0,98-1,02) | |||
| Other drugs | 8397 | 7565 | 832 | 1,06 | 0,095 | 1,08 | 0,027 |
| (100%) | (90,1) | (9,9) | (0,98-1,14) | (1,01-1,16) | |||
IPH: Impaired Physical Health; ** Poisson logistic regression; PR: Prevalence ratio; CI 95%: Confidence Interval of 95%. Source: Prepared by the authors.
DISCUSSION
In this study, we analysed physical health impairment based on the combination of three outcome variables (physical activity, nutritional status and body weight) and identified different factors associated with the prevalence of IPH in Brazilian schoolchildren. We emphasize that the conditions chosen to create the IPH variable are indicated by the scientific literature as potential health risk factors to which children and adolescents are ex-posed in the school context26. We opted for physical activity because it has a high level of relationship with physiological and psychological variables of adolescents’ health28,29. The perception of nutritional status and the variable “make an effort to change body weight” were chosen because they are easily assessed by teachers, researchers and other health professionals. Furthermore, it is recommended that, when evaluating physical health, variables of self-perception and also behaviour itself be considered17-19. For this reason, we chose to assess whether the adolescents made (or had al-ready made) any effort to change their weight, as a way of indirectly assessing behaviours.
The main evidence presented indicates that individual characteristics (gender and ethnicity), food (smoking and other drugs consumption), family (not living with parents), phone use and geographic characteristics showed a significant association with the prevalence of IPH. These results reinforce that the impairment of physical health is influenced by several factors and provide important information for managers in planning efficient public policies to promote health for this population. The evidence indicates the need for local public policies since the prevalence of IPH also varies according to the regions of the country. We observed that the South, Southeast and Northeast regions have the highest frequencies of IPH, which can be explained, in part, by the greater physical inactivity presented by the population of these regions30. Physical inactivity may also explain the higher prevalence of IPH in female adolescents when compared to males. Previous studies have shown that, in the Brazilian reality, female adolescents practice fewer physical activities29,30, negatively influencing the health of this population. Although Physical Education classes at school have promoted greater participation of female adolescents, the social and cultural challenges still faced by girls and women regarding the practice of physical activity indicate the need for public policies aimed at this population31.
Ethnicity was also identified as an associated factor of IPH, being more prevalent in White individuals, Black and Native American adolescents. Some factors may act as mediators and explain these findings. Previous studies have shown that White adolescents have a higher alcohol consumption32 and a higher prevalence of eating disorders33, negatively impacting their health. On the other hand, physical inactivity, which also compromises health, is more prevalent in Brazilians who declare themselves to be Black or African American34. Economic aspects may explain, in part, these differences since the White individuals historically had more social and economic privileges, while the Black population faces different types of segregation. Consequently, finds more barriers to participating in physical activities in recreational and fewer health-related opportunities. Thus, gender, class and ethnicity are factors that intersect with each other and should be taken into account in the elaboration of public policies for the health of children and adolescents.
When investigating family factors, we found that living with the father reduces the prevalence of IPH, but living with the mother does not appear to be a significant factor. The relationship between family and adolescents is complex and diverse, with different facets. For example, Peres et al. (2008)35 showed that rates of several IPH were lower among adolescents living with both parents and higher among those living with neither, indicating family members as a supportive factor that favours a healthy life. On the other hand, Costa et al. (2007)36 showed that among the reasons for adolescents to start using alcohol, curiosity, being with parents and friends stand out, with the family being an enabler of alcohol consumption.
In this study, we advance knowledge and present a new element for research by showing that fathers and mothers exert different influences on their children’s health. In the present investigation, we did not investigate parents’ engagement in physical activities performed by schoolchildren. But, in the Brazilian context, we know that the willingness of children and adolescents to start or remain physically active seems to be associated with living with people who perform this type of routine37,38. Parents exert a great in-fluence and often encourage their children to practice activities39, acting in a protective way for IPH when analysed in isolation and remaining significant when considered in the adjusted model.
The results of our study also show that cell phone use is a factor that decreases the prevalence of IPH. We can explain this finding from an indirect relationship with the socioeconomic level of these students since the phone pose can be interpreted - hypothetically - as an indirect sign of better access to infrastructure, food and care opportunities. Furthermore, Georgeson et al. (2020)40recently showed that technological resources, such as smartphones, have been used to carry out interventions aimed at changing behaviour in favour of the health of children and adolescents. In addition, Aschbrenner et al. (2019)41 showed that the phone can be used by public health agents as a technology to promote physical activity and, consequently, to protect IPH, indicating its potential in the development of strategies for health promotion.
When investigating health risk factors, we found a high prevalence of alcohol use (67%) among Brazilian schoolchildren. Studies carried out in the early 2000s showed that approximately 48% of Brazilian adolescents consumed alcoholic beverages42, indicating a possible increase in this prevalence over the last few years. Adolescence is particularly important in this debate because it is indicated as the moment of first contact with alcohol and other drugs, being stimulated mainly by social interaction43. The concern with the use of alcohol in adolescence and its continuity in adulthood is due to the various dam-ages generated to the body and, consequently, to the health of its users.
In addition to the direct consequences of intoxication, there are long-term consequences that can interfere with the adolescent’s life, such as learning, employment prospects, risky behaviour in traffic, situations of violence, such as involvement in fights, sexual and domestic violence, and among others44. Therefore, although there was no evidence of a significant association between alcohol consumption and IPH, the high per-centage of participants who have already consumed alcohol deserves to be highlighted and draws the attention of health policymakers in the country.
In the present study, smoking was significantly associated with IPH, with a prevalence of IPH 7% higher in participants who maintained this behaviour. When analysed in combination with the consumption of alcohol and other drugs, its adjusted prevalence was 9% higher, exposing an interaction with the consumption of other drugs. Smoking consumption is directly related to a variety of health problems, especially respiratory problems45 and the development of lung cancer46, compromising even more when smoking begins in adolescence45. Seo & Huang (2012)47 highlighted in their study that smoking interferes with the willingness to perform physical activities, especially due to the perception of compromising physical performance, in addition to the effective respiratory compromise. These factors together become aggravating factors for the health of adolescents and reinforce their importance in the development of public health strategies for adolescents.
Analysing the consumption of other drugs alone, the prevalence ratio did not show a significant association, however, when analysed together with smoking and alcohol, it started to show statistical significance, with a prevalence of 8% higher in participants classified with IPH. The consumption of other drugs represents an alert that must be taken into account by health and education managers, especially when the results concern elementary school students, a time of transition to adolescence with the prospect of greater family independence and social interaction. Schoolchildren who smoke, consumption alcohol or other types of drugs tend to perceive a compromise in their physical capacity or body image, which influences their commitment to start or remain physically active47.
Finally, our study demonstrated that the IPH variable can be easily collected and evaluated in future research. In addition to surveys, teachers and health professionals can use a simple questionnaire assessment to obtain a profile of adolescent physical health, which we have shown to be associated with various sociodemographic variables.
Despite the important results brought by our study and its practical applicability for health managers, it is important to recognize its limitations. Firstly, data collection was performed using a public database made available by the national government. Although the national mapping was carried out in a standardized way, we do not have access to nor provide parameters of reliability for data collection. In addition, the variables investigated in this study corresponded to those collected by PeNSE, indicating the possibility of investigating the influence of other variables on the health parameters of Brazilian schoolchildren. Finally, our results are a first indication of a variable that can be used to monitor the physical health status of adolescents, however, the results obtained in this work are suggested to compare with previous research to validate their applicability for different situations.
CONCLUSION
The main evidence presented indicates that individual characteristics (gender and ethnicity), diet (smoking and consumption of other drugs), family (not living with parents), telephone use and geographic characteristics were significantly associated with the prevalence of impaired physical health. These results reinforce that the impairment of physical health is influenced by several factors and provide important information for managers in planning efficient public policies to promote health for this population.

