CASE REPORT
Sigmoid volvulus as a complication of imperforate anus: a case report
Caio Felipe Araujo Matalani, Conception and design of the research, obtaining clinical data, literature review and critical evaluation of the reporta
 http://orcid.org/0000-0001-8769-9149
http://orcid.org/0000-0001-8769-9149
Giovanna Layse Uyeda, Conception and design of the research, obtaining clinical data, literature review and critical evaluation of the reporta
http://orcid.org/0000-0003-2291-7381
Danilo Maciel de Deus e Melo, Conception and design of the research, obtaining clinical data, literature review and critical evaluation of the reporta
http://orcid.org/0009-0000-3395-292X
Isabella Meneghetti Inacio Silva, Conception and design of the research, obtaining clinical data, literature review and critical evaluation of the reporta
http://orcid.org/0009-0003-4636-7422
Ana Cristina Aoun Tannuri, Supervision and guidancea
http://orcid.org/0000-0002-5481-032X
aInstituto da Criança do Hospital das Clínicas da Faculdade de Medicina da USP, HCFMUSP, São Paulo,05403-000; drcaiomatalani@gmail.com; dragiovannauyeda@gmail.com; danilomdmelo@gmail.com; isabellamisilva@gmail.com; cristannuri@hotmail.comBrazil
Abstract
Introduction
we report a case of a 6-year-old boy with chronic constipation due to an imperforate anus and poor adherence to outpatient treatment, who developed a severe sigmoid volvulus requiring Hartmann’s procedure.
Objective
the main objective of this report is to contribute to knowledge about a rare condition in children, with few descriptions in the literature.
Methods
the study is characterized as a case report, based on the clinical evaluation, medical records, and surgical descriptions of a 6-year-old male patient. Associated with the report, medical databases (PUBMED, LILACS) were searched for reviews and case reports about sigmoid volvulus in children and its relationship with anorectal anomaly, including aspects of diagnosis and treatment.
Results
patient, male, 6-years-old, with a history of anoplasty due to an imperforate anus, developed over the years with chronic constipation and multiple fecal impactions removal. After the last procedure, he presented prostration and abdominal pain, with an image diagnosis of sigmoid volvulus. The patient underwent laparotomy, with visualization of extensive necrosis and the option of performing segment resection and colostomy.
Conclusion
sigmoid volvulus is a rare condition in children and needs to be quickly identified so that earlier interventions can prevent advanced outcomes.
Key words: intestinal volvulus; imperforate anus; anorectal anomaly; bowel dysfunction; pediatrics; case report
Authors summary
Why was this study done?
Case report of an association between sigmoid volvulus and anorectal anomaly, a condition rarely described in the literature.
What did the researchers do and find?
The researchers studied patient records, such as surgical descriptions and images. Furthermore, we searched the literature for case reports and reviews about sigmoid volvulus in children and its relationship with anorectal anomaly.
What do these findings mean?
The finding shows that the association between anorectal anomaly and sigmoid volvulus is rare, with few reports in the literature. This case is an important tool for increasing knowledge on the topic.
Key words: intestinal volvulus; imperforate anus; anorectal anomaly; bowel dysfunction; pediatrics; case report
Highlights
This study describes a case of sigmoid volvulus in a child with an imperforate anus, an extremely uncommon association reported in very few cases worldwide. Not only does the report emphasize the rarity of this overlap of conditions among fewer than 100 occurrences of pediatric sigmoid volvulus, only three involved anorectal malformations but it also underscores the importance of early diagnosis and appropriate surgical treatment to prevent serious complications such as intestinal necrosis. Thus, this case serves as a reference for therapeutic management in similar situations and highlights the need for special attention to children with anorectal malformations and chronic constipation.
Key words: intestinal volvulus; imperforate anus; anorectal anomaly; bowel dysfunction; pediatrics; case report
Resumo
Introdução
relatamos o caso de um menino de 6 anos com constipação crônica em consequência de ânus imperfurado e má adesão ao tratamento ambulatorial, que desenvolveu volvo grave de sigmoide com necessidade de procedimento de Hartmann.
Objetivo
o principal objetivo deste relato é contribuir para o conhecimento sobre uma condição rara em crianças, com poucas descrições na literatura.
Método
o estudo caracteriza-se como um relato de caso, baseado na avaliação clínica, prontuários e descrições cirúrgicas de um paciente do sexo masculino, de 6 anos de idade. Associadas ao relato, foram pesquisadas bases de dados médicas (PUBMED, LILACS) em busca de revisões e relatos de casos sobre volvo de sigmóide em crianças e sua relação com anomalia anorretal, incluindo aspectos de diagnóstico e tratamento.
Resultado
paciente, sexo masculino, 6 anos de idade, com história de anoplastia por ânus imperfurado, evoluiu ao longo dos anos, com constipação crônica e múltiplas desimpactações fecais. Após o último procedimento, apresentou prostração e dor abdominal, com diagnóstico após imagem de volvo de sigmoide. Paciente foi submetido a laparotomia, com visualização de extensa necrose e opção de realização de ressecção do segmento e colostomia.
Conclusão
o volvo de sigmoide é uma condição rara em crianças e precisa ser rapidamente identificado, para que intervenções mais precoces evitem piores desfechos.
Palavras-Chave: volvo intestinal; ânus imperfurado; anomalia anorretal; disfunções intestinais; pediatria, relato de caso
INTRODUCTION
Sigmoid volvulus (SV) is a rare cause of intestinal obstruction in children1. Consequently, most published studies on this topic are case reports2-6. These reports highlight an association of SV with chronic constipation (10%) and Hirschsprung’s disease (HD) (10%)7.
Anorectal anomalies, such as imperforate anus, represent a condition that can trigger constipation and has also been associated with SV8, although they are less commonly reported in the literature.
We report the case of a 6-year-old boy with chronic constipation due to an imperforate anus and poor adherence to outpatient treatment, who developed a severe sigmoid volvulus requiring Hartmann’s procedure. The patient showed significant clinical improvement following surgery.
The main objective of this report is to contribute to knowledge about a rare condition in children.
METHODS
Study design
The study is characterized as a case report, based on the clinical evaluation, medical records, and surgical descriptions of a 6-year-old male patient. Associated with the report, medical databases (PUBMED, LILACS) were searched for reviews and case reports about sigmoid volvulus in children and its relationship with anorectal anomaly, including aspects of diagnosis and treatment.
Study location and period
Survey made between December 10th and December 20th, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo.
Study population and eligibility criteria
Children diagnosed with sigmoid volvulus, and Children with anorectal anomaly.
Data collection
Clinical evaluation, medical records, and surgical descriptions of a 6-year-old male patient and reviews or case reports in the literature.
Data analysis
Since this is a case report, no objective data analysis was performed; instead, a descriptive analysis was conducted following the search for similar reports in the previously mentioned databases.
Ethical and legal aspects of the research
This article does not contain studies with humans or animals carried out by none of the authors.
RESULTS
Case report
A 6-year-old patient, who had undergone cutback anoplasty 5 years prior due to an imperforate anus, was under regular outpatient follow-up with no other comorbidities. During follow-up, the patient presented chronic constipation and required ambulatory fecal impaction removal in the surgical center 17 times.
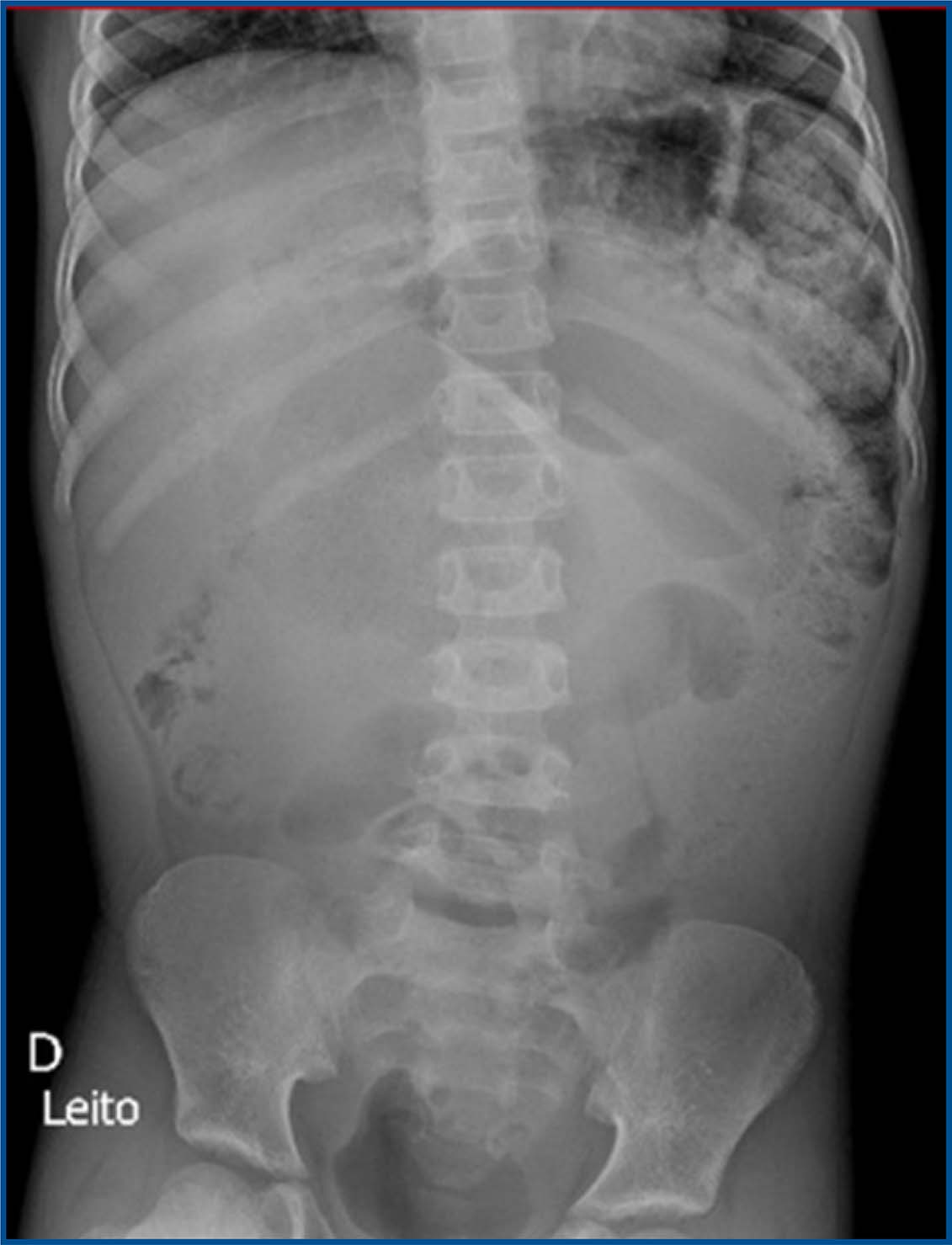
During the most recent outpatient visit, a significant fecal impaction was again identified, requiring surgical removal. Following the procedure, the patient remained hemodynamically stable, but experienced prostration, abdominal pain, poor oral intake tolerance, and diffuse abdominal tenderness on palpation, without signs of peritonitis. An abdominal X-ray was performed (figure 1), and the patient was started on a regimen of antibiotics, cessation of oral intake, basal maintenance fluids, and optimized analgesia.
Although hemodynamically stable, the patient continued to report intermittent abdominal pain. On physical examination, the abdomen was tense, with no rebound tenderness. Given these findings, a follow-up upright abdominal X-ray was ordered (figures 2 and 3), as the initial supine bedside X-ray showed no significant abnormalities.
The follow-up imaging revealed the “coffee bean” sign, leading to a sigmoid volvulus diagnosis. Surgical intervention was deemed necessary, and an exploratory laparotomy was performed. This confirmed the presence of a volvulus with three complete twists, accompanied by necrosis of the entire sigmoid colon, though without perforation (figure 4). The volvulus was successfully untwisted, and the necrotic sigmoid segment was resected. The distal rectal stump was amputated, and a Brooke colostomy was created. The procedure was completed without complications.
Following surgery, the patient required brief vasoactive support with norepinephrine and continued intravenous antibiotics. The clinical course was favorable, with the patient progressing to clinical stabilization and improvement. Upon discharge, the patient was in good general condition, afebrile, tolerating oral intake well, with a soft, non-tender abdomen on palpation and normal bowel sounds.
DISCUSSION
Sigmoid volvulus is a rare but significant condition that can lead to acute intestinal obstruction. While commonly seen in adults, particularly those with risk factors such as chronic constipation or advanced age, its occurrence in children is infrequent. Since 1940, fewer than 100 cases of sigmoid volvulus in pediatric patients have been reported in the literature, highlighting its unusual nature in this population. Among these, only three cases have been described in association with anorectal malformations, further underscoring the complexity and rarity of this clinical presentation9.
The clinical presentation typically includes abdominal pain, distension, and constipation, often associated with colonic transit disturbances, as seen in our case. Radiological imaging, such as the classic “coffee bean” sign observed in abdominal X-rays, is essential for early diagnosis, as demonstrated in this case9,10 This finding aligns with the literature, which suggests that early identification of the sign can reduce the risk of severe complications, such as intestinal perforation9,11.
The therapeutic approach to sigmoid volvulus depends on the extent of necrosis and the patient’s clinical status. Although endoscopic detorsion is considered the initial treatment option for uncomplicated cases, surgical intervention was indicated in this patient due to the presence of extensive sigmoid colon necrosis11,12. Exploratory laparotomy was performed, successfully removing the affected segment and creating a Brooke colostomy13, which is the standard approach for cases with extensive necrosis. This decision was made based on the fact that a definitive colostomy provides better outcomes in cases of extensive necrosis, particularly when the viability of the colon cannot be safely restored14.
Postoperatively, the patient required brief vasopressor support for hemodynamic stabilization, which was effective and short-lived, as the overall clinical course was satisfactorily managed with antibiotics and appropriate post-surgical care. Although this case had a favorable outcome, it is important to note that complications such as sepsis or multi-organ failure may occur, especially in older patients or those with significant comorbidities9,11.
The main clinical lesson from this case is the importance of rapid and accurate evaluation in patients presenting with signs and symptoms of acute intestinal obstruction, as early diagnosis can improve prognosis and reduce complications. Additionally, careful selection of the therapeutic approach, based on the severity of necrosis and the patient’s clinical condition, is crucial for treatment success.
CONCLUSION
Sigmoid volvulus should be considered in the differential diagnosis of pediatric patients presenting with acute abdominal obstruction, especially those with underlying conditions such as anorectal malformations. Early diagnosis and timely surgical intervention are crucial to prevent morbidity and mortality. This case adds to the limited literature on sigmoid volvulus in children and highlights the challenges in managing such rare and complex cases.
Acknowledgments
We would like to express our gratitude, first and foremost, to the patient and their family for granting permission to report this case and for their cooperation with the team. Additionally, thanks to the Institute for Children and Adolescents for its technical support, infrastructure, and exceptional care provided to its patients.
REFERENCES
1. Ciardini, A Vizzoni, L Dinelli, PVolvulus of the sigmoid colon in childhood. Osp Ital Pediatr. 1977; 12:663-675.
[ Links ]
2. Allen RP, Nordstrom JE: Volvulus of the sigmoid colon in children. Am J Roentgenol 91:690-693, 1964.
[ Links ]
3. Valla JS, Louis D, Berard J, Jaubert M, de Beaujeu MJ. Volvulus du sigmoïde chez l'enfant. A propos de 6 observations [Sigmoid volvulus in children. About 6 cases]. Chir Pediatr. 1982 Mar-Apr;23(2):93-6. French. PMID: 7074724.
[ Links ]
4. McCalla TH, Arensman RM, Falterman KW. Sigmoid volvulus in children. Am Surg. 1985 Sep;51(9):514-9. PMID: 4037548.
[ Links ]
5. Venugopal KS, Wilcox DT, Bruce J. Hirschsprung's disease presenting as sigmoid volvulus in a newborn. Eur J Pediatr Surg. 1997 Jun;7(3):172-3. doi: 10.1055/s-2008-1071085. PMID: 9241508.
[ Links ]
6. Zain M, Abouheba M. Sigmoid volvulus; a rare complicated presentation of Hirschsprung's disease: A case report. Int J Surg Case Rep. 2021 Dec;89:106608. doi: 10.1016/j.ijscr.2021.106608. Epub 2021 Nov 18. PMID: 34808446; PMCID: PMC8607194.
[ Links ]
7. Hencke J, Loff S. Recurrent Sigmoid Volvulus in Children-Our Experience and Systematic Review of the Current Literature. Children (Basel). 2023 Aug 24;10(9):1441. doi: 10.3390/children10091441. PMID: 37761402; PMCID: PMC10528811.
[ Links ]
8. Janik JS, Humphrey R, Nagaraj HS. Sigmoid volvulus in a neonate with imperforate anus. J Pediatr Surg. 1983 Oct;18(5):636-8. doi: 10.1016/s0022-3468(83)80382-0. PMID: 6644513.
[ Links ]
9. Damkjaer MB, Farooqui W, Ifaoui I, Penninga L. Sigmoid volvulus in children. BMJ Case Rep. 2021 May 12;14(5):e241869. doi: 10.1136/bcr-2021-241869. PMID: 33980558; PMCID: PMC8117995.
[ Links ]
10. Puneet, Khanna R, Gangopadhyay AN, Shahoo SP, Khanna AK. Sigmoid volvulus in childhood: report of six cases. Pediatr Surg Int. 2000;16 (1-2):132-3. doi: 10.1007/s003830070001. PMID: 10663863.
[ Links ]
11. Parolini, Filippo et al. Sigmoid volvulus in children. Surgery, Volume 161, Issue 2, 562 - 563. DOI: doi:10.1016/j.surg.2016.01.020.
[ Links ]
12. Smith SD, Golladay ES, Wagner C, Seibert JJ. Sigmoid volvulus in childhood. South Med J. 1990 Jul;83(7):778-81. doi: 10.1097/00007611-199007000-00015. PMID: 2196690.
[ Links ]
13. BROOKE BN. The management of an ileostomy, including its complications. Lancet. 1952 Jul 19;2 (6725):102-4. doi: 10.1016/s0140-6736(52)92149-1. PMID: 14939845.
[ Links ]
14. Baiu I, Shelton A. Sigmoid Volvulus. JAMA. 2019 Jun 25;321(24):2478. doi: 10.1001/jama.2019.2349. PMID: 31237646.
[ Links ]
© The authors (2025).












 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo

 Permalink
Permalink