











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo

 Permalink
Permalink
INTRODUCTION
Other nomenclatures/synonymous terminology for accelerated idioventricular rhythm (AIVR): Idioventricular rhythm, “slow ventricular tachycardia (VT)”, “Reperfusion arrhythmia”, nonparoxysmal VT, accelerated isorhythmic ventricular rhythm, and the curious nomenclature “benevolent VT”1.
Definition: AIVR is a typically regular ventricular rhythm, with a heart rate between 50 to 110 (-120) beats per minute (bpm) absence of P waves or sinus P waves with atrioventricular dissociation, and a wide QRS interval. When the sinoatrial node is blocked or suppressed, latent pacemakers become active to conduct rhythm secondary to enhanced activity and generate escape beats that can be atrial, junctional or ventricular. When ventricular rhythm takes over, it is essentially called idioventricular rhythm2.
AIVR is currently defined as an enhanced ectopic ventricular rhythm with at least three consecutive ventricular beats, which is faster than normal intrinsic ventricular escape rhythm (≤40 bpm), but slower than VT (at least 100-120 bpm).
History: “Idioventricular rhythm” was first described by Sir Thomas Lewis in 1911 in his textbook “Mechanism of the Heart Beat” as the slow intrinsic ventricular rhythm not evident from the ECG during ordinary circumstances3. The topic was later expanded in his book entitled “The Mechanism and Graphic Registration of the Heart Beat. Whit Especial Reference to its Clinical Pathology published in 1920”. Lewis’s book is considered the first book on the electrocardiogram. The book is about the mechanism of the heartbeat and its clinical pathology. It includes (experimental and clinical) examples of graphic records and analysis, including AIVR, to help readers understand the subject.
Sir Thomas Lewis (1881-1945) was a British pioneer in cardiology.
1963: Phibbs, analyzed the diverse semantics and nomenclature such as interference and dissociations terms1.
1966: Marriot and Menendez introduced the current term for AIVR4 1969: Agustín Castellanos Jr. used the term “slow VT” to describe AIVR during an acute MI5.
1974. Rothfeld and Zucker described the polymorphic form of AIVR, which they called “Multiform accelerated idioventricular rhythm!!6.
AIVR and VT are both heart rhythms that originate in the ventricles, but they differ in heart rate and clinical implications:
Heart rate: AIVR has a heart rate between 50 and 110 (-120) beats per minute (bpm), while VT is faster than 100 bpm, normally >120 bpm.
Clinical implications: AIVR is usually a benign rhythm that doesn’t require direct antiarrhythmic therapy, while VT can be life-threatening.
ECG appearance: Both rhythms have wide QRS complexes on the ECG, but AIVR has a slower rate than VT.
Other differences between AIVR and VT include:
Hemodynamic stability: AIVR is mainly a hemodynamically stable rhythm that often occurs in acute myocardial infarction.
Complications: Rarely, AIVR can degenerate into VT or ventricular fibrillation (VF), resulting in hemodynamic instability and risk of sudden cardiac death.
AIVR is sometimes called a “slow ventricular tachycardia” because it has similar characteristics to VT, but a slower ventricular rate.
Importantly, there is potential rate overlap between AIVR and some slow VT. AIVR should not be diagnosed solely based on ventricular rate; context is important. Other characteristics of AIVR are helpful for its correct diagnosis. Fusion and capture beats are much more frequent in AIVR than in VT, because the heart rate of AIVR is often close to that of the prevailing sinus rhythm6,7. AIVR typically lacks the abrupt onset typical for VT.
AIVR is generally a transient rhythm, rarely causing hemodynamic instability and rarely requiring treatment. However, misdiagnosis of AIVR as slow ventricular tachycardia or complete heart block can lead to inappropriate therapies with potential complications. AIVR is often a clue to certain underlying conditions, like myocardial ischemia-reperfusion, digoxin toxicity, and cardiomyopathies8-11.
Pathophysiology
In most cases, the mechanism of AIVR appears to be related to enhanced automaticity in the His-Purkinje fibers and/or myocardium2, sometimes accompanied with vagal excess and decreased sympathetic activity12. Ischemia, reperfusion, hypoxia, drugs, and electrolyte abnormalities can all accelerate the phase 4 action potential depolarization rates in the His-Purkinje fibers and myocardium, leading to faster spontaneous cell depolarization (enhanced automaticity)8. When the enhanced automaticity in the His-Purkinje fibers or myocardium surpasses that of the sinus node, AIVR manifests as the dominant rhythm of the heart. Sinus bradycardia may facilitate the appearance of AIVR.
Under certain conditions such as acute ischemia and digoxin toxicity, triggered activity has been suggested as the mechanism for AIVR2.
Most AIVRs originate from a single focus. Occasionally, in patients with acute myocardial ischemia and myocarditis, AIVR can originate from multiple foci13-15.
Usually, AIVR is hemodynamically well tolerated due to its relatively slow ventricular rate. It is self-limited and resolves as sinus rate surpasses the rate of AIVR. Rarely, AIVR can degenerate into life-threatening ventricular arrhythmias. In patients with severe myocardial dysfunction, AIVR may lead to hemodynamic instability due to the loss of AV synchrony or the ventricular rate. Frequent AIVR may impair left ventricular function similar to the scenario with high rate of ventricular premature beats; left ventricular ejection fraction was negatively correlated with AIVR burden on Holter monitoring16.
Etiologies
AIVR can occur in apparently healthy individuals17-19. The most common cause of AIVR is myocardial reperfusion in acute myocardial infarction. The list of other etiologies is long, and includes the following:
Buerger disease20, or thromboangiitis obliterans (TAO), is a rare disease that causes inflammation and blockage of small and medium-sized blood vessels in the arms, legs, fingers, and toes. The exact cause of Buerger disease is unknown, but tobacco use is a central factor in its initiation and progression.
Congenital heart disease21 (CHD), including tetralogy of Fallot, ventricular septal defect, and Ebstein’s anomaly.
Dilated cardiomyopathy10 (DCM). Based on Holter findings, AIVR appeared to be a benign finding in patients with idiopathic DCM.
Myocarditis13. There are only a few case reports dealing with AIVR in myocarditis, and therefore, it is difficult to assess the clinical significance of this combination.
Drugs: digoxin toxicity9,22, cocaine toxicity23, and various anesthesia agents24-26.
Electrolyte abnormality such as hypo- and hyperkalemia (often associated with impaired renal function).
Post resuscitation27. In one study, post-resuscitation AIVR was associated with lower survival in successfully resuscitated out-of-hospital cardiac arrest victims.
AIVR in the acute myocardial infarction scenario.
Clinically, AIVR has been best studied in patients with acute ST-elevation myocardial infarction (STEMI)28,29. In the thrombolysis era, AIVR was noted to be a marker of reperfusion15,30. However, not all patients with reopened coronary artery have AIVR. In patients with acute myocardial infarction treated with primary percutaneous coronary intervention, the reported incidence of AIVR varied significantly, ranging from 15-42%, depending on methods of monitoring30.
Studies in patients with STEMI treated with primary percutaneous coronary intervention support that AIVR is a marker of reopening of an occluded coronary artery but is not necessarily a marker for complete reperfusion. In fact, AIVR seems to be associated with more extensive myocardial damage and delayed microvascular reperfusion30, although the mortality rates were similar in patients with and without AIVR. In primary percutaneous intervention patients, AIVR following reperfusion was associated with marked reduction in both systolic and diastolic blood pressure, irrespective of the infarct-related artery31.
In association with bundle branch block32. A case report described AIVR unmasking of the Brugada electrocardiographic pattern in a patient with right bundle branch block.
Epidemiology
Hingorani et al analyzed drug-free ambulatory ECG recordings from 1273 healthy volunteers (who had normal screening ECGs) from 22 phase 1 studies that were analyzed in a core ECG laboratory. AIVR was observed in 0.3% of these apparently healthy volunteers, while other types of arrhythmias were observed in a higher percentage33.
No racial preponderance exists, and men and women are equally affected.
No age predilection exists.
Prognosis
AIVR is a mostly self-limiting rhythm and typically has a benign prognosis, when AIVR rather than a slow VT is the true underlying entity2. The prognosis of patients with AIVR largely depends on their underlying conditions.
Morbidity/mortality
In general, AIVR does not significantly affect morbidity or mortality, which reflects that of the underlying condition causing the AIVR. In a retrospective observation study, AIVR was found to be associated with a lower 7-day survival rate in post-resuscitation patients compared to patients without AIVR27.
Patient history
History is helpful for identifying the underlying etiology for accelerated idioventricular rhythm (AIVR). AIVR per se may be an accidental finding in the 12-lead ECG, or more often, on Holter monitoring. The presence of the following conditions supports a potential diagnosis of AIVR:
Most patients with AIVR have chest pain or shortness of breath, symptoms related to myocardial ischemia. The arrhythmia typically appears at the time of myocardial reperfusion with drugs or coronary artery interventions8.
Some patients with AIVR have chest discomfort, shortness of breath, peripheral edema, cyanosis, clubbing, symptoms related to cardiomyopathy, myocarditis, and congenital heart diseases.
Occasionally, patients with AIVR have a history of using digoxin, some anesthetic agents, or cocaine.
Rarely, AIVR can occur in people without apparent heart disease and no identifiable triggers.
Physical Examination
There are no specific physical findings for accelerated idioventricular rhythm (AIVR). The following physical signs may be present:
Slow (< 55 bpm) or fast (>100 bpm) pulse rate.
Variable heart sound intensity and cannon A waves related to atrioventricular dissociation.
Some irregularity of heart rate/pulse rate due to competing sinus rhythm and AIVR.
Rarely, hypotension related to either AV asynchrony or relatively rapid ventricular heart rate during AIVR.
Diagnostic Considerations
Accelerated idioventricular rhythm (AIVR) is diagnosed based on its characteristic electrocardiographic findings. Its main differential diagnosis includes.
Slow ventricular tachycardia, complete heart block,
Junctional rhythm with aberrancy, supraventricular tachycardia with aberrancy, and
Slow antidromic atrioventricular reentry tachycardia.
AIVR is a wide QRS ventricular rhythm with rate of 50-110 (120) bpm, often with variability during the episodes. However, AIVR should not be diagnosed solely by its ventricular rate because of the rate overlap between AIVR and some slow ventricular tachycardias. See the image below.
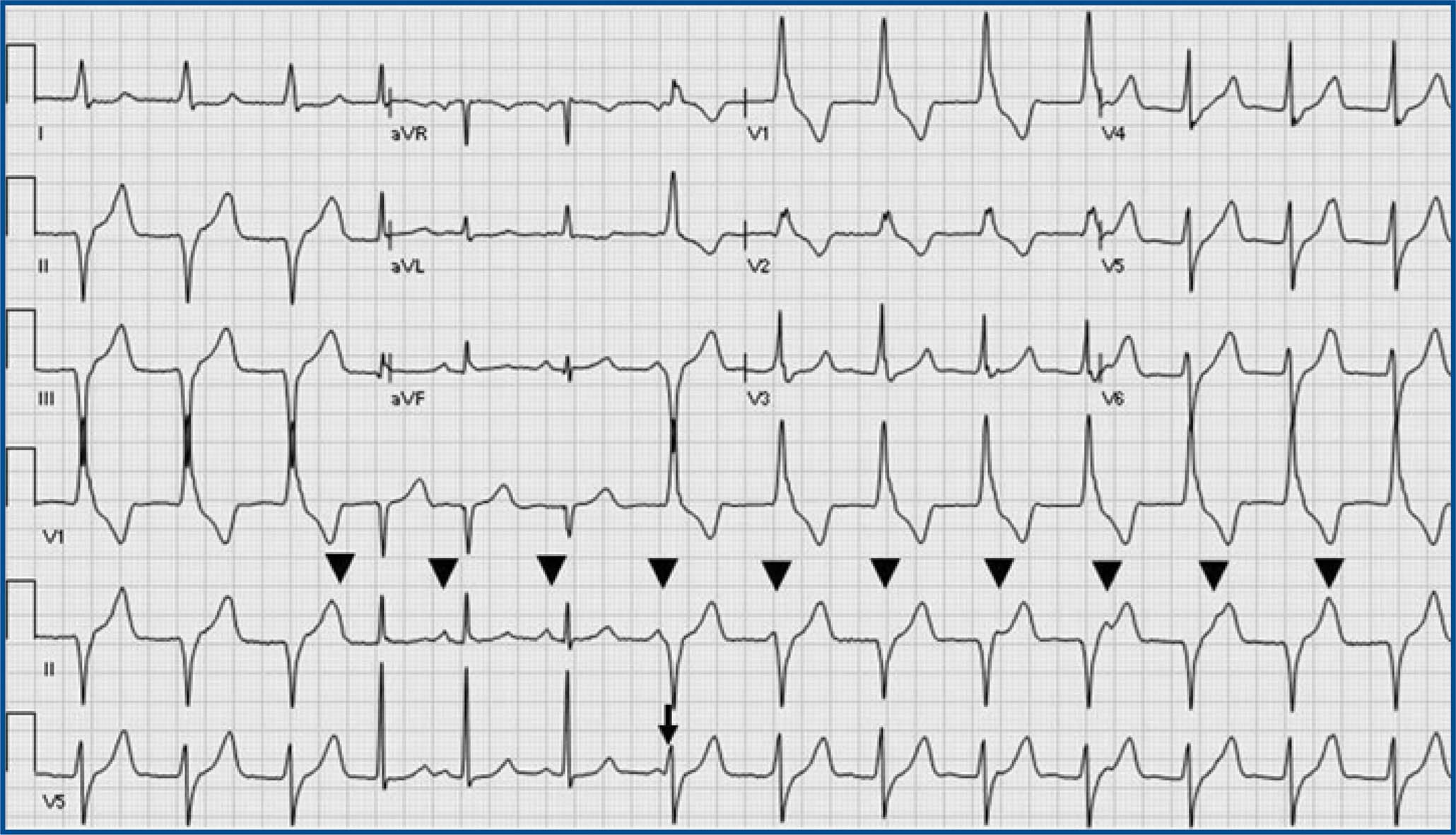
Accelerated Idioventricular Rhythm (AIVR) and sinus rhythm: AIVR starts and terminates gradually, competing with sinus rhythm. A possible ventricular fusion beat (arrow) and isoarrhythmic AV dissociation (arrowheads: sinus P waves) are present. During AIVR, ectopic ventricular rate is just faster than sinus rate. AIVR has a wide QRS morphology different from the QRS morphology in sinus rhythm.
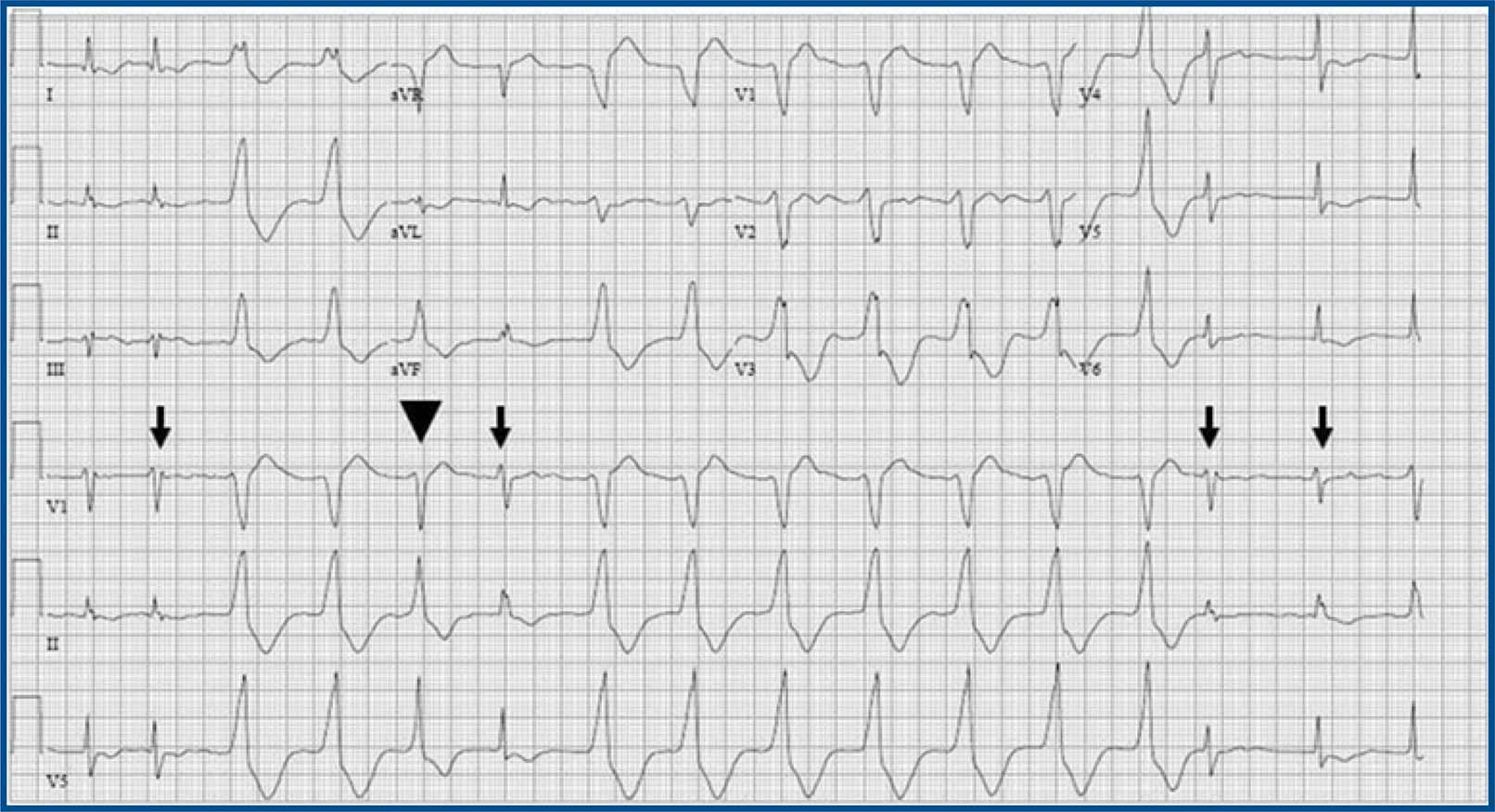
Accelerated Idioventricular Rhythm. AIVR in atrial fibrillation: AIVR starts and terminates gradually, competing with the ventricular capture beats (arrow) from atrial fibrillation. Ventricular fusion beat (arrowhead) is present. AIVR has a wide QRS morphology different from the QRS morphology of ventricular capture beats.
Junctional escape rhythm. Complete heart block with junctional escape rhythm: The AV dissociation in complete heart block is not isoarrhythmic AV dissociation, because the atrial rate is much faster than the ventricular rate of the junctional escape rhythm.
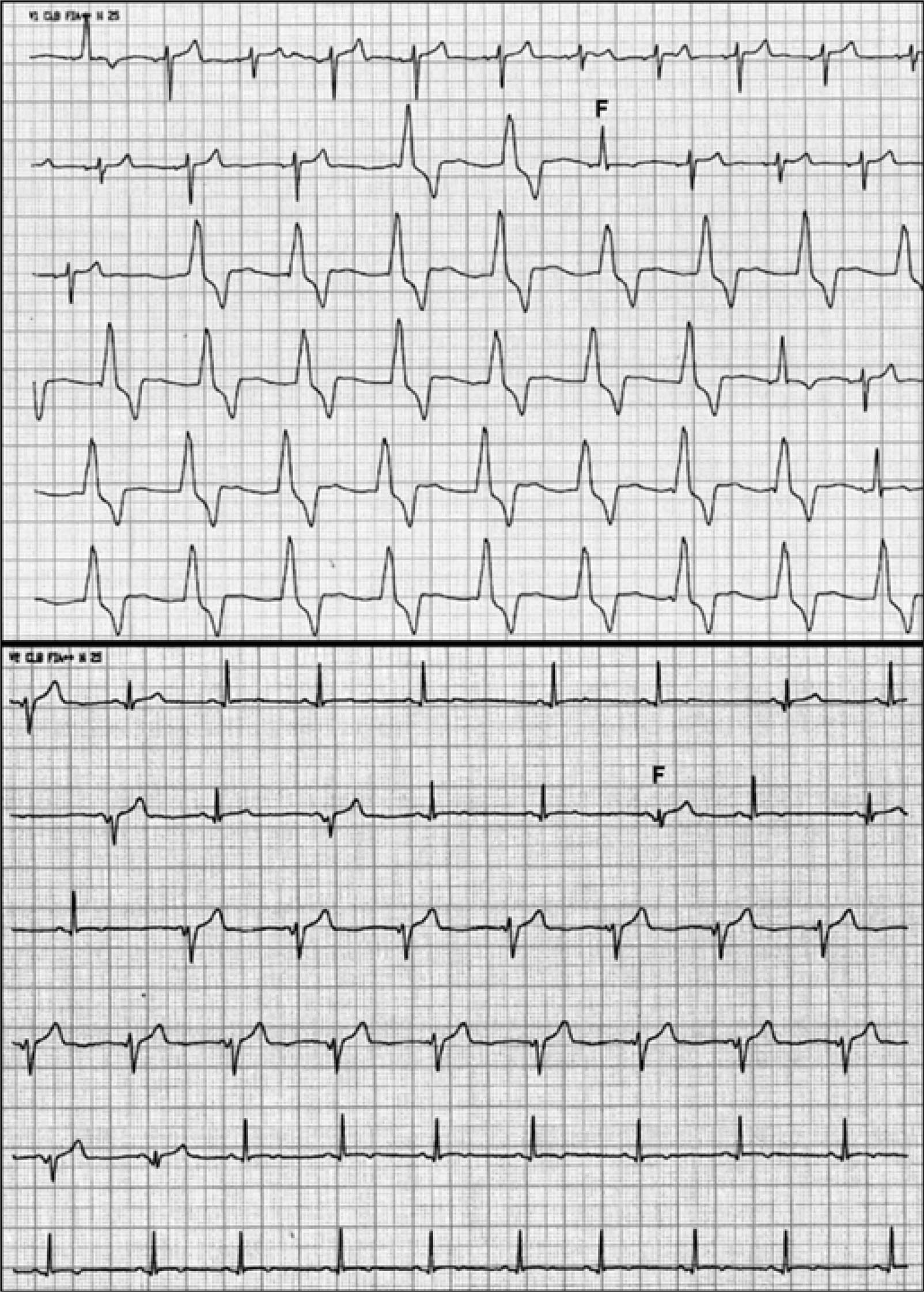
These ECGs belongs to a young, asymptomatic, Caucasian patient, without cardiovascular history, who practiced physical activities regularly. He had been treated with azithromycin for an upper airway infection. Both panels show sinus rhythm alternating with AIVR at approximately 60 bpm. Note fusion beats (F).
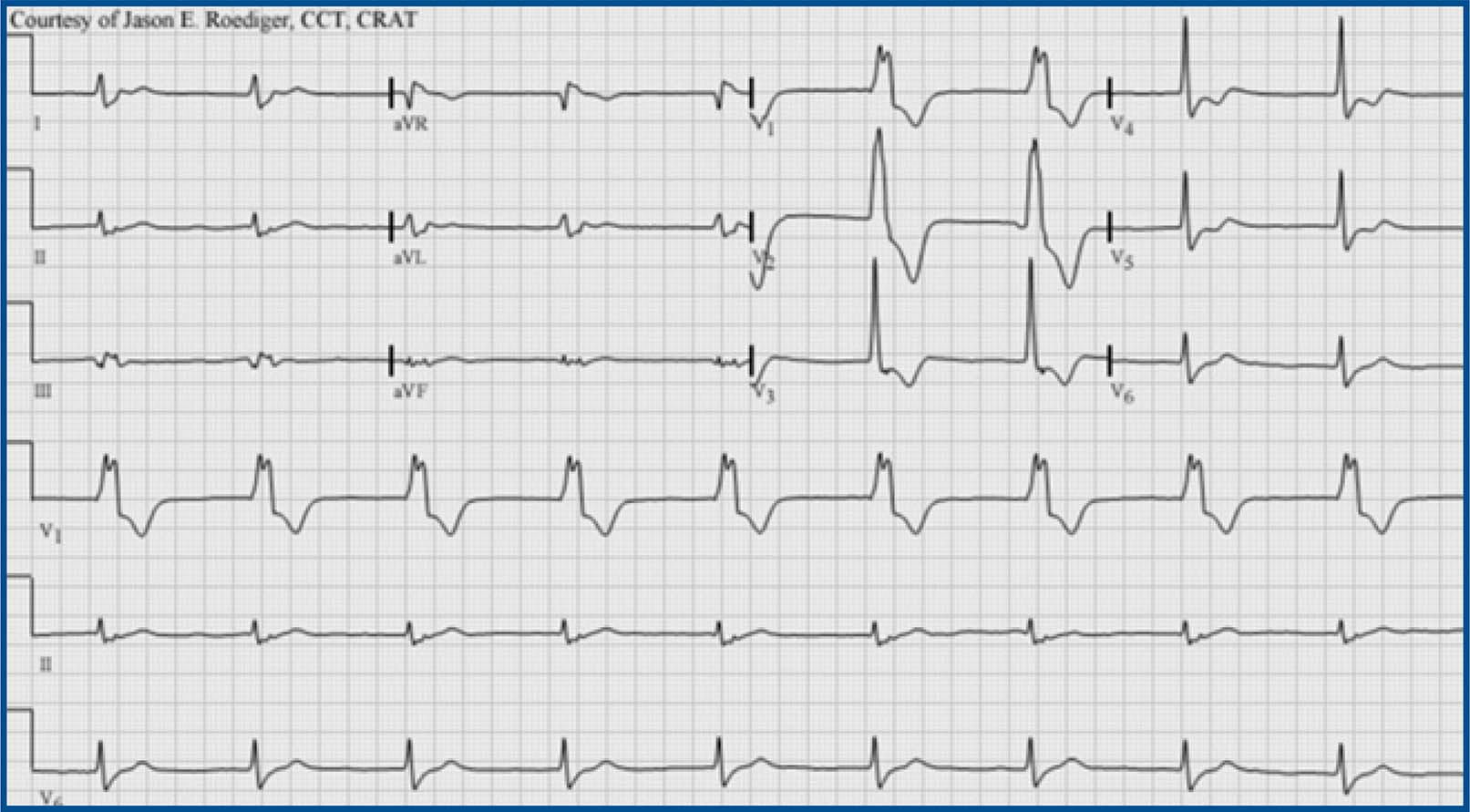
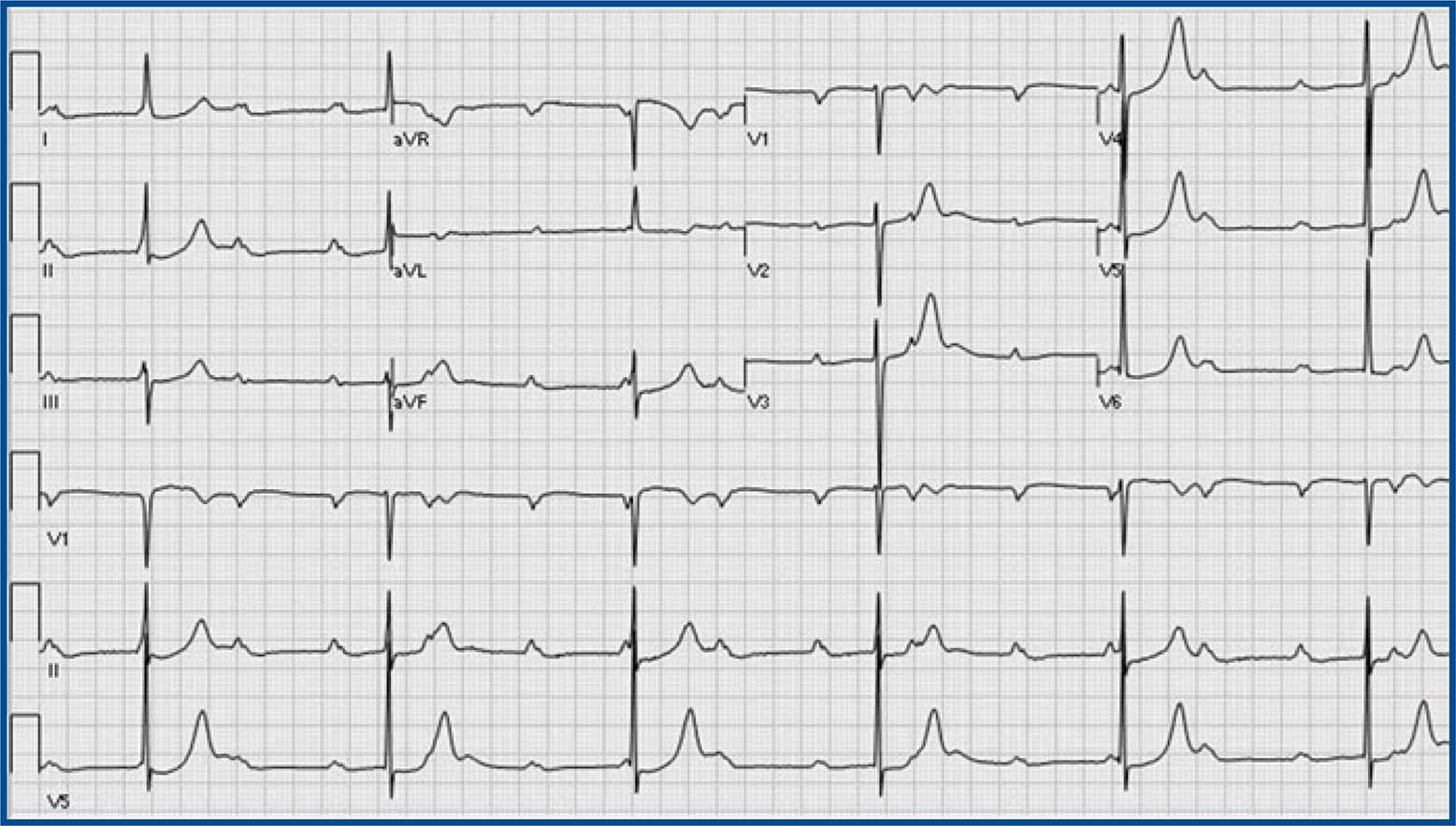
Accelerated idioventricular rhythm (AIVR), HR 55bpm, focus originating from the left ventricle: RBBB-like pattern in V1. Note the typical QRS morphology in lead V1 characteristic of ventricular ectopy from the LV. Monophasic R-wave with smooth upstroke and notching on the downstroke (i.e., the so-called taller left peak or “rabbit-ear”.) Contributed Courtesy of Jason E. Roediger (CC BY-SA 3.0 https://creativecommons.org/licenses/by-sa/3.0/deed.en).
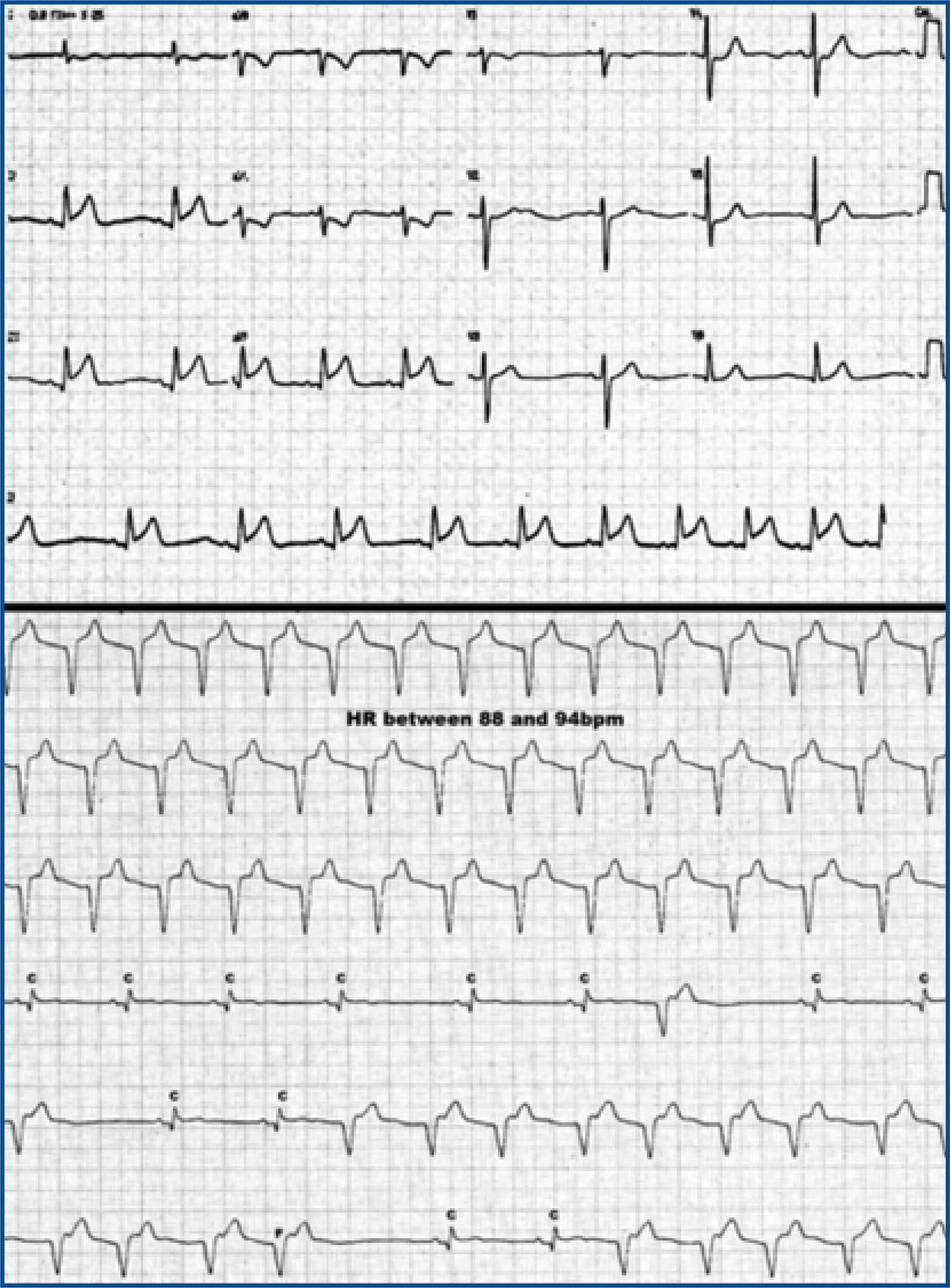
This ECG belongs to an elderly woman with acute ST-elevation myocardial infarction (superior panel). During thrombolytic administration, AIVR occurred (inferior panel). The heart rate is 88 bpm. AIVR alternates with sinus captures (C) and fusion beats (F). Sinus capture occurs when the sinoatrial node temporarily “captures” the ventricles, producing a QRS complex of normal duration. This can occur when the sinus rate is faster than the idioventricular rate. Fusion beats are hybrid complexes that occurs when a sinus and ventricular beat happen at the same time.

