











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo

 Permalink
Permalink
INTRODUCTION
Chest pain is one of the most common causes of hospitalization in emergency departments, affecting approximately 70% of patients with acute coronary syndrome. This syndrome is characterized by ischemic manifestations of the myocardial muscle due to complete or partial occlusion of the coronary arteries and can be divided into three clinical forms: unstable angina, non-ST-segment elevation myocardial infarction, and ST -segment elevation myocardial infarction. These severe conditions require nurses to exercise clinical reasoning to make quick and safe decisions1,2.
Risk classification is a tool that helps nurses, through qualified listening, to take on the role of regulating care demand and determining the priority of care for these patients. These professionals are responsible for using protocols to optimize and provide quality care.
During the admission of a patient with chest pain, the nurse’s assessment becomes essential, as he or she is the professional responsible for classifying risk and regulating care demand, determining the priority of care and referring the patient to the treatment area according to their demands, in an agile and effective manner3.
To this end, the use of assistance instruments, such as flowcharts, can contribute to nursing care through the standardization of care in the initial care of patients with chest pain, providing greater safety and agility in work processes, as it guides decision-making and also contributes to the training and qualification of nursing professionals in emergency services4.
Flowcharts can also assist nurses in their management activities by reducing costs and the risk of duplicating tasks. They also improve the effectiveness of care and, consequently, patient safety, in addition to aiding in the visualization of information4,5.
However, the assistance instruments available in the scientific literature for treating patients with chest pain present decision-making that guides, almost exclusively, medical conduct and does not consider the diversity of nursing actions.
The development of a care flow based on nursing interventions and activities and the main guidelines and recommendations of good practices, allows the nurse and the nursing team to quickly visualize specific nursing actions for these patients in the emergency room6.
Thus, the objective is to develop and validate a nursing care flowchart for approaching patients with acute coronary syndrome in emergency services, aiming at standardizing procedures and improving the quality of care.
METHODS
Study design
This is a methodological study to develop a flowchart based on the care sequence of the American Heart Association Acute Coronary Syndrome Algorithm7. Three stages were followed: In the first stage, an integrative literature review was carried out to identify the main clinical indicators for patients with chest pain associated with acute coronary syndrome, adapted by the Preferred recommendation Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA Statement)8. In the second stage, cross-mapping was carried out and in the third stage, validation by judges.
Place and period of study
This study is the result of a master’s dissertation completed in a Professional Master’s Program in Nursing located in the state of Espírito Santo. The database search was conducted between May and August 2021.
First stage: integrative literature review
To carry out the integrative literature review, the following steps were followed: elaboration of the guiding question; literature search; data collection; critical analysis and discussion of the results9.
The guiding research question was formulated using the Patient - Intervention-Outcomes (PIO) strategy, a variation of the Patient-Intervention-Comparison- Outcomes (PICO) strategy, considering the acronym P (Population) as patient with acute coronary syndrome; the acronym I (Intervention) as clinical indicators in patients with chest pain; and the acronym O (Outcome) as identification of nursing interventions and activities9. Thus, the guiding question was formulated as follows: What are the clinical indicators found in patients with chest pain in acute coronary syndrome? Signs, symptoms, and complications were considered clinical indicators.
Data were collected from the following databases: Medical Literature Analysis and Retrieval System Online (MEDLINE), Latin American and Caribbean Literature on Health Sciences Information (LILACS) and Cumulative Index to Nursing and Allied Health Literature ( CINAHL). Articles indexed in CINAHL were accessed through the CAPES portal, and the search for MEDLINE and LILACS publications was conducted through the Scientific Electronic Library Online (SciELO) and the Virtual Health Library (VHL).
Health Science Descriptors (DeCS/MeSH) in Portuguese and English were used: “signs and symptoms / signs and symptoms”, “chest pain/chest pain”, “complications / complications ”and “acute coronary syndrome / acute coronary syndrome”, crossed with each other using the Boolean resource “AND”.
The inclusion criteria were articles available in full, in Portuguese, English, and/or Spanish, published between 2016 and 2020, focusing on adults, and addressing the guiding question. Literature reviews, letters to the editor, editorials, case reports, abstracts published in conference proceedings, personal opinions, dissertations, theses, book chapters, institutional manuals, and articles on virtual and hybrid simulation scenarios were excluded.
The studies were selected, first by reading titles and abstracts, with the participation of two independent researchers with the help of a free web review program , with a single version, called Rayyan Qatar Computing Research Institute ( Rayyan QCRI)10, given its ability to facilitate initial screening by excluding duplicate articles and incorporating a high level of usability and selection effectiveness, with blinding of the auxiliary researcher, identified at the link https://rayyan.qcri.org/.
Next, the selected studies were read in full and their reference lists were checked to include new articles, obtaining the desired final sample.
Second stage: Cross-mapping and elaboration of the Flowchart
In the second stage of the research, the clinical indicators found in the integrative review were grouped according to their clinical similarities. Then, a standard term similar to that found in NANDA was determined – International11 that defined them and organized them into a standardized language . Subsequently, the clinical indicators were mapped with nursing interventions and activities. Intervention Classification (NIC)12.
Cross-mapping is defined as a method that seeks to identify applicable, comparable and understandable terms from a standard language with the objective of validating information in different contexts and realities13, making it possible to produce teaching materials that can be incorporated into clinical nursing practice as they support decision-making through clinical reasoning14.
To develop the cross-mapping, six rules were determined based on the characteristics of the data obtained and the classification applied , adapted from the methodological framework used by Moorhead and Delaney13 and Lucena and Barros15, described below: 1) determine a keyword ( standard term ) that clearly describes the clinical indicator; 2) select the most relevant diagnosis and interventions based on their similarity with the clinical indicator or its definition; 3) list the activities corresponding to the interventions based on the similarity between these and the clinical indicator that describe the reality of emergency nursing care practice; 4) map the clinical indicator in different interventions, when the actions and/or results are distinct; 5) identify the clinical indicator that cannot be mapped.
The results were analyzed through thematic analysis, in three phases: (1) pre-analysis with a cursory reading of evidence; (2) organization of convergent information and exploration of findings with grouping of convergences and (3) data processing, listing the categories16. Afterwards, the information obtained was interpreted and the synthesis of knowledge was presented.
Thus, the care flowchart was structured based on the precepts and recommendations of good practices, considering the main clinical indicators, stratified by the degree of complexity presented by the patient during the phases of emergency care, and the nursing activities found through cross-mapping.
Third stage: focus group assessment and validation by judges
The study population consisted of nurses who comprised the focus group and the panel of judges, respectively, who assessed the content and validated the instrument. For both groups, the following inclusion criteria were used: being a nurse with at least two years of clinical experience in an emergency room or a specialization program in emergency room nursing, cardiology, critical care, intensive care, and/or coronary care.
The focus group is considered a qualitative research technique that proposes the collection of information through group interactions, based on communication, with the main purpose of gathering the maximum amount of information on a given topic, in a way that can provide an understanding of perceptions, beliefs and attitudes on a given subject17.
Nurses working in the emergency departments of the same hospital where the researcher works and who met the inclusion criteria were invited to participate in the focus group. Nurses who were unable to attend the meetings on the scheduled days were excluded from the group. During the meetings, the study proposals were presented, and upon acceptance, participants were required to sign the Free and Informed Consent Form (FICF) as a criterion for group participation. The focus group meetings were held in March and April 2023 and were attended by seven nurses. These nurses reviewed the content of the first version of the flowchart, assessing the adequacy of the priority and complexity of care.
During the meetings, participants were able to provide feedback on the maintenance, relocation, or removal of components from the service flowchart. Once all participants reached consensus, the changes were analyzed and implemented.
The other study population consisted of nurses who acted as judges, responsible for evaluating the second version of the care flowchart regarding clinical relevance, practical relevance and clarity of language.
The search for judges was conducted through the researcher’s network of contacts and a snowball sampling technique. After selection, based on the aforementioned criteria, the judges were contacted via email, to which a form prepared using Google Forms was sent. This form consisted of five sections: Section 1 contained the letter of invitation to participate in the study; Section 2 the Informed Consent Form (ICF); Section 3 presented the research steps; Section 4 contained the participant characterization form; and Section 5 contained the evaluation items. Only participants who agreed to participate by accepting the ICF were allowed to proceed to Session 3. Judges who did not return the form within the 15-day time limit were excluded from the study.
Data analysis
To assess inter-judge agreement, the Content Validity Index (CVI) was used, which measures the proportion or percentage of judges in agreement on certain aspects of the construct and its items. It allows for the initial analysis of each item individually and then the construct as a whole18.
The item that obtained a CVI ≥0.80 among the judges was considered to have evidence of validity. Items that had a lower average were modified or excluded, as suggested.
Likert- style scale was applied, divided into three evaluation points and three levels of analysis. The first point assessed clinical relevance: 1 - not at all relevant, 2 - somewhat relevant, 3 - very relevant; the second point assessed relevance to the nursing team’s performance: 1 - not at all relevant, 2 - somewhat relevant, 3 - very relevant; and the third point assessed clarity of language: 1 - not at all clear, 2 - somewhat clear, 3 - very clear. Spaces were also provided for suggestions. The formula for evaluating each item individually is presented below:
Ethical and legal aspects
The ethical and legal principles of research involving human beings were respected, as established by Resolutions Nº. 466/2012 and Nº. 510/2016 of the National Health Council (CNS). This research was approved by the Ethics Committee for Research involving Human Beings of the Cassiano Antônio de Moraes University Hospital (HUCAM), CAAE Nº. 21160719.7.0000.507, under Nº. 3,698,598.
RESULTS
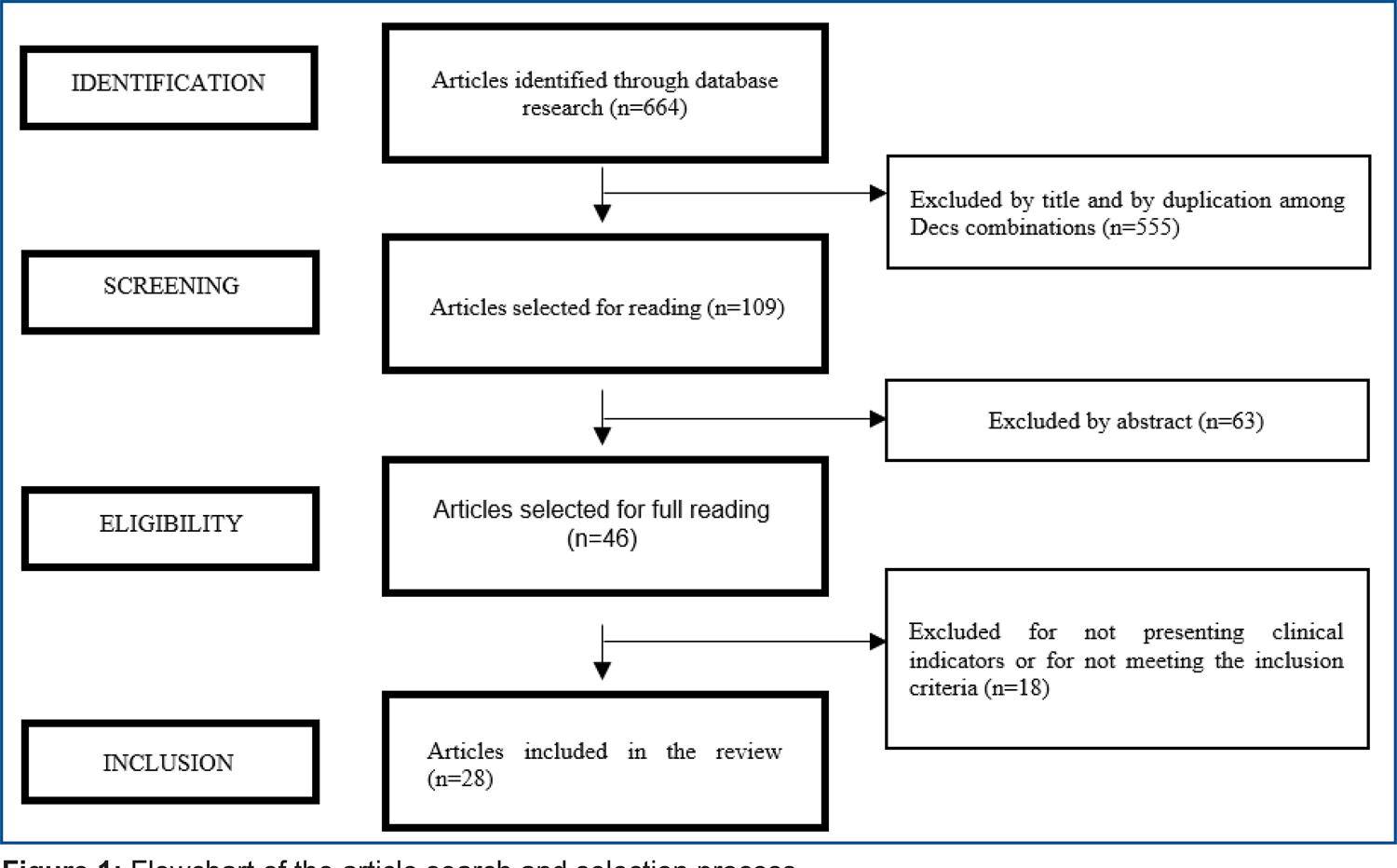
During the integrative literature review process, 664 articles were found, of which 59 were excluded due to duplication, 496 after reading the titles and 63 after reading the abstracts, leaving 46 full articles. Furthermore, 18 studies were excluded because they did not answer the guiding question, leaving 28 articles to be included in the integrative review (figure 01).
Regarding the databases, 3 (11%) studies were accessed via LILACS and 25 (89%) via MEDLINE. Among the journals, the Journal of the American Heart Association and the American Journal of Cardiology, both with 3 (11%) indexed searches.
Regarding methodology, 8 (29%) articles were clinical trials, 7 (25%) retrospective studies, 6 (21%) cross-sectional studies, 4 (14%) prospective studies, 1 (4%) descriptive exploratory study, 1 (4%) cohort study, and 1 (4%) with a quantitative approach.
Of the 28 articles, 199 clinical indicators were identified which, after grouping, resulted in 38 standard terms (Chart 1).
Chart 1 : Clinical indicators found in the literature review and their respective standard terms for patients with chest pain related to acute coronary syndrome . Vitória, ES, Brazil, 2025
| Clinical indicators | Standard terms |
|---|---|
| Ventricular ejection fraction <40% (n: 1) Depressed left ventricular ejection fraction (<35%) (n: 1) Low left ventricular ejection fraction (n: 1) Decreased left ventricular ejection fraction (n: 1) Ventricular dysfunction with left ventricular ejection fraction <35% (n: 1) Reduced ejection fraction (n: 2) Preoperative left ventricular ejection fraction ≤35% (n: 1) Severe left ventricular dysfunction (ejection fraction: 25%) (n: 1) Impaired left ventricular function (LVEF <50%) (n: 1) Preoperative severe left ventricular dysfunction (n: 1) Decrease in left ventricular flow (n: 01) | Decreased ejection fraction |
| Peripheral edema (n: 1) Edema (n: 5) Anasarca (n: 01) Reduced extra-to-intravascular space fluid mobilization (n: 01) Reduced peripheral capacitance blood mobilization (n: 01) Lower body negative pressure (n: 02) | Edema |
| Postoperative atrial fibrillation (n: 02) Electrocardiogram abnormalities (Left Bundle Branch Block or Atrial Fibrillation) (n: 01) Changes in the electrocardiogram (n: 02) Arrhythmias (n: 04) Altered Rhythm (n: 01) | Change in electrocardiogram (ECG) |
| Blood pressure changes (n: 2) Decrease in blood pressure (n: 01) Hypotension (n: 2) High blood pressure (n: 2) Hypertension (n: 01) Increased baroreflex sensitivity (n: 01) | Change in blood pressure |
| Dyspnea (n: 05) Changes in breathing pattern (n: 01) Bronchospasm (n: 01) Hypoxemia (n: 01) Pulmonary congestion (n: 1) | Dyspnea |
| Acute renal failure (n: 04) Acute kidney injury (n: 01) Elevated creatinine levels (n: 01) Creatinine change (n: 01) Azotemia (n: 01) | Altered renal function |
| Increased insulin clearance (n: 01) Decreased insulin-C-peptide ratio (n: 01) Hyperglycemia (n: 01) Elevated glucagon (n: 01) Diabetes (n: 01) Diabetes mellitus (n: 01) Impaired glucose homeostasis (n: 01) Low fasting plasma glucose (n: 01) | Unstable blood glucose |
| Infectious complications (n: 01) Sepsis (n: 01) Mediastinitis (n: 01) Deep sternal wound infection (n: 2) Active endocarditis (n: 01) Increased inflammatory response (n: 01) Wound infections (n: 01) | Infection |
| Tachycardia (n: 03) Postural tachycardia syndrome (n: 01) Altered heart rate (n: 02) | Tachycardia |
| Echocardiographic changes (n: 02) Left trunk disease (n: 01) Triple vessel disease (n: 01) Double vessel disease (n: 01) Valvular disease with previous moderate to severe pulmonary hypertension (n: 01) | Changes in cardiac structure and function |
| Reduced systolic function (n: 01) Systolic heart failure (n: 01) Decrease in stroke volume (n: 01) Stroke volume reduction (n: 01) Altered Stroke Volume (n: 01) Decreased stroke volume index (n: 01) | Decreased stroke volume index (SVI) |
| Chest pain (n: 1) Chest pain (n: 2) Angina at rest (n: 01) Pain (n: 01) | Chest pain |
| Jugular vein distension (n: 2) Jugular distension (n: 01) Jugular venous distension (n: 01) Positive hepatojugular reflex (n: 01) | Jugular vein distension |
| Rales (n: 02) Rales and crackling (n: 1) Crackling (n: 1) Altered lung auscultation (n: 01) | Adventitious respiratory sounds |
| Orthopnea (n: 03) Apnea-hypopnea index ≥ 5/h (n: 1) | Orthopnea |
| Bradyarrhythmia (n: 01) Bradycardia (n: 02) Reduction in heart rate (n: 01) | Bradycardia |
| Mechanical ventilatory assistance (n: 01) Mechanical ventilation (n: 02) Prolonged ventilation (n: 01) | Ventilatory assistance |
| Postoperative bleeding (n: 01) Bleeding (n: 03) | Bleeding |
| Anxiety (n: 4) | Anxiety |
| Fatigue (n: 3) Tiredness (n: 1) | Fatigue |
| Change in skin color (n: 3) Flushed skin (n: 01) | Abnormal skin color |
| Activity intolerance (n: 01) Weakness (n: 01) Physical fragility (n: 01) | Activity intolerance |
| Change in mental state (n: 01) Mental confusion (n: 01) Neurological complications (n: 01) | Confusion |
| Restlessness (n: 01) Agitation (n: 2) | Restlessness |
| Paroxysmal nocturnal dyspnea (n: 2) Sleep-disordered breathing (n: 01) | Paroxysmal nocturnal dyspnea |
| Hypoperfusion (n:01) Cerebral hypoperfusion (n:01) Reduced cerebral blood flow (n: 01) | Decreased cerebral perfusion |
| Increased systemic vascular resistance (n: 03) | Increased systemic vascular resistance (SVR) |
| Renal replacement technique (n: 01) Renal replacement therapy (n: 02) | Renal replacement therapy |
| Oliguria (n: 2) / Anuria (n: 01) | Oliguria/Anuria |
| Third heart sound (S 3 gallop) (n: 1) Sound S3 (n: 1) B3 sound( n: 1) | Presence of 3rd heart sound (S3) |
| Decreased peripheral perfusion (n: 01) Cyanosis (n: 02) | Prolonged capillary refill time |
| Palpitation (n: 2) | Heart palpitations |
| Fourth heart sound (S 4 gallop) (n: 1) Sound S4 (n: 1) | Presence of 4th heart sound (S4) |
| Postoperative cardiac arrest (n: 01) Respiratory arrest (n: 01) | Cardiopulmonary arrest |
| Cold and clammy skin (n: 01) Cold and clammy skin (n: 01) | Sticky skin |
| Cough (n: 2) | Cough |
| Cardiac index < 2.0 l/min/m2 (n: 01) Cardiac index < 2.5l/m/m2 (n: 01) | Decreased cardiac index |
| Vasovagal syncope (n: 02) | Syncope |
The standard terms were mapped with 17 nursing interventions and 115 nursing activities present in the NIC, being: 05 interventions of the Basic Physiological domain in five classes (Elimination Control, Immobility Control, Nutritional Support, Promotion of Physical Comfort and Facilitation of Self-Care); 07 (63%) interventions of the Complex Physiological domain in seven classes (Electrolyte and Acid-Base Control, Medication Control, Neurological Control, Respiratory Control, Skin/Injury Control, Thermoregulation and Tissue Perfusion Control); 01 (02%) intervention of the Behavioral domain in one class (Promotion of Psychological Comfort); 02 (10%) interventions of the Safety domain in two classes (Crisis Control and Risk Control) and 02 (07%) interventions of the Health System domain in two classes (Health System Mediation and Health System Control). No clinical indicators were mapped in the Family and Community domains.
Afterwards, the care flowchart was structured and presented for content assessment in focus group meetings, composed of 7 nurses, who redefined the terminology to “Patient admitted via Spontaneous Demand” and “Patient referred via SAMU”.
Regarding the clinical criteria assessed for patient admission during Risk Classification using the Manchester Protocol, the group added “Altered level of consciousness”; redefined the “Chest pain” indicator to “Precordial or cardiac pain”; and preferred to use “ Acute dyspnea and very low SatO2” instead of “Tachypnea (RR: 25 IRPM) and SatO2 < 92%.” Participants unanimously maintained the bradycardia value (HR <50 bpm), but focused more discussion on the tachycardia value, which was defined as greater than 140 beats per minute. There was also consensus on the systolic blood pressure value equal to or less than 80 mmHg.
For patients under clinical observation, the focus group suggested adding a care process box called “ Observation Follow-up” containing nursing activities. The addition of hygiene-related activities to the flowchart was also suggested and accepted.
The focus group requested that electrocardiograms be performed daily for up to 96 hours, considering the time of admission to the cardiac emergency department. The following nursing activity was also added: “Arrange for an electrocardiogram within 10 minutes,” correlating with the recommendations for the test to be performed within the first few minutes of care.
The group discussed that fluid balance should be performed every six hours and vital signs should be recorded according to the complexity and clinical response of the patient.
Everyone agreed that the service should be organized by level of complexity in the flowchart and that similar activities should be excluded in order to bring more objectivity.
After assessment and adjustments made by the focus group, 18 judges were invited to carry out the content validation process. However, only 8 participated in the research: 5 (62.5%) were female; 3 (37.5%) with a lato sensu postgraduate degree and 5 (62.5%) with a stricto sensu postgraduate degree (master’s/doctorate); 1 (12.5%) with a specialization in Urgency and Emergency, 2 (25%) in Intensive Care, 2 (25%) in Cardiology Nursing and 3 (37.5%) with other specializations; 3 (37.5%) have worked or work as a teacher and 4 (50%) have worked or work with clinical research. The average time working in Urgency and Emergency was 9 years. The average age among the judges ranged from 31 to 40 years.
According to the responses regarding clinical relevance, practical relevance and clarity of language, the items evaluated by the judges obtained a CVI equal to or greater than 0.80 in two or more requirements (table 1).
Table 1 : Validation process of items in the nursing care flowchart structures for acute coronary syndrome in the emergency room . Vitória, ES, Brazil, 2025
| Flowchart structure | PC* | RP* | CL* |
|---|---|---|---|
| BOX 01: Emergency room | 1.0 | 1.0 | 1.0 |
| BOX 02: Chest Pain, ECG Change, Tachycardia, Bradycardia, Heart Palpitations | 1.0 | 1.0 | 1.0 |
| BOX 03: Dyspnea, Ventilatory assistance, Fatigue, Adventitious respiratory sounds | 1.0 | 1.0 | 1.0 |
| BOX 04: Cardiogenic shock, Change in blood pressure, Hemodynamic instability | 0.87 | 0.87 | 0.75 |
| BOX 05: Unstable Blood Glucose | 1.0 | 1.0 | 1.0 |
| BOX 06: Bleeding, Clammy skin, Abnormal skin color, Diminished peripheral pulses, Prolonged capillary refill time | 1.0 | 1.0 | 1.0 |
| BOX 07: Decreased cerebral perfusion, Drowsiness, Syncope, Headache, Dizziness | 1.0 | 1.0 | 1.0 |
| BOX 08: Edema, Jugular vein distension, Cough, Activity intolerance | 1.0 | 1.0 | 1.0 |
| BOX 09: Oliguria/Anuria, Altered renal function, Renal replacement therapy | 1.0 | 1.0 | 1.0 |
| BOX 10: Infection Anxiety, Confusion, Restlessness, Constipation | 1.0 | 1.0 | 1.0 |
| BOX 11: Anxiety, Confusion, Restlessness | 1.0 | 1.0 | 1.0 |
| BOX 12: Constipation | 0.87 | 0.87 | 1.0 |
| BOX 13: Clinical indicators for transfer to the emergency room assessed in the Risk Classification. | 0.87 | 0.87 | 0.87 |
| BOX 14: Follow-up observation | 1.0 | 1.0 | 1.0 |
| BOX 15: Discharge Guidelines | 1.0 | 1.0 | 0.75 |
| BOX 16: Emergency care | 0.87 | 1.0 | 0.75 |
| BOX 17: Admission care | 1.0 | 1.0 | 1.0 |
| BOX 18: Routine care | 1.0 | 1.0 | 1.0 |
| BOX 19: Transfer Care | 1.0 | 1.0 | 1.0 |
Abbreviations: PC* - Clinical Relevance; RP* - Practical Relevance; CL* - Clarity of Language.
Considering that most items obtained evidence of validity among the judges with CVI ≥0.80, the suggestions made during the evaluation of each box were analyzed and many were incorporated into the flowchart in order to enrich it with the experience and knowledge of the participants.
In the space provided for suggestions in BOX 01, the judges indicated obtaining or changing peripheral venous access to the left upper limb, favoring the right upper limb for performing procedures via the right radial artery.
They also suggested the inclusion of 12 precordial leads for performing an electrocardiogram and reinforced the importance of patient identification.
Regarding emotional support, they expressed special attention in BOX 02, incorporating the activity “ Provide factual information regarding diagnosis, treatment and prognosis”.
The nursing activities “Keep the head of the bed elevated at 30 to 45 degrees, except when contraindicated (i.e., hemodynamic instability)” and “Document all changes in the respirator configuration, with justification for changes” were also added to BOX 03.
BOX 04 received a CVI of 0.75 for clarity of language. Therefore, the judges suggested performing a fluid balance, although this activity is detailed in the box labeled “Routine Care.” They also suggested describing the signs and symptoms of decreased cardiac output in the activity “Monitor signs and symptoms of decreased cardiac output”.
The activity “Identify the patient’s cognitive or physical deficits that may increase the potential for falls” was included in BOX 07 due to the precaution regarding the risk of falls in light of the clinical indicators evaluated.
For patients who present anxiety, confusion, or restlessness, the judges suggested evaluating the need for physical restraint with other team members and considering the inclusion of a family member.
Regarding the clarity of language in the “Discharge Guidelines,” the CVI was 0.75, with adjustments requested by the judges, who suggested describing the characteristics of pain that would motivate seeking prompt help. However, after discussion, the researchers concluded that this issue is addressed in the activity “Provide guidance on signs/symptoms of early heart disease and worsening heart disease”.
Regarding “Admission care”, the activity “Ensure continuous ECG monitoring at the bedside” was added at the suggestion of the judges.
In “Routine Care”, the activity was modified to “Obtain an ECG when necessary and within 96 hours of admission”, allowing for identification of changes. The activities “Document assessments, diagnoses, interventions, and outcomes of nursing care provided”, documenting nursing records, and “Use an assessment tool for risk of skin breakdown and falls”, were also included , as suggested.
Thus, the nursing care flowchart, in its final version, was structured as follows (figure 02).
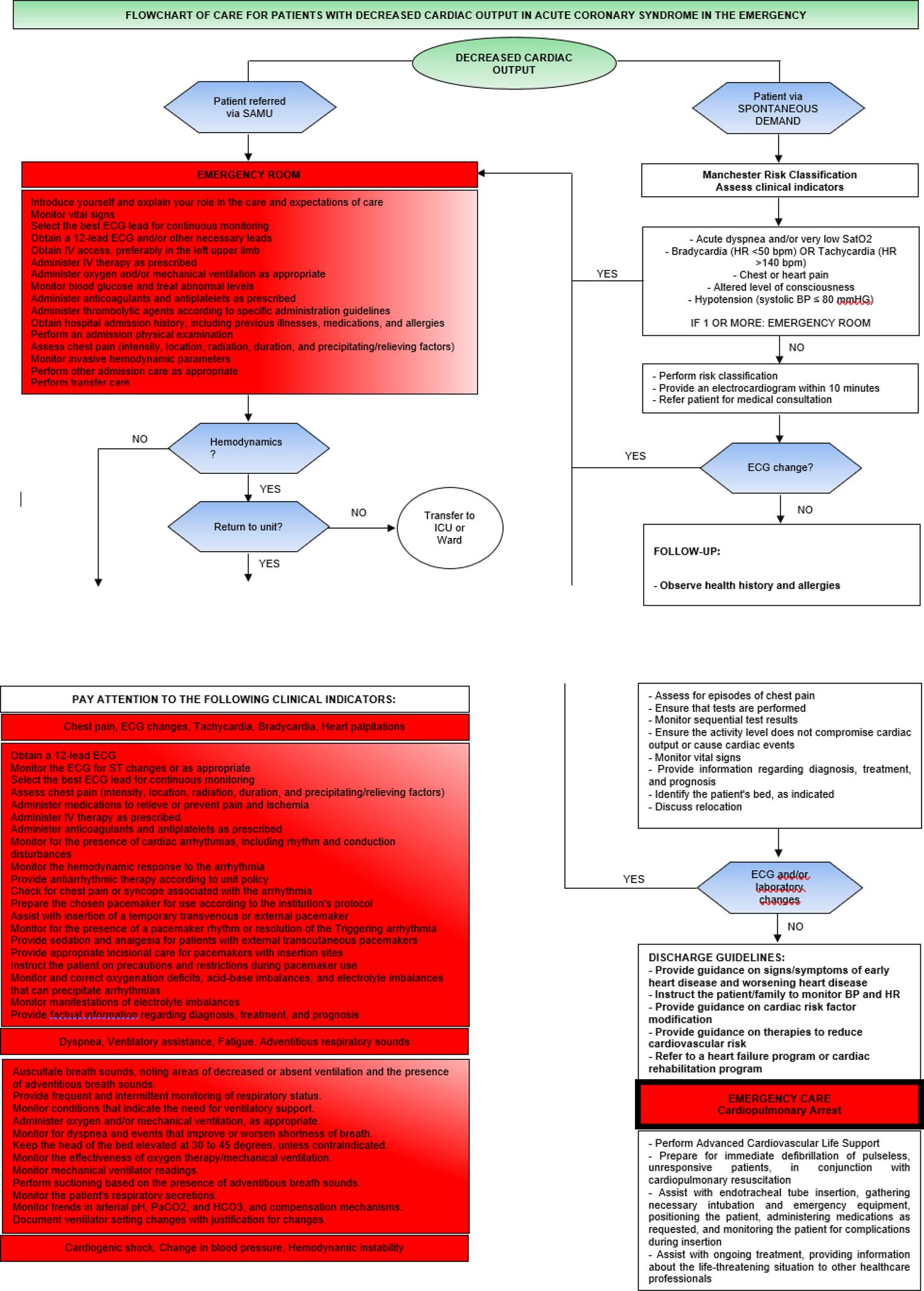
Figure 2a : Nursing care flowchart for patients with chest pain in acute coronary syndrome in the emergency room, Brazil, 2025. Source: Prepared by the authors

DISCUSSION
This research developed and validated a nursing care flowchart for patients with chest pain associated with acute coronary syndrome treated in an emergency unit, based on the care sequence of the American Heart Association Acute Coronary Syndrome Algorithm.
This flowchart is considered a unique care tool because it encompasses a set of clinical indicators that can contribute to nurses’ decision-making for the standardization of actions during the different phases of emergency care for patients with acute coronary syndrome, based on the main nursing interventions and activities and the main guidelines and recommendations for good practices.
In the admission stage of the flowchart, the inclusion of the assessment of precordial or cardiac pain becomes of great importance, as it is considered the most common manifestation of acute coronary syndrome19. It is characterized by the Levine sign, which contributes to the suspicion of ischemia, where the patient places the clenched fist on the sternum, and describes the pain as a sensation of tightness or burning that can spread to the upper limbs and face20.
Other typical symptoms, such as dyspnea, bradycardia, altered level of consciousness, hypotension, pain radiating to the jaw/neck, associated diaphoresis, and pain worsening with exertion, should also be assessed upon emergency room admission and become important markers for reducing nursing staff response time, helping to reduce complications and mortality. Furthermore, pain radiating to the right arm or both arms, vomiting, chest pain, and sweating made acute myocardial infarction more likely, considering advanced age, male gender, and electrocardiogram changes21.
Although the literature highlights these characteristic symptoms, considered typical, nursing staff should be aware that only 70% of patients admitted to the cardiac emergency room present one of these symptoms. Approximately 13% present none of these typical symptoms, and the use of clinical history alone is inadequate to reliably diagnose or exclude acute coronary syndrome22.
Another important factor to consider upon admission is age. However, although older adults have an increased risk of cardiovascular disease, care for young adults in cardiac emergency departments should not be neglected, considering the elevated risk of cardiovascular disease in this population, especially with heart failure23, although a study conducted in Brazil demonstrated a stabilization in the risk of death among young adults from coronary artery disease in recent years24.
After admission to the emergency department, patients presenting with chest pain with ischemic characteristics should immediately begin the Chest Pain Protocol, which prioritizes immediate nursing care. During this phase, the patient should be monitored and kept at rest, oxygen levels measured, and peripheral venipuncture performed for medication administration. In parallel, data collection begins, contributing to effective nursing care and promoting patient safety.
Another priority in nursing care is performing an electrocardiogram within the established 10-minute timeframe after the patient’s arrival, known as the door-to-electrode time. It is a painless, noninvasive, low-cost, and fast-acting test that captures electrical waves from the heart through electrodes attached to the patient, identifying possible coronary obstructions, heart chamber problems, and heart rate and rhythm26.
It is also important to highlight the importance of collecting laboratory tests, with troponin levels considered the gold standard in the diagnosis of acute myocardial infarction due to their extremely high sensitivity, allowing the identification of small myocardial lesions. Cardiac enzymes should be collected upon admission and again 6 hours after the first collection, to ensure accurate analysis and a definitive medical diagnosis27.
Considering the complexity of actions to be performed by the nurse in caring for these patients, the preparation of the care flowchart becomes fundamental with the aim of standardizing the assessment, management and treatment non-pharmacological , thus enabling more qualified and safe nursing care12.
Furthermore, the flowchart highlights the patient’s admission to the service: whether through spontaneous demand, preceded by the Manchester Protocol Risk Classification, whose outcome is determined by the patient’s clinical presentation, or through referrals via the Emergency Medical Service (SAMU), promptly admitted to the emergency room. In this phase, classified patients who show no signs of severity will remain under observation for diagnostic and therapeutic determination, while referred patients are quickly transferred to the therapy of choice with diagnostic confirmation, taking into account the recommended reperfusion times.
It is worth noting that the flowchart, developed in this study by professionals with clinical experience in emergency care , follows a sequence of care according to severity and/or complexity and, consequently, the nursing care inherent to each stage of the process. It includes discharge guidelines and highlighted boxes for emergency care, admission care, routine care, and transfer care.
Therefore, developing a nursing care flowchart for patients with acute coronary syndrome in the emergency room represents a novel, feasible, accessible, and necessary care technology for emergency services. It is based on the main interventions and activities contained in the NIC and on key guidelines and best practice recommendations.
Furthermore, it can be readily viewed by the nurse and the nursing team to define the appropriate actions to be followed and implemented, guided by the clinical indicator and the complexity presented by the patient during the different phases of care, assisting in decision-making, emphasizing the context of urgency and emergency, in addition to promoting and providing visibility to nursing conducts.

