










Services on Demand

article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators
Share

 Permalink
PermalinkPsicologia: teoria e prática
Print version ISSN 1516-3687
Psicol. teor. prat. vol.20 no.2 São Paulo May/Aug. 2018
https://doi.org/10.5935/1980-6906/psicologia.v20n2p339-352
ARTICLES
CLINICAL PSYCHOLOGY
Incident of femoral fracture and screening of signs of depression in the elderly
Ocurrencia del fractura femoral y rastreo del señales de depresión en mayores
Rosana Fortunato ModestoI; Edinalva Neves NascimentoII; Sandra Regina Gimeniz-PaschoalIII
IFaculty of Higher Education and Integral Training, FAEF, SP, Brazil
IISecretary of Health of Marília, SP, Brazil
IIIJúlio de Mesquita Filho São Paulo State University, Unesp, SP, Brazil
ABSTRACT
Femoral fractures in the elderly can cause physical, emotional, family and social problems. The objective of these studies was to identify the occurrence of hip fractures and to screening signs of depression in the elderly. Admission data were analyzed for the elderly of the Health Office of São Paulo city and interviews with 30 elderly people in their homes with the implementation of the Geriatric Depression Scale reduced Yesavage-version (GDS-15). We found that a period of one year, there were 94 admissions of elderly with hip fractures, mainly by falls in their homes, resulting in loss of autonomy, pain, and sorrow. Of those interviewed, 28 (93%) showed signs of depression, rating from mild to severe. We concluded that there was a high number of hospitalizations for hip fractures and signs of depression among the elderly, signaling the necessity of further investigations and actions which change that reality.
Keywords: care for the elderly; femoral fractures; depression; comprehensive health care; accident prevention
RESUMEN
Fracturas de fémur pueden causar problemas físicos, emocionales, familiar y social. El objetivo fue investigar la ocurrencia de fracturas de fémur y del los signos de depresión en las personas mayores. analizaron los datos de hospitales de los ancianos en Departamento de Salud en la ciudad de Sao Paulo y llevado entrevistas con 30 personas mayores en sus hogares con la aplicación de la Escala Depresión Geriátrica reduce Yesavage-versión (GDS-15). Se encontró que un período de un año, hubo 94 admisiones de la fractura en fémur de la tercera edad, principalmente por caídas en sus hogares, lo que resulta en la pérdida de la autonomía, el dolor y la tristeza. De los encuestados, 28 (93%) mostraron signos de la depresión, que van de leves a severos. No había número alto de fracturas de cadera y signos de depresión indica la necesidad de realizar investigaciones y acciones de modificar esta realidad.
Palabras clave: atención a las personas mayores; fracturas de fémur; depresión; atención integral de salud; prevención de acidentes.
Introduction
In the whole world, the life expectancy has grown progressively, becoming notable the existence of people more than a hundred years old (Rodrigues, Barbeito, & Alves Junior, 2016). Aging is a complex process, inherent to all the structures of the organism. Over time, the tissues start to be worn out and thus compromising the organs and their functions (Alencar, Bezerra, & Dantas, 2009). The compromise of the body structures facilitates risks for falls. Fall is not an intentional event, and its causes are multifactorial so that they can be both for intrinsic factors, like physiologic, pathologic and medical, and extrinsic factors, like inadequacy in the environment and footwear (Menezes & Bachion, 2008).
Most of the falls in the environment of the elderly occur because of inadequate illumination, loose carpets, the presence of steps, slippery surfaces, among others. It may cause fractures in femur, arms, forearms, face or even death, as well as psychologic changes like fear of falling and depression (Menezes & Bachion, 2008). The falls cause physical, functional and psychosocial consequences. Physical consequences are fractures, internment, immobilization, and neurological injury. Functional consequences are a restriction in mobility, change of habits, and dependence. Also, psychosocial consequences are the fear of falling, change of domicile, family rearrangement, social isolation, depression, and a decrease of self-esteem (Lopes & Dias, 2010).
A study performed in the University Hospital of Patras, in Greece, confirmed that falls in aged people cause physical damages that are immediately visible after their occurrence, and they can also cause significant problems in the psychological state of these people, such as anxiety, fear, and social isolation, linked to the event of depression (Mentis, Gouva, Antoniadou, Mpourdoulis, Kesoudidou, Marneras, & Panagiotopoulos, 2017).
There is a positive correlation between the depressive symptoms and the occurrence of the fall. A study performed with 68 elderly people in Vitória da Conquista, in the state of Bahia, twelve months after the accident, showed that 48,5% of the elderly people who fell present depressive condition such as fear, discouragement, irritability, social isolation and compromise in the ability to feel pleasure in life (Matias, Fonseca, & Matos, 2015). The depressive disorders may cause indifference to the environment, change in the level of attention, change in walking, decrease in energy, decrease in self-confidence, reclusion, and cognitive losses, especially among institutionalized elderly (Borges, Rocha, Couto, & Mancini, 2013).
A prospective study was performed in Taiwan between 2003 and 2007 with 4,547 elderly people with a diagnosis of femoral fracture. Only participants who did not present depressive signs before fracture were included in the research. The results showed that after the femoral fracture 1.2% (n = 55) of the participants started to present depression. The signs were more evident in the first 200 days and could be noticed until the first three years after the occurrence (Chang et al., 2014). Likewise, a study performed with 190 aged people with femoral fracture detected neuropsychic comorbidities during the hospitalization like, for instance, depression and dementia (Cunha & Veado, 2006). The presence of depression after a fracture is also a predisposing factor for the occurrence of other falls in the next two subsequent years (Berg1 et al., 2011).
Besides depression, other comorbidities were also identified like, for instance, respiratory problems, cardiac arrhythmia, and insufficiency, as well as cerebrovascular accident (Chang et al., 2014). Researchers showed that femoral fractures are also associated to decrease of the elderly. An epidemiologic study performed in a teaching hospital in the central region of São Paulo demonstrated that 48 of the 115 elderly people who fell had a femoral fracture. The fracture was associated to chronical diseases (especially renal failure), and it contributes to a rate of 7.1% of in-hospital mortality (Daniachi, Santos Netto, Ono, Guimarães, Polesello, & Honda, 2015). These data corroborate with the literature research that showed a rate of 21.85% of mortality in the first year among elderly people who had a femoral fracture (Mesquita, Lima, Santos, Alves, Brito, & Martins, 2009).
Considering the different consequences of falls with femoral fractures in elderly people and the need of implementation of public policies concerning this issue, this work aimed to identify the occurrence of femoral fracture and keep track of signs of depression in elderly people who suffered this kind of accident.
Method
This article is part of a bigger project submitted by the Municipal Secretariat of Health (SMS) of a medium-sized municipality in the countryside of São Paulo to the Health Surveillance Secretariat (SVS) of the Ministry of Health (MS), it was approved and funded by the federal government. The research proposal had the assent of the Research Ethics Committee, Protocol no. 0800/2013.
This is a descriptive study, with data collection about signs of depression in elderly people who had femoral fracture between September 2010 and October 2011. The elderly people who accepted to participate in the study and signed the Informed Consent Form, the elderly people who reside in the urban area of the municipality of study, and those whose residence was found during the home visiting were added. About the criteria of exclusion, those who did not consent to the carrying out of the interview, those who resided in the rural area, those who died, those who moved to other cities and those who changed their address inside the municipality of study but without the possibility of finding the new residing place, were excluded. We searched for the participation of the 94 elderly people in all the stages of the research. However 94 aged people participated in the first stage (hospital information), and 30 aged people participated in the second stage (interviews).
The collection of information was performed in three stages: 1) collection of hospital information; 2) carrying out of interviews about the situation where the fall/ femoral fracture occurred; 3) application of the short version of the Geriatric Depression Scale (GDS-15) of Yesavage, Brink, & Rose (1983).
First stage: collection of hospital information
In the first stage, the hospital information of the elderly people who had a femoral fracture in the period of one year was collected. In order to do so, the SMS made contact with two reference hospitals in care for the elderly in the municipality of study, and requested, via letter, the spreadsheets of information about the birth date, procedures conducted in the hospital, date of admission in the hospital, date of hospital discharge, International Classification of Diseases (ICD), costs of internment and address of residence.
A contact was made with the person responsible for the Technical Area of Health of the Elderly and requested authorization for the access to data. Through consent, the addresses were identified and the health units of the elderly by means of the Outpatient Information System (SIAL) of the SMS. In this stage, information about 94 elderly people who were hospitalized for femoral fracture in the period of one year was obtained. Among the 94 aged people of the first stage, 12 were excluded (four resided in rural areas/districts and eight died, according to the record of SIAL), for the second stage.
Second stage: carrying out of interviews about the situation where the fall/ femoral fracture occurred
For the carrying out of the interview, 82 home visits were made. The visits were made in the morning and the afternoon, during the week and also on Saturdays. The researchers used white coat and identification badge in all the visits. To find the addresses, since it is a medium-sized municipality, Google Maps and a Global Positioning System (GPS) device were used.
The first contact with the elderly was made in the residence door, when the researcher introduced herself and explained the aims of the research. As the elderly accepted to participate, they allowed the entrance to their home for the collection of data.
After the 82 home visits, it was observed that there was death (n = 24), change of address reported by the neighbors (n = 12), interview not authorized by the elderly's husband (n = 1), living in the asylum with no authorization from the institution for the interview (n = 1) and address not found (n = 14). Thus, the final sample was composed of 30 elderly people. There was a sample loss of 52 elderly people.
The 30 elderly people were interviewed, in this stage, about the situation where the fall/femoral fracture occurred. The interviews were carried out between 24 and 35 months after the internment of the elderly, with an average of 29.7 months and standard deviation of 3.3. This calculation was made based on the date of the internment of the elderly due to the unavailability of data about the date of the accident. However, it is estimated that the date of internment is very close to the occasion of the event.
A script with 17 open questions was elaborated by the researchers, presenting personal information, general data, and specific questions about the situations where the fracture occurred, seeking to identify the place, the causes and consequences that this event provoked in the life of the elderly, family and friends. It is important to note that the script of the interview was tested through the performing of a pilot study with three elderly people who suffered a femoral fracture from another municipality, to check the clarity of the instrument and whether the language level was adequate to the target population of the study.
Third stage: application of the short version of the Geriatric Depression Scale (GDS-15)
In the third stage, a short version of the Geriatric Depression Scale (GDS-15) of Yesavage, Brink and Rose (1983) was applied right after the interviews of the second stage, to identify the signs of depression among the elderly who suffered falls/femoral fracture. That scale is composed of 15 dichotomous questions with answers "yes" and "no," being attributed one point for yes and zero points for no.
According to Almeida & Almeida (1999), the short Geriatric Depression Scale is one of the most frequently used instruments to keep track of depression in elderly. Paradela, Lourenço, & Veras (2005) confirmed that this test allows keeping track of depressive symptoms in a geriatric individual, and it can be of great value in keeping track of an elderly individual with suspect of depression. This scale was validated by the last three authors, in a Brazilian outpatient geriatric population (similar to the target public of the work in question), being recommended to be applied in any other environment (hospitals, homes, long-stay institutions and basic healthcare). Thus, the instrument becomes valid to keep track of depressive signs in Brazilian elderly people.
Data analysis
The data analysis was carried out quantitatively and qualitatively, in a complementary way, to understand the reality studied better.
In the quantitative analysis, the most prevalent data were presented, and in the qualitative one, the cuttings of the participants' speeches. On the other hand, the answers to the depression test were analyzed quantitatively, summing up the negative answers obtained in the application of the instrument of 15 questions.
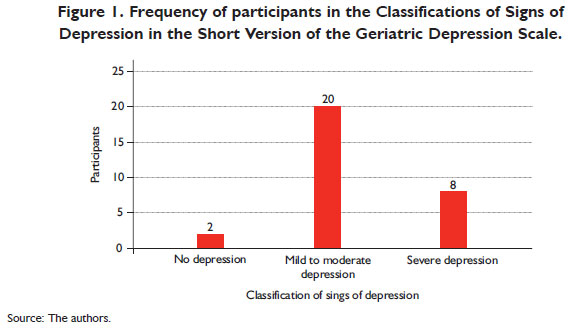
For the classification of the suspect of depression, the guidelines presented by Almeida & Almeida (1999) and by Paradela, Lourenço, & Veras (2005) were adopted, that is to say, each participant had the answers to the 15 questions analyzed individually. When we observed the quantity of up to four negative answers, the participant was classified as "no depression"; between 5 and 10 negative answers, as "mild to moderate depression"; and above 10 negative points, as "severe depression."
Results
Concerning the hospital information
The hospital internment data revealed that in the period of one year, 94 elderly people were interned for a femoral fracture in the two hospitals of the municipality, being 18 elderly people in Hospital 1 and 76 elderly people in Hospital 2. The minimum age of the elderly was 62 years old, and the maximum was 98 years old, with an average of 64 years old. The elderly investigated were interned in Hospital 1 between 3 and 19 days, with an average of 8.4 days of internment. In Hospital 2, they were interned between 1 and 81 days, with an average time of internment to 8.33 days. The hospital internments for a femoral fracture use to create a high cost for the municipality, that is to say, in the period of one year, amounts equivalent of 65 minimum wages were invested in a hospital, and 218 wages in the other one, which is equivalent to an average cost of three wages for each elderly person interned.
Concerning the data of the interview about the fall/femoral fracture
The sample investigated showed that most of the participants were females (80%). Concerning the marital status, one of them was single, three were married, three were divorced, nine widowed, and 14 separated. When they fractured the leg, 20 elderly people were in their own house, four were on the street, two were at work, and two were at a grandchild's house. Moreover, an aged woman fell on the shuttle bus and another one on the escalator of the Bus Station Barra Funda, in São Paulo.
Concerning the home environment, most of them fell in the backyard (n = 4), in the bedroom (n = 4) and on the street (n = 3). For instance, a lady was hanging clothes on the clothesline and slipped on the water that was dropping. Even in pain, she crawled and reached an iron gate and continuously knocked, until a child heard the noise and went to see what was happening. She passed the key underneath the gate and asked him to call for someone to help her. After this situation, the old lady went to live in a cottage behind her daughter's house, but she said she preferred to be in her own home.
A total of 15 elderly people informed that there was someone next to them in the moment of the fall, especially children (n = 6), grandchildren (n = 2), wife (n = 1) and even another aged person (n = 1). The elderly people were taken to the hospital by the Mobile Emergency Medical Services - SAMU 192 (n = 17) and by their own relatives (children: n = 4; grandchildren: n = 3). What caused a stir was the fact that an aged woman went to the hospital by herself. She said she fell and fractured her leg, but first she went to inform the old lady to whom she provided care. "You know, we must account." Subsequently, she took the shuttle bus and went to the hospital by herself. During this period of stay in the environment of the hospital, the lady lost seventeen kilos, and reckoned that it was a sad period, of suffering and pain. Besides, she could not work, and no income to pay her debts, and it let her "nervous and depressive."
Eight elderly people mentioned that they had felt pain during the hospital internment. They informed that in the hospital the nurses raised the fractured leg, causing unbearable pain. They could not sleep because of so much pain and constantly asked the hospital staff to give them medicine that could relieve it. An aged man commented that in that period of internment he had hallucinations, he saw the roof falling on him, and people walking on the walls of the room. About the recovering after the hospital internment, eight elderly people informed that it was good, and seven of them said they had much pain. The elderly people who evaluated positively referred that being at home (even in pain) was better than in the hospital: "it cannot be compared." Those who pointed out negative feelings reported that they could not do their personal hygiene and depended on other people to do it, especially their family (grandchildren, children, siblings, daughters-in-law, mother, etc.).
Among the 30 elderly people who participated, 20 informed that their friends did not help in the care. They were old friends (20 to 30 years) who did not support them in anything. They reported that "those people were friends only while they were healthy" and that "in the moment when they needed the most, the friends were not present." All of them informed that there were changes in their social activities. Most of them (n = 24) stopped leaving home not to give their children a hard time, because, in their opinion, walking with a walker disturbs the family routine. They prefer to stay home instead of asking for physical support.
Concerning the use of medicine, 20 elderly people informed that they used it before the fracture, and this number increased to 24 elderly people after the fall. They received, most of the times, medical follow-up in specialized services (Physiotherapy, Neurology and Geriatrics) and family medical doctors. The elderly people informed that the fracture could have been prevented if they had had more attention and more care. Moreover, one of them said that she should not have climbed the sofa to take clothes from the clothesline.
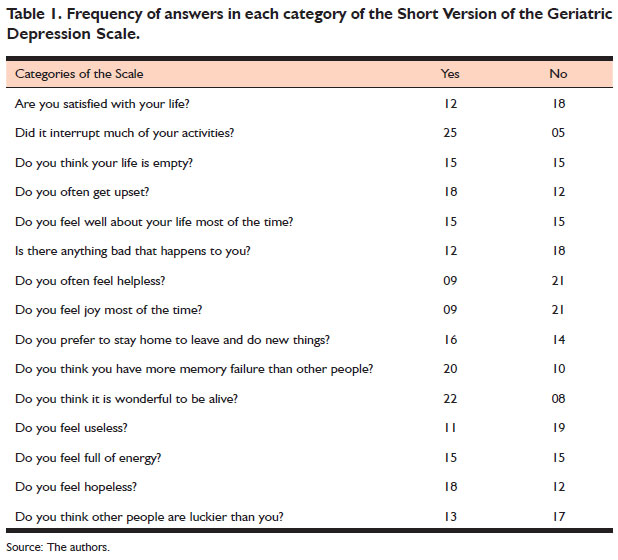
Concerning the data from the Short Version of the Geriatric Depression Scale (GDS-15)
The frequency of answers in each category of the Short Geriatric Depression Scale is shown in Table 1.
Most of the participants referred that they were not satisfied with life after the fall, because they stopped doing many things they used to do because of it. They informed that they worked their whole life and, in that moment, they were in a situation of dependence on others for everything, even personal hygiene. Moreover, some of them started bathing sitting on a chair, other stopped doing simple actions that they were used to doing like, for instance, going to the stove and putting their own meals. They said that the leg became shorter than the other one, and that this "defect" made walking hard, making life harder: "if I have to live depending on others, God had better revise my life on earth".
A good deal of the elderly people said they did not leave home anymore, fearing to fall and go through everything again in the hospital. After surgery, they needed to keep the stitches for fifteen days, and the cut opened while bathing, so they had to go back to the hospital and repeat the procedure. According to some elderly people, "it was a big suffering" having to go back to the surgical center.
The elderly people said that life became empty after the femoral fracture, because they "were useless." With the fall, "everything was over, because they could not even walk well." Others said that "being alive was really a miracle."
After the fracture they reported that they live with much pain and they cannot walk normally, needing a walker to be able to get around. When they were asked if they felt well about life most of the time, they said they did not, as they stopped doing many things they used to do. With the femoral fracture, their lives changed completely, and that change was to worse, because they could not leave home and go to the bank to withdraw their retirement pension anymore. They said they had worked their whole life and now they have to depend on others, that they could not put their feet on the ground and walk like a normal person. All of this let them distressed.
The other ones said it is hard and, sometimes, they caught themselves wondering about the life they had before the fall. They were upset, cried, and sometimes quarreled with anyone who was near them, but soon after that they "thanked God for being alive." Many elderly people feared that something bad could happen to them and many of them said they did not have joy most of the time. They justified that there was no joy because they could not do the simple actions they always did, like bathing by themselves, prepare their meals, withdraw their pension, go shopping, go to church, and work to complement the family income. Most of them often felt helpless, because they had to change their habits, left their homes to live with other people, or their relatives moved to their houses.
Thus, many of them preferred to stay home to do new things, because whenever they had to leave home they had to ask for help to get around. Others said that they had more memory failure than other people, that they had been very tired of coping with life, and that age contributes for that. They informed that in the hospital they felt pain and went through situations of hunger, fear, distress, sadness and neglect from some health professionals. The elderly referred lack of energy to do activities and loss of hope in life, once they stopped walking.
The frequency of participants in the Classification of Signs of Depression in the Geriatric Depression Scale of Yesavage - Short Version (GDS-15) is represented in Figure 1.
Discussion
The quantitative data from the hospitals allowed verifying that the femoral fracture occurred mainly among the female population (80%), being larger than the percentage found in the literature. Research conducted by Martini, Guerra, Mendes, & Echevest (2012) identified involvement in 68% of women. A study by Matias, Fonseca, & Matos (2015) verified in 60.3% of the female population. New investigations are necessary to evaluate this variable to check if this is a loco regional characteristic or if the female population is becoming more and more vulnerable to this kind of injury.
Another factor that must be highlighted is the age of the elderly, because in this study the average was of 62 years old, and in the research of Martini, Guerra, Mendes, & Echevest (2012) it was 78 years old, and in Matias, Fonseca, & Matos (2015) it was 73.1 years old, so it hypothesizes that the accidents can be earlier in this cycle of life. The situations of risk were more evident in the elderly's home and in the surroundings, corroborating with the study of Jahana & Diogo (2007), where most of the accidents occurred at home or near it. Literature confirms that the home environment presents risky situations to aged people, and among them are the presence of unstable pieces of furniture, inclined staircases or with no handrail, ramps or steps, loose carpets, inadequate illumination, slippery floor, presence of pets, use of slippers or shoes in bad conditions or inadequate, and loose electric wires (Yamazaki & Ferreira, 2013).
Considering that it is possible to make little changes in the risky situations in the residences, it is suggested the implantation of municipal public policies by the Secretariat of Health of the municipality in study, in the sense of promoting actions of prevention of accidents among the elderly. These actions could be carried out by the basic health units, especially by the community agents, who make frequent home visits in the territory. It would be desirable that the specialized services of rehabilitation (Physiotherapy, Neurology and Geriatrics), quoted by the participants of this study also carried out actions of prevention in the elderly people's homes. This study allowed identifying, in addition, risky situations in public areas of wide circulation of people, like streets, sidewalks and bus stations, so it can draw the attention of professionals of urban planning to projects of recovering of these places. According to Menezes & Bachion (2008), the improvement in the illumination of streets is indicated as a possible action. Besides, the review of projects of urban accessibility could contemplate all these requirements and, thus, promote safer public environments, especially for the elderly population.
Far beyond this, the qualitative information obtained through the interviews revealed that the social and emotional damage was impacting in these elderly people's lives, as it changed their routine and the relationship of family and friends towards the person who suffered the injury. The data of the interview show narrow connection to the results of the Geriatric Depression Scale (GDS-15) of Yesavage, Brink, & Rose (1983), especially in the interruption of the daily activities. Interrupting daily actions and depending on relatives to do routine activities were frequently mentioned by the elderly participant. This situation contributes to the presence of depression in aged people, according to the study performed in Bagé, Rio Grande do Sul, Brazil, when the Geriatric Depression Scale was applied to 1,593 people older than 60 years old (Bretanha et al., 2015). It is highlighted that in this study 93% of the participants presented signs of depression varying from mild to severe, and it can be considered a high rate, compared to the results found in Vitória da Conquista (48.7%) (Matias, Fonseca, & Matos, 2015) and in Taiwan (1.2%) (Chang et al., 2014), referring to the elderly who had a femoral fracture.
Taking as a basis the classification of Lopes & Dias (2010), the psychosocial consequence that was most present in the speech of the elderly who participated in this research was the fear of falling, corroborating to the study of Ribeiro, Souza, Atie, Souza, & Schilithz (2008) that revealed that most of the elderly people started to fear falling again after the fall. In interviews conducted with 72 elderly people from the municipality of Rio de Janeiro who fell, it was also verified that most of them started to fear, and others abandoned the habitual activities. Besides, there was difficulty to sleep and the feeling of sadness, contributing to the presence of depressive symptoms (Ribeiro, Souza, Atie, Souza, & Schilithz, 2008).
In this work, the interviews were conducted between 24 and 35 months after the internment of the elderly. The literature reveals that the depressive signs are frequently identified in the first 200 days, but they still can be noticed in the first three years after the fracture (Chang et al., 2014). The screening done in this study is within the time preconized by the literature, but nonetheless it is suggested the carrying out of new longitudinal studies to check whether the signs of depression improve or disappear with the time.
It is possible to state that the study reached the aim proposed, that is to say, it demonstrated that there are signs of depression in the elderly who suffered femoral fractures after falling, especially depressive humor. Once it is an exploratory and descriptive study, there was no purpose of carrying out a correlational analysis, being this kind of study suggestive to future research, including with the investigation of the cause of death, confrontation with epidemiologic data and data collection with the health services involved. Also, the results of this work cannot be generalized to other municipalities, because each one has a different epidemiologic characteristic and human development index, but it can encourage the carrying out of other works of collection of data and, preferably, of intervention, in partnership with universities or even public health services.
The high rates of morbimortality after femoral fracture identified in this study suggests the carrying out of actions of intervention by the health system, once the literature reveals that the elderly people who fell became more prone to a new accident (Berg1 et al., 2009) and that, when added to the signs of depression, increases the risk of death (Mesquita et al., 2009). For the elderly who presented the signs of depression, it is suggested to involve the psychologists of the municipal network of health in the elaboration of therapeutic projects which can relieve the depressive signs. The scientific evidence showed that the Cognitive-Behavioral Psychotherapy (CBT) was successful in the reduction of the symptomatology of depression after seven sessions of psychotherapy (Lobo et al., 2012).
The systematization of the results of this work allowed a discussion with the Department of Basic Care and with the technical areas of Elderly Health and Mental Health of the municipality, causing the implantation of municipal public policies of prevention of falls among the elderly, especially in the ages of more risk, to avoid negative consequences due to these episodes, especially signs of depression. New studies are necessary to investigate what this and other municipalities are doing in this sense, what actions were planned and which ones are being carried out, as well as the partners involved and the results obtained. Besides, even the literature having signaled the prevalence of deaths after the fall, it is fundamental to investigate whether the fracture was responsible separately for the signs of depression or what other comorbidities contributed to the death of the elderly. It is also suggested to check the progressive history of psychiatric symptoms among the elderly people and their relatives, to correlate to the depressive signs identified after the femoral fracture, these limitations being found in this study.
References
Alencar, N. A., Bezerra, J. C. P., & Dantas, E. H. M. (2009). Avaliação dos níveis de atividade física, autonomia funcional e qualidade de vida de idosas integrantes do programa saúde da família. Fitness Perfomance Journal, 8(5),315-321. doi:10. 3900/fpj.8.5.315.p [ Links ]
Almeida, O. P., & Almeida, S. A. (1999). Confiabilidade da versão brasileira da Escala de Depressão em Geriatria (GDS) versão reduzida. Arquivos de Neuro-Psiquiatria, 57(2B),421-426. doi:10.1590/S0004-282X1999000300013 [ Links ]
Berg1, M. V. D., Verdijk, N. A., Leusink, G. L., Gent, C. J. M. W., Romeijnders, A. C., Pop, V. J. M., & Bergh, J. P. W. V. D. (2011). Depression after low-energy fracture in older women predicts future falls: a prospective observational study. BMC Geriatrics, 11(73). doi:10.1186/1471-2318-11-73 [ Links ]
Borges, M. G. S., Rocha, L. R., Couto, E. A. B., & Mancini, P. C. (2013). Comparação do equilíbrio, depressão e cognição entre idosas institucionalizadas e não-institucionalizadas. Revista CEFAC, 15(5),1073-1079. doi:10.1590/S1516-18462013000 500003 [ Links ]
Bretanha, A. F., Facchini, L. A., Nunes, B. P., Munhoz, T. N., Tomasi, E., & Thumé, E. (2015). Sintomas depressivos em idosos residentes em áreas de abrangência das unidades básicas de saúde da zona urbana de Bagé, RS. Revista Brasileira de Epidemiologia, 18(1),1-12. doi:10.1590/1980-5497201500010001 [ Links ]
Chang, C. Y., Chen, W. L., Liou, Y. F., Ke, C. C., Lee, H. C., Huang, H. L., Ciou, L. P., Chou, C. C., Yangl, M. C., Ho, S. Y., & Lin, Y. R. (2014). Increased risk of major depression in the three years following a femoral neck fracture - a national population-based follow-up study. Plos One, 9(3),1-8. eCollection 2014. doi:10.13 71/journal.pone.0089867 [ Links ]
Cunha, U., & Veado, M. A. C. (2006). Fratura da extremidade proximal do fêmur em idosos: independência funcional e mortalidade em um ano. Revista Brasileira de Ortopedia, 41(6),195-199. [ Links ]
Daniachi, D., Santos Netto, A., Ono, N. K., Guimarães, R. P., Polesello, G. C., & Honda, E. Y. (2015). Epidemiology of fractures of the proximal third of the fêmur in eldely patients. Revista Brasileira de Ortopedia, 50(4),371-377. doi:10.1016/j.rboe. 2015.06.007 [ Links ]
Jahana, K. O., & Diogo, M. J. E. (2007) Quedas em idosos: principais causas e consequências. Saúde Coletiva, 4(17),148-153. [ Links ]
Lobo, B., Rigoli, M. M., Sbardelloto, G., Rinaldi, J., Argimon, I. L., & Kristensen, C. H. (2012). Terapia cognitivo-comportamental em grupo para idosos com sintomas de ansiedade e depressão: resultados preliminares. Psicologia: Teoria e Prática, 14(2),116-125. [ Links ]
Lopes R. A., & Dias, R. C. (2010). O impacto das quedas na qualidade de vida dos idosos. ConScientiae Saúde, 9(3),504-509. [ Links ]
Martini, F. P., Guerra, M. T. E., Mendes, M. R., & Echevest, S. S. (2012) Estudo epidemiológico das fraturas de fêmur proximal em Canoas no ano de 2010. Revista da AMRIGS 56(4),320-324. [ Links ]
Matias, A. G. C., Fonseca, M. A., & Matos, M. A. A. (2015). Análise fatorial de sintomas depressivos e ocorrência de quedas em idosos. Scientia Medica, 25(1),2-8. doi:10.15448/1980-6108.2015.1.19804 [ Links ]
Menezes, R. L., & Bachion, M. M. (2008). Estudo da presença de fatores de risco intrínsecos para quedas em idosos institucionalizados. Ciência e Saúde Coletiva, 13(4),1209-1218. doi:10.1590/S1413-81232008000400017 [ Links ]
Mentis, M., Gouva, M., Antoniadou, E., Mpourdoulis, K., Kesoudidou, I., Marneras, C., & Panagiotopoulos, E. (2017). Psychological and physical problems in elderly people with problems of falls. European Psychiatry, 41(suppl.),S659-S660. doi:10.1016/j.eurpsy.2017.01.1112 [ Links ]
Mesquita, G. V., Lima, M. A. L. T. A., Santos, A. M. R., Alves, E. L. M., Brito, J. N. P. O., & Martins, M. C. C. (2009). Morbimortalidade em idosos por fratura proximal do fêmur. Texto e Contexto Enfermagem, 18(1),67-73. [ Links ]
Paradela, E. M. P., Lourenço, R. A., & Veras, R. P. (2005). Validação da escala de depressão geriátrica em um ambulatório geral. Revista de Saúde Pública, 39(6),918-923. doi:10.1590/S0034-89102005000600008 [ Links ]
Ribeiro, A. P., Souza, E. R., Atie, S., Souza, A. C., & Schilithz, A. O. (2008). A influência das quedas na qualidade de vida de idosos. Ciência & Saúde Coletiva, 13(4),1265-1273. [ Links ]
Rodrigues, G. D., Barbeito, A. B., & Alves Junior, E. D. (2016). Prevenção de quedas no idoso: revisão da literatura brasileira. RBPFEX - Revista Brasileira de Prescrição e Fisiologia do Exercício, 10(59),431-437. doi:10.1590/S1413-81232008000400023 [ Links ]
Yamazaki, A. L. S., & Ferreira, E. G. (2013). Identificação dos fatores de risco relacionados à queda em idosos inseridos na estratégia saúde da família. Revista Saúde e Pesquisa, 6(1),93-98. [ Links ]
Yesavage, J. A., Brink, T. L., Rose, T. L., Lum, O., Huang, V., Adey, M., & Leirer, V. O. (1983). Development and validation of a geriatric depression screening scale: a preliminary report. Journal of Psychiatric Research, 17(1),37-49. doi:10.1016/00223956(82)90033-4 [ Links ]
 Mailling address:
Mailling address:
Rosana Fortunato Modesto
Rua Lucia Aparecida Tonon Rodrigues, 139, Bairro Jardim Brasil, Garça
São Paulo, SP, Brazil. CEP
E-mail: rosana_psique@hotmail.com
Submission: 2.23.17
Acceptance: 3.27.18

{kind=link}