










Servicios Personalizados
Revista

Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores
Compartir

 Permalink
PermalinkJournal of Human Growth and Development
versión impresa ISSN 0104-1282versión On-line ISSN 2175-3598
J. Hum. Growth Dev. vol.29 no.3 São Paulo sept./dic. 2019
https://doi.org/10.7322/jhgd.v29.9541
ORIGINAL ARTICLE
Leprosy and Physiotherapy: a necessary approach
Cláudia Cecília de Souza Álvarez; Günter Hans Filho
Programa de Pós-graduação em Doenças Infecciosas e Parasitárias, Federal University of Mato Grosso do Sul (UFMS) - Campo Grande (MS), Brasil
ABSTRACT
INTRODUCTION: New cases of leprosy occur due to a set of factors associated with the lack of knowledge about the disease, both by health professionals and patients, favoring late diagnosis, the development of physical and social disabilities, stigma and prejudice.
OBJECTIVE: To verify the knowledge of students completing the physiotherapy course on leprosy and professional practice in the care of patients with the disease.
METHODS: A qualitative exploratory descriptive study was conducted with 68 undergraduate students from physiotherapy courses from public and private universities (AU, UB, UC), in the State of Mato Grosso do Sul. Data were collected through a questionnaire with ten open questions about knowledge, practical action, motivations, interests and teaching-learning process about leprosy. To organize and analyze the data, the collective subject discourse technique was used.
RESULTS: It was found that 60% of aU students, 63% of UB and 30.8% of UC have a general conception about the disease. 46.7% of aU students, 77.8% of UB and 80.9% of UC never had contact with leprosy patients. More than half of the students at the three universities said they were unaware of the physiotherapy approaches and practices in leprosy. Almost 100% of ub and UC students stated that the subject was not addressed during the course and therefore did not feel prepared to provide health education and to guide on how to prevent physical deficiencies resulting from leprosy. 73.3% of AU students, 96.3% of UB and 100% of UC recorded negative evaluations, qualifying the course as precarious, insufficient and weak in the leprosy approach.
CONCLUSION: It is concluded that leprosy should be included in physiotherapy courses systematically, providing practical care activities, developing skills from prevention to rehabilitation, seeking greater motivation and identification of his work in this area.
Keywords: higher education, learning, professional practice, leprosy, physiotherapy.
INTRODUCTION
More than 16 million patients throughout the world have been treated for leprosy in the last 20 years, with 211,973 new cases occurring in 2015, accounting for 2.9 new cases per 10,000 people. These new cases indicate the transmission continuity of the disease, of which 94% were registered in only 13 countries (Bangladesh, Brazil, Democratic Republic of Congo, Ethiopia, India, Indonesia, Madagascar, Myanmar, Nepal, Nigeria, Philippines, Sri Lanka And the United Republic of Tanzania)1. Thus, the World Health Organisation has launched the Global Leprosy Strategy 2016-2020, with the intention of eliminating leprosy from the world by increasing knowledgeable teams and focusing on three pillars: government ownership, coordination and partnership, an end to leprosy and its complications, and the cessation of discrimination and the promotion of inclusion.
Leprosy is a compulsorily notifiable disease in Brazil, with the highest detection rates in the central-west, north and northeast regions of the country. In 2015, there were 28,761 new cases (13.6% of global cases), placing Brazil in second place in the world. The main concern is the existing active transmission circuit2, with 7.3% of national cases occurring in young people under 15 years of age, representing a detection coefficient of 4.88 per 100,000 people in this age group (considered high index).
New leprosy cases occur due to a set of factors connected to a lack of knowledge of the disease, both by health professionals and patients. Several physicians have no knowledge of the transmission mechanisms of leprosy, and encourage patient behaviours that increase the negative stigma of the disease3. Leprosy study participants (42% of them) reported that physicians had not diagnosed them primarily with the disease, confusing it with rheumatism and skin allergies4.
Besides the difficulty of obtaining a rapid diagnosis, it is common for patients to discontinue treatment and to be unaware of the symptoms of the disease. Leprosy is not approached with a singular language that is understandable to people who do not have complete schooling, thereby impairing the continuity of treatment and the identification of disease symptoms5. Moreover, most professionals are not able to deal with the psychological aspects of these patients, who require a sensitive approach to the experience of suffering and the stigma associated with leprosy6.
Physiotherapist intervention is essential for a physical and functional evaluation and for the prevention or minimisation of physical disabilities7, considering that many patients have disabilities during the diagnosis phase or develop them during leprosy treatment. These disabilities have a major impact on the patient's social and work life, largely because of the emotional distress associated with the illness. Thus, this study aimed to assess knowledge about leprosy and the professional performance of physiotherapy graduating students at public and private universities.
METHODS
This was a qualitative exploratory descriptive study, carried out at three universities (UA, UB, UC) in the state of Mato Grosso do Sul (Brazil). All students (n = 68) attended the last year of a physiotherapy course, with 22% (15) at UA, 39.7% (27) at UB and 38.3% (26) at UC.
To evaluate the students, a self-administered questionnaire was used, based on the script developed by Dias, Cyrino and Lastória8, composed of ten open questions related to knowledge, practical action, motivations, interests and the teaching-learning process with regard to leprosy.
Data was collected in a single meeting, in the classroom of each university, between May 2014 and March 2015, and no member had access to the evaluation before the scheduled date. The researcher read the Informed Free Consent Term to the students, which clarified the purpose of the research, and supervised them during the evaluation. The questionnaire was answered individually, without consulting digital or printed sources. All participants signed a free and informed consent form.
To organise data and analysis, the collective subject discourse (CSD) technique was used, as this was developed for the qualitative analysis of social opinion surveys. This methodology seeks discursiveness, inseparable characteristics of collective thought and presents the results in a qualitative and quantitative way, expressed as the perception of collectivity from individual testimonials9.
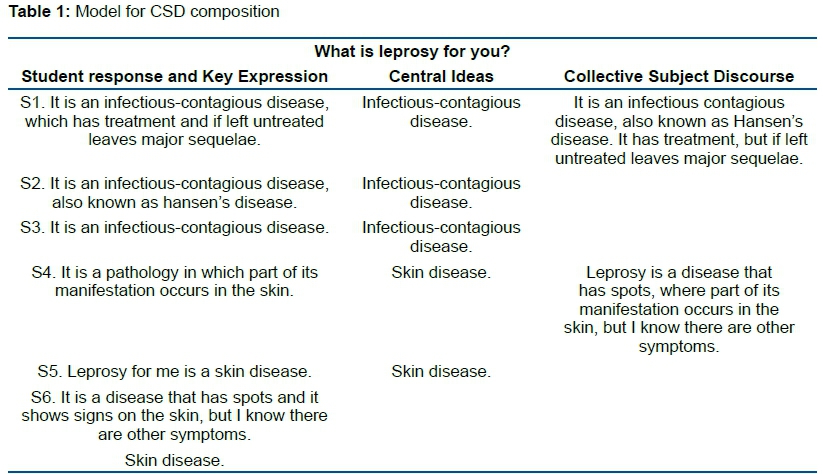
CSD selects the key expression (KE) from each response, formed by the most important passages, which are literal transcriptions that reveal the essence of the testimony and which best answer the questions. KE correspond to central ideas (CI), which may be a name or an expression that accurately describes the meaning of each statement. Thus, the discourse-synthesis is constructed, i.e. KE that have similar or complementary CI. The discourse is written in the first singular person, in which the idea of a group presents itself as an individual discourse (Table 1).
This study was submitted and approved by Ethics and Research Committee of the Federal University of Mato Grosso do Sul (document nº. 159,139).
RESULTS
The results are presented according to categories and frequencies, separating the CIs and the discourses by university.
The three universities did not present specific classes and times for the leprosy study, as the general aspects of the disease were mentioned in classes including Community Health, Microbiology, Pathology and Neurology (peripheral lesions).
Leprosy - conception of the disease, contact and reasons for preconception
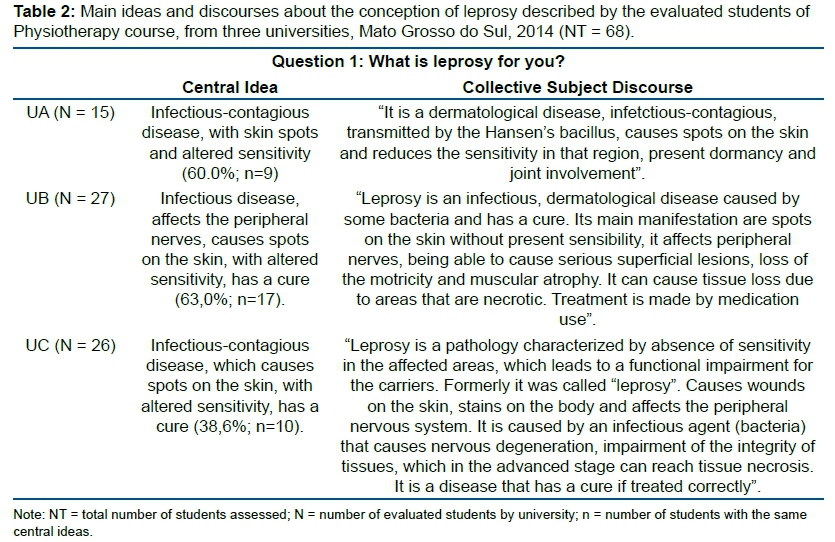
Question 1: What is leprosy for you? - 60% (9) of UA, 63% (17) of UB and 30.8% (8) of UC had a general conception about the disease. Students answered that it is an infectious-contagious disease that affects the peripheral nerves, causes skin spots and presents as an alteration in sensitivity (Table 2).
13.4% (2) of UA, 22.2% of UB (6) and 19.1% (5) of UC did not know the disease, indicating it as: 'an autoimmune disease that causes a skin stain', 'caused by a virus', 'animal disease transmitted by animals', ' non-contagious, and has no cure, only treatment'.
Question 2: Have you ever had contact with a leprosy patient? Where and how was it? - 46.7% (7) of UA students, 77.8% (21) of UB and 80.9% (21) of UC had never had contact with leprosy patients. However, 53.3% (8) of UA mentioned contact with patients during the course, through visiting a hospital or during a curricular traineeship in a polyclinic or public health unit. Some testimonies showed a lack of knowledge about the disease and insecurity: 'Yes, at the public health unit, during the stage, the patient had a lot of sequelae. It was worrisome because we did not have personal protective equipment and the patient had several skin lesions and we were not certain if it was treated or cured'. Others felt safe because they were sure that the patient was already on treatment. At UB and UC, contact occurred during hospital visits, extracurricular activities and in the subjects' personal lives.
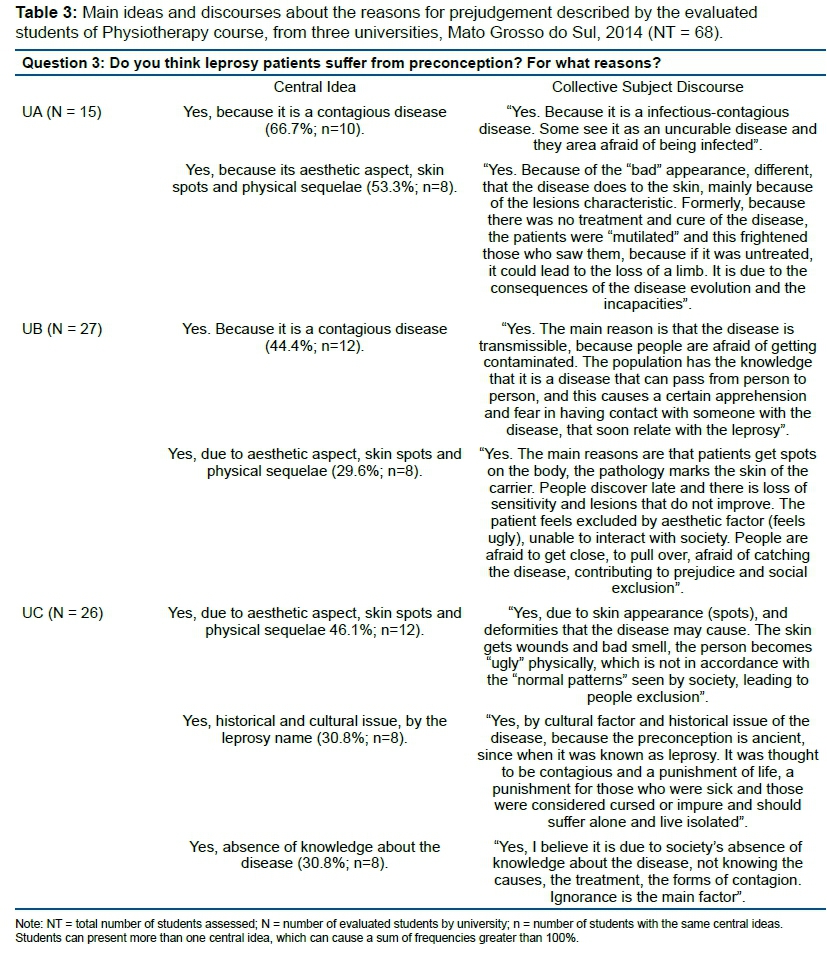
Question 3: Do you think leprosy patients suffer from preconception? For what reasons? - 100% (68) of the students said yes. The main reasons for UA and UB were the contagious characteristic of the disease and the physical stains and sequelae. For UC, the main reasons were the aesthetic aspect, lack of knowledge about the disease and the historical factors associated with leprosy (Table 3).
Physical incapacity evaluation, performance and physical therapy
Question 4: What are the items that should be addressed in a physical therapy assessment to determine the degree of physical disability in a leprosy patient? - 66.7% (18) of UB and 30.8% (8) of UC declared they did not know. 100% (15) of UA, 22.2% (6) of UB and 53.8% (14) of UC mentioned three to five basic items of a physical therapy assessment: inspection, palpation, goniometry, sensory evaluation and muscular strength.
Question 5: What services can a physiotherapist provide for a leprosy patient? - 59.3% (16) of UB students and 61.5% (16) of UC indicated they did not know; however, 53.3% (8) of UA indicated some aspects of professional performance: evaluation and prevention of deformities, health promotion, disease guidelines, treatment and reintegration of patients into society. The rest of the students mentioned treatment and rehabilitation items in general and insecure ways, demonstrating that they did not know the extent of actions and professional performance in the context of leprosy.
Question 6: What are the physiotherapeutic procedures that can be performed for a leprosy patient? - 85.2% (23) of UB students and 57.7% (15) of UC did not know how to respond. 60% (9) of UA, 7.4% (2) of UB and 19.2% (5) of UC mentioned at least four therapeutic approaches: exercises for muscle strengthening, range of motion improvement, stretching and sensory stimulation. Only UB (7.4%; 2) mentioned skin evaluations and ulcer care.
All students who failed to indicate the therapeutic approaches were insecure in responding, claiming that the topic was not addressed during the course.
Student perception - ability to care, leprosy teaching and learning interests
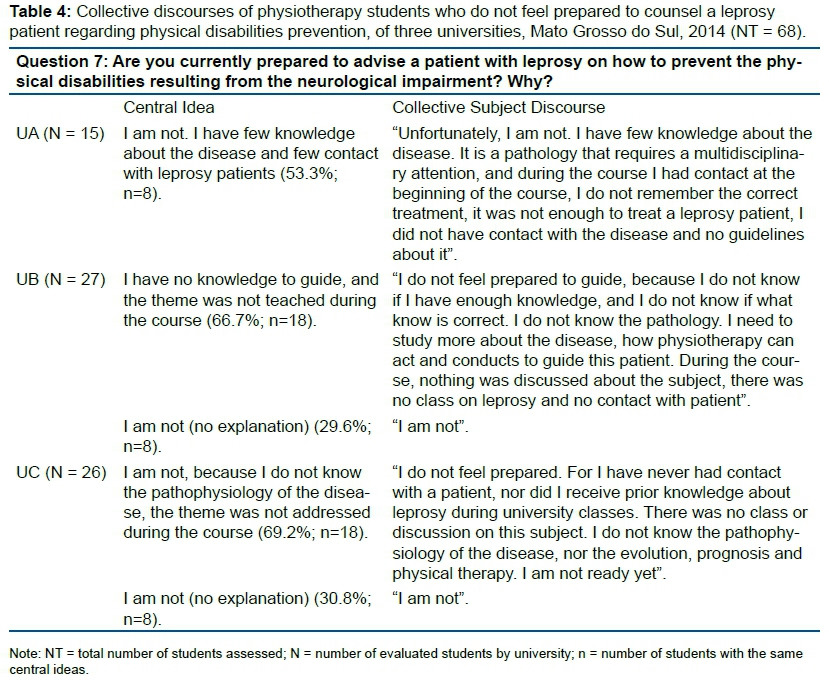
Question 7: Are you currently prepared to advise a patient with leprosy on how to prevent the physical disabilities resulting from neurological impairment? Why? - 53.3% (8) of UA students, 96.3% (26) of UB and 100% (26) of UC answered that they did not feel prepared due to insecurity, few or no contact with the patient, absence of theoretical and practical knowledge about the disease, lack of teaching on the course, lack of knowledge of physiotherapeutic practices for leprosy patients (Table 4).
Question 8: Are you currently prepared to provide health education to the patient, the communicator and the general public about leprosy? If not, what do you need to feel prepared to give these guidelines? - Similarly, 66.7% (10) of UA, 100% (27) of UB and 100% (26) of UC reported not being prepared to provide guidance due to a lack of knowledge about the disease (Table 5).
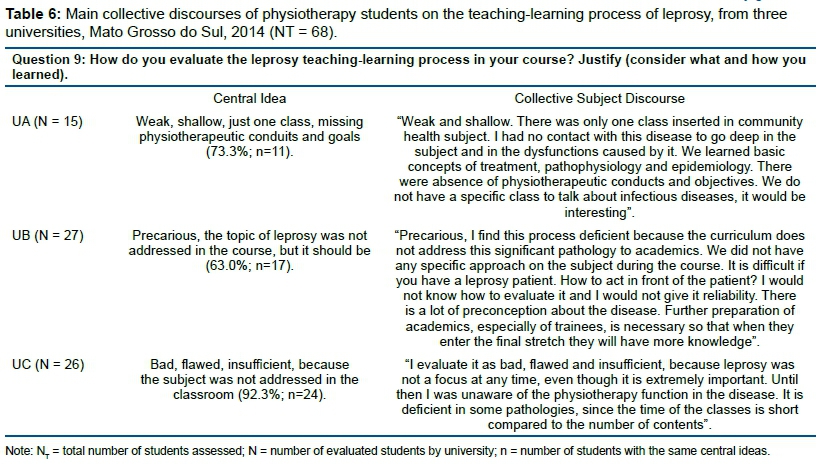
Question 9: How do you evaluate the leprosy teaching-learning process in your course? Justify (consider what and how you learned) - 73.3% (11) of UA, 96.3% (26) of UB and 100% (26) of UC registered negative evaluations, qualifying the course as precarious, weak, insufficient and poor (Table 6).
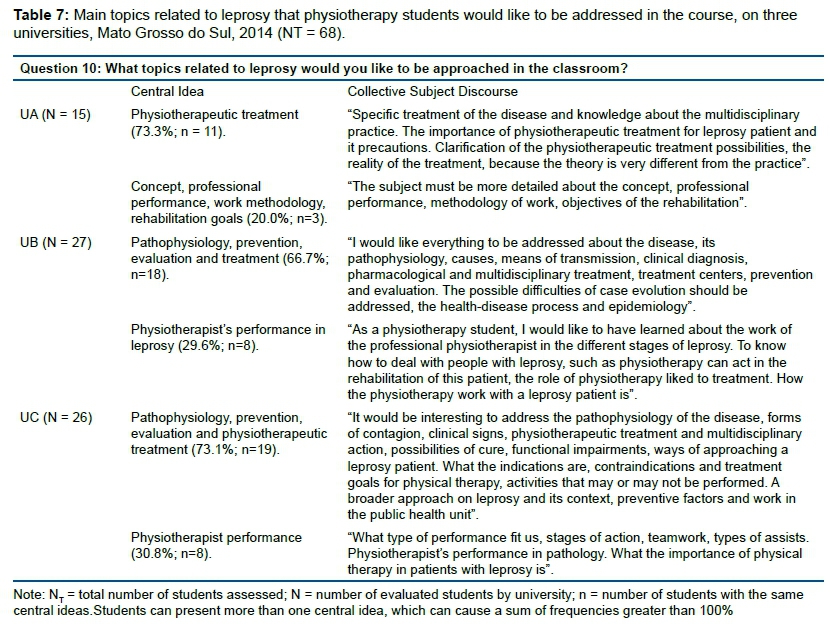
Question 10: What topics related to leprosy would you like to have approached in the classroom? - The three universities listed similar themes: physical therapy treatment and knowledge about multidisciplinary practice, pathophysiology, prevention, evaluation and treatment, physiotherapist performance, historical issues and breach of preconceptions, prevention programs and intervention projects about the disease and physiotherapy work with changes in post-leprosy sensitivity.
The topics of greatest interest were the pathophysiology of the disease, physical therapy evaluations and treatments, as well as physiotherapist performance (Table 7).
DISCUSSION
Leprosy - conception of the disease, contact and reasons for preconception
Leprosy is a notifiable disease, endemic in Brazil and still considered a public health problem, with a correlation between the disease population and social condition10,11. The later diagnosis and treatment, the more serious the physical and social disabilities of patients12,13. Stigma and preconceptions resulting from this disease remain in the popular imagination and are linked to the image of the body, because patients may have skin spots, lesions on the mucosa and physical deformities. The patient can also manifest feelings of sadness, worry, fear and isolation due to the possibility of suffering preconceptions and rejection in their social environment14,15.
Despite health campaigns and government actions, society is unaware of the disease and carries erroneous beliefs, fear and preconception. The existence of free and efficient treatment, with easy administration and a high cure rate, is not enough to eliminate stigma regarding this disease. The absence of clarification is commonly observed among those who should guide the population. Professionals who have not had adequate education in their training feel insecure in terms of attending to or touching leprosy patients, favouring behaviours that reinforce the stigma and preconception14,16,17.
It is imperative to discuss all aspects of the disease and to demystify leprosy among health professionals and students. This will allow them to feel safe and prepared to identify and diagnose the disease early, clarify doubts and reassure the patient about treatment and cure15,18-20.
Therefore, it is essential to contact the patient and the professional practice during the course, to develop skills and competencies and to undo erroneous ideas existing among health professionals. The design of new health practices requires an assessment of the training of professionals, who must be able to perceive the multi-causality of morbid processes and to visualise the individual in their environment.
Physical incapacity valuation, performance and physiotherapy conducts
It is not possible to say that students know the physiotherapeutic approach to leprosy, since some physical evaluation items were cited, but they were not related to the leprosy patient. Added to this, almost 100% of the students did not feel prepared to advise a leprosy patient, to prevent physical incapacities and to describe physical therapy, due to a lack of knowledge and a lack of content in the curriculum.
It is essential to perform a Disability Grade Assessment and Simplified Neurological Assessment at diagnosis and then every three months during treatment, whenever there are complaints (pain, paraesthesia and muscular weakness), in cases of leprosy reactions, at the end treatment and after post-neural decompression surgery. The disability degree indicates a loss of protective sensitivity and/or visible deformities as a result of neural damage and/or blindness, and is an epidemiological indicator used to evaluate programs, to provide an early diagnosis (the presence of a deformity indicates a late diagnosis), and to compare disability grades at the beginning of treatment and after treatment cessation10.
The Simplified Neurological Assessment checks the integrity of neural function, identifies neurites early, monitors responses to indicated treatment and determines the need for surgery. This involves a physical examination, with an inspection of the eyes, nose, neck, hands and feet, palpation of the peripheral nerves (ulnar, medial, radial, common fibular and posterior tibial), performing a sensitive sensory threshold test on hands and feet and a manual test of muscle strength assessing movement and the capacity to oppose gravity and manual resistance, in each muscular group referring to a specific nerve10,21,22.
Every health professional should be able to evaluate and identify any early dermatoneurological signs of leprosy, to guide and propose appropriate therapy and to avoid or minimise physical disabilities22,23.
Physical evaluation and monitoring a patient's clinical condition are essential for the preservation of nerve structure and function, identifying deficiencies and preventing future changes. The participation physiotherapy professionals in the clinical/functional diagnosis, treatment and discharge of the patient contributes to disability reduction, recovery of motor skills and avoids the progression of neural complications, all of which are essential for participation in a leprosy control program and in the professional team of a public health unit7,24-27.
The physiotherapist has general professional training, directed to integral care of the patient, and is able to act at all levels of health care. Their work regarding leprosy consists of patient and general population orientation and communication, the prevention of new cases, providing a functional diagnosis, evaluation, treatment and rehabilitation of physical disabilities and social reintegration8,28,29.
In the multidisciplinary team, after diagnosis, the physiotherapist classifies disability degree and monitors neural function, basing the therapeutic behaviours on information obtained in the neurological evaluation. The main approaches include conventional treatment with muscle strengthening and stretching exercises, passive or active mobilisation (assisted or not), proprioceptive neuromuscular facilitation (PNF); the neural mobilisation technique, electrothermophototherapeutic resources, hydration, lubrication and superficial massage of the skin, the development and adaptation of orthoses, splints and insoles as well as guidelines for self-care26,28,30-33.
Physical therapy in leprosy strengthens muscles, decreases and prevents contractures, recovers and maintains joint mobility, maintains tone, integrity and elasticity of skin and prevents deformities. In ulcers, physiotherapy stimulates the healing process, and in cases of surgeries for neural decompression and tendon transfer, it acts in the pre- and postoperative period, controls inflammation, pain, oedema and muscle spasms, maintains functional independence in the activities of daily life and guides the patient toward new patterns of movement post-transfer10,29,31,32.
The students who mentioned some type of physical therapy had the opportunity to experience contact with leprosy patients or related the treatment of other diseases with neuromuscular impairments and sensory and motor alterations that could be similar to leprosy. Therefore, it is necessary to teach leprosy and a directed approach on neurological physical and neurological evaluations, so that the future professional is capable of understanding and exercising its role as a transforming agent in health conditions8,21,34,35.
Learner perception - care, leprosy teaching and learning interests
Lack of knowledge of students and health professionals contribute directly to a late diagnosis, physical disabilities, situations of stigma and preconception and increase the number of infected individuals8,21,34.
These results demonstrated the need to approach leprosy in undergraduate physiotherapy courses, in order to train professionals to be able to contribute directly to the three levels of health care and to launch a new assessment at professional practices8,21,34,36. Due to the impact that a well-trained and qualified professional has on leprosy patient care, it is important to emphasise a greater search for motivation and identification of their work in this area.
Physiotherapist actions in the control and elimination of leprosy are important, but poorly explored. It is fundamental to review the curriculum of undergraduate courses in order to contemplate leprosy in theory and practice systematically, focusing on a physiotherapist's professional work, as well as encouraging students and teachers to discuss strategies and challenges in combating this disease.
CONCLUSION
The assessment of physiotherapy students' knowledge evidenced the absence of important knowledge to identify, evaluate, treat and guide the leprosy patient. Physiotherapist actions in the control and elimination of leprosy are important, but poorly explored. So, it is fundamental to review the curriculum of undergraduate courses in order to contemplate leprosy in theory and practice systematically, focusing on the physiotherapist's professional work, as well as encouraging students and teachers to discuss strategies and challenges in combating the disease. Due to the impact that a well-trained and qualified professional has on leprosy patient care, it is important to emphasise a greater search for motivation and identification of their work.
It is essential to contact the patient and ensure best professional practice on physiotherapy courses, to develop skills and competencies and to undo erroneous ideas existing among health professionals. It is suggested that, in hospitals and centres specialised in leprosy, partnerships should be established with higher education institutions in order to provide the student with practical experience in the care of patients with leprosy, as well as to stimulate research and innovations in physiotherapeutic activities.
Source(s) of support:
The research was funded by Coordination for the Improvement of Higher Education Personnel (CAPES).
REFERENCES
1.World Health Organization (WHO). Global leprosy strategy 2016-2020: accelerating towards a leprosy-free world. [cited 2017 Apr 4] Available from: http://www.searo.who.int/entity/global_leprosy_programme/documents/global_leprosy_strategy_2020/en/. [ Links ]
2.Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Coordenação-Geral de Desenvolvimento da Epidemiologia em Serviços. Guia de Vigilância em Saúde: recurso eletrônico. Brasília: Ministério da Saúde, 2016. [ Links ]
3.Sillo S, Lomax C, Wildt G, Fonseca MS, Galan NGA, Prado RBR. A temporal and sociocultural exploration of the stigma experiences of leprosy patients in Brazil. Lepr Rev. 2016;87(3):378-95. [ Links ]
4.Henry M, Galan N, Teasdale K, Prado R, Amar H, Rays MS, et al. Factors contributing to the delay in diagnosis and continued transmission of leprosy in Brazil - an explorative, quantitative, questionnaire based study. PLoS Negl Trop Dis. 2016;10(3):e0004542. DOI: https://doi.org/10.1371/journal.pntd.0004542 [ Links ]
5.Silva MCD, Paz EPA. Health education in the leprosy control program: the experience of the multidisciplinary team. Esc Anna Nery. 2010;14(2):223-9. DOI: http://dx.doi.org/10.1590/S141481452010000200003 [ Links ]
6.Nakae MF. Nada será como antes - o discurso do sujeito coletivo hanseniano. Psic. 2002;3(2):54-73. [ Links ]
7.Serrano-Coll H, Vélez JD, Trochez D, Beltrán JC, Suanca D, Monsalve F, et al. Effectiveness of an individual physical rehabilitation programme in a group of patients with Hansen's disease. Lepr Rev. 2016;87(3):355-67. [ Links ]
8.Dias A, Cyrino EG, Lastória JC. Knowledge and necessities of learning of physiotherapy's students about Leprosy. Hansen Int. 2007;32(1):9-18. [ Links ]
9.Lefèvre F, Lefèvre AMC. Discurso do sujeito coletivo: um novo enfoque em pesquisa qualitativa (desdobramentos). Porto Alegre: Educs, 2003. [ Links ]
10.Brasil Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Diretrizes para vigilância, atenção e eliminação da hanseníase como problema de saúde pública. Brasília: Ministério da Saúde, 2016. [ Links ]
11.Castro SS, Abreu GB, Fernandes LFRM, Santos JPP, Oliveira VR. Leprosy incidence, characterization of cases and correlation with household and cases variables of the Brazilian states in 2010. An Bras Dermatol. 2016; 91(1):28-33. DOI: http://dx.doi.org/10.1590/abd1806-4841.20164360 [ Links ]
12.Monteiro LD, Martins-Melo FR, Brito AL, Alencar CH, Heukelbach J. Physical disabilities at diagnosis of leprosy in a hyperendemic area of Brazil: trends and associated factors. Lepr Rev. 2015;86(3):240-50. [ Links ]
13.Lima AS, Pinto KC, Bona MPS, Mattos SML, Hoffmann MP, Mulinari-Brenner FA, et al. Leprosy in a University Hospital in Southern Brazil. An Bras Dermatol. 2015;90(5):654-9. DOI: http://dx.doi.org/10.1590/abd1806-4841.20153959 [ Links ]
14.Pellizzari VDZV, Arruda GO, Marcon SS, Fernandes CAM. Perceptions of people with leprosy about disease and treatment. Rev Rene. 2016; 17(4):466-74. DOI: https://doi.org/10.15253/2175-6783.2016000400005 [ Links ]
15.Silveira MGB, Coelho AR, Rodrigues SM, Soares MM, Camilo GN. Hansen's disease patients: psychological impact of the diagnosis. Psicol Soc. 2014;26(2):517-27. DOI: http://dx.doi.org/10.1590/S0102-71822014000200027 [ Links ]
16.Lana FCF, Lanza FM, Carvalho APM, Tavares APN. Stigma associated with hansen's disease and its relation to control actions. Rev Enferm UFSM. 2014;4(3):556-65. DOI: http://dx.doi.org/10.5902/2179769212550 [ Links ]
17.Teasdale K, Wildt G, Pranab K, Virmond Mda C, Galan NG, Prado RB, et al. The patient perspective of the diagnostic process for leprosy in Brazil. An exploratory study. Lepr Rev. 2015;86(1):21-36. [ Links ]
18.Santos DCM, Nascimento RD, Gregório VRN, Silva MRF. The Hansen's disease and its diagnostic process. Hansen Int. 2007;32(1):19-26. [ Links ]
19.Malviya GN. Disabilities in leprosy - the new concepts. Indian J Lepr. 2014; 86(3):121-7. [ Links ]
20.Sermrittirong S, Van Brakel WH. Stigma in leprosy: concepts, causes and determinants. Lepr Rev. 2014;85(1):36-47. [ Links ]
21.Lopes JP. Conhecimento de alunos sobre Hanseníase. Saúde Rev. 2016;16(42):1-10. DOI: http://dx.doi.org/10.15600/2238-1244/sr.v16n42p1-10 [ Links ]
22.Rodini FCB, Gonçalves M, Barros ARSB, Mazzer N, Elui VMC, Fonseca MCR. Disability prevention in leprosy using a self-care manual for patients. Fisioter Pesqui. 2010;17(2):157-66. DOI: http://dx.doi.org/10.1590/S1809-29502010000200012 [ Links ]
23.Véras LST, Vale RGS, Mello DB, Castro JAF, Lima V, Trott A, et al. Electromyography function, disability degree, and pain in leprosy patients undergoing neural mobilization treatment. Rev Soc Bras Med Trop. 2012;45(1):83-8. DOI: http://dx.doi.org/10.1590/S0037-86822012000100016 [ Links ]
24.Araujo AERA, Aquino DMC, Goulart IMB, Pereira SRF, Figueiredo IA, Serra HO, et al. Factors associated with neural alterations and physical disabilities in patients with leprosy in São Luis, State of Maranhão, Brazil. Rev Soc Bras Med Trop. 2014;47(4):490-7. DOI: http://dx.doi.org/10.1590/0037-8682-0119-2014 [ Links ]
25.Beluci ML, Borgato MH, Galan NGA. Evaluation of multidisciplinary courses in leprosy. Hansen Int. 2012;37(2):47-53. [ Links ]
26.Gonçalves SD, Sampaio RF, Antunes CMF. Predictive factors of disability in patients with leprosy. Rev Saúde Pública. 2009;43(2):267-74. DOI: http://dx.doi.org/10.1590/S0034-89102009000200007 [ Links ]
27.Caldas AM, Aquino DMC, Caldas AJM, Silva RSO, Silva SMF. Action of physical therapy multipurpose team in the monitoring of patients with leprosy. Rev Hosp Universitário UFMA. 2007;8(2):17-22. [ Links ]
28.Ferreira JLPM, Cerdeira DQ, Nunes TTV, Guimarães DF, Liberato FRC. Role of physical therapy in the follow-up of patients with leprosy. Fisioter Bras. 2016;17(5):472-79. [ Links ]
29.Brasil Serviço Público Federal. Conselho Regional de Fisioterapia e Terapia Ocupacional da 11ª Região - DF e GO. Protocolo de Fisioterapia e Terapia Ocupacional para prevenção de incapacidades físicas e reabilitação em hanseníase recomendado pelo Creffito 11. Brasília: 2015. [ Links ]
30.Oliveira JM, Torquato SG, Mello D, Dantas EHM. [Experience report on the use of low-power laser in the treatment of neurotrophic ulcers]. Rev enferm ufpe on line. 2014 May;8(5):1330-6. doi: 10.5205/reuol.5863-50531-1-ed.0805201430. Portuguese. [ Links ]
31.Xavier EM, Ferreira J, Raniero LJ, Batista JRX, Freitas MLL, Sousa M, et al. Wound healing leprosy induced by low intensity laser. Hansen Int. 2012;37(1):51-7. [ Links ]
32.Lima GM, Miranda MGR, Ferreira TCR. Action of therapeutic exercises in patients with chronic neuritis holders of leprosy, accompanied at the Reference Unit Specialized in Sanitary Dermatology Dr. Marcello Candia. Hansenol Int. 2009;34(1):9-16. [ Links ]
33.Diaz AF, Moro FL, Binotto JM, Fréz AR. Preliminary comparative study between proprioceptive and passive static stretching in patients with leprosy sequelae. Fisioter Pesqui. 2008;15(4):339-44. DOI: http://dx.doi.org/10.1590/S1809-29502008000400004 [ Links ]
34.Reis FJJ, Gomes MK, Alves D, Cabral R, Cunha AJLA. Leprosy: knowledge and social representations among physical therapy students. Fisioter Bras. 2014;15(3):178-83. [ Links ]
35.Kanodia SK, Dixit AM, Shukla SR, Seth AK, Balothia V, Gupta R. A study on knowledge, beliefs and attitude towards leprosy in students of Jaipur, Rajasthan. Indian J Lepr. 2012;84(4):277-85. [ Links ]
36.Alves CRP, Ribeiro MMF, Melo EM, Araújo MG. Teaching leprosy: current challenges. An Bras Dermatol. 2014;89(3):454-9. DOI: http://dx.doi.org/10.1590/abd1806-4841.20142444 [ Links ]
 Correspondence:
Correspondence:
ghansfilho@hotmail.com
Manuscript received: December 2018
Manuscript accepted: July 2019
Version of record online: October 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}